
Abstract
Introduction
Poststroke hyperglycemia has been associated with unfavorable outcome. Several trials investigated the use of intravenous insulin to control hyperglycemia in acute stroke. This meta-analysis summarizes all available evidence from randomized controlled trials in order to assess its efficacy and safety.
Methods
We searched PubMed until 15/02/2013 for randomized clinical trials using the following search items: ‘intravenous insulin’ or ‘hyperglycemia’, and ‘stroke’. Eligible studies had to be randomized controlled trials of intravenous insulin in hyperglycemic patients with acute stroke. Analysis was performed on intention-to-treat basis using the Peto fixed-effects method. The efficacy outcomes were mortality and favorable functional outcome. The safety outcomes were mortality, any hypoglycemia (symptomatic or asymptomatic), and symptomatic hypoglycemia.
Results
Among 462 potentially eligible articles, nine studies with 1491 patients were included in the meta-analysis. There was no statistically significant difference in mortality between patients who were treated with intravenous insulin and controls (odds ratio: 1·16, 95% confidence interval: 0·89–1·49). Similarly, the rate of favorable functional outcome was not statistically different (odds ratio: 1·01, 95% confidence interval: 0·81–1·26). The rates of any hypoglycemia (odds ratio: 8·19, 95% confidence interval: 5·60–11·98) and of symptomatic hypoglycemia (odds ratio: 6·15, 95% confidence interval: 1·88–20·15) were higher in patients treated with intravenous insulin. There was no heterogeneity across the included trials in any of the outcomes studied.
Conclusions
This meta-analysis of randomized controlled trials does not support the use of intravenous insulin in hyperglycemic stroke patients to improve mortality or functional outcome. The risk of hypoglycemia is increased, however.
Keywords
Introduction
Hyperglycemia is a frequent finding in patients with acute stroke (1). Human and animal model studies have shown that it exerts a deleterious effect on the ischemic brain mediated by several pathophysiologic pathways (2). Glycemia in the acute phase of stroke has been shown to be an independent predictor of stroke outcome (3). In this context, several trials have tried to investigate whether glucose control with intravenous insulin infusion in acute stroke patients is associated with improved outcome; however, results have been inconclusive (4–13).
This meta-analysis summarizes all available evidence from randomized controlled trials of intravenous insulin in acute stroke patients in order to assess its efficacy and safety.
Methods
Search strategy and inclusion criteria
We searched PubMed for potentially eligible trials from 01/01/1966 to 15/02/2013. The search items were ‘intravenous insulin’ or ‘hyperglycemia’, and ‘stroke’. We also screened the references of related letters, editorials, reviews, and meta-analyses to identify potentially eligible studies. Eligible studies had to be randomized controlled trials of intravenous insulin in hyperglycemic patients with acute stroke, both blinded or not. This work was performed according to the PRISMA statement (14).
Outcomes and data extraction
The efficacy outcomes analyzed were mortality and functional outcome. The safety outcomes analyzed were mortality, any hypoglycemia (asymptomatic or symptomatic), and symptomatic hypoglycemia. For each outcome, sub-group analysis was also performed according to the control intervention (subcutaneous insulin or normal saline).
Data extraction was performed independently by two reviewers (G. N. and V. P.). For each outcome, the number of patients who were originally randomized to each treatment arm was extracted. In case that data were unavailable in the current publications, the trial investigators were contacted personally. Any uncertainty about the extracted data was resolved by consensus among the authors.
Statistical analysis
Data were analyzed in an intention-to-treat basis. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for each outcome using the Peto fixed-effects method. Heterogeneity between trials was assessed by the I2 index, which measures the percentage of the variability in effect estimates that is attributable to heterogeneity. All analyses were performed with the Review Manager (RevMan) version 5·1 (The Nordic Cochrane Centre, The Cochrane Collaboration, 2011, Copenhagen, Denmark).
Results
Among 462 potentially eligible publications that were identified in the literature, nine studies fulfilled our criteria and were included in the analysis (Fig. 1). Among 1491 patients included in these trials, 766 patients were allocated to intravenous insulin infusion and 725 formed the control group. The vast majority were patients with ischemic strokes with only 114 patients (7·6%) with primary intracerebral hemorrhage recruited in one trial (11).
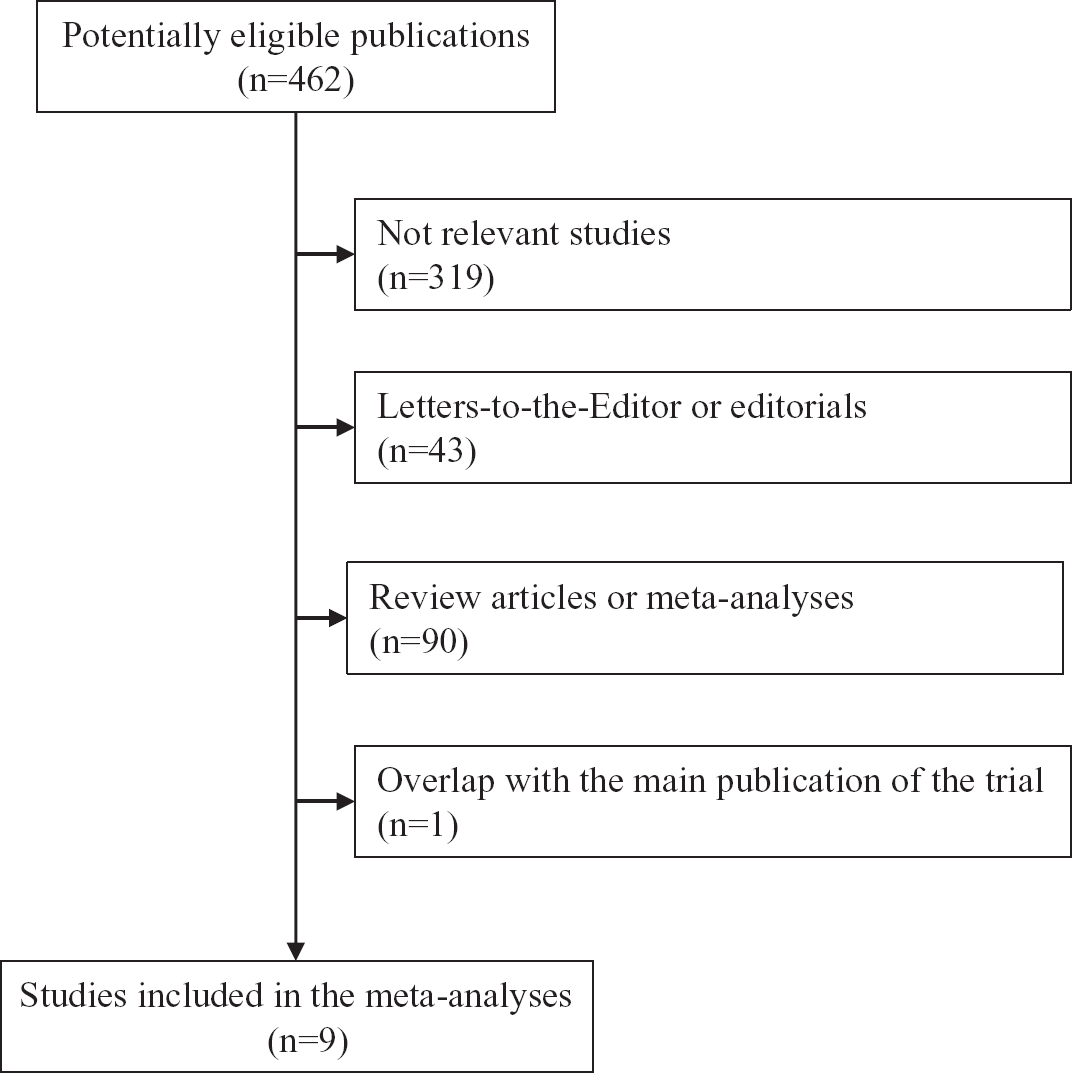
Flowchart of search and study selection strategy.
Various intravenous insulin regimens were used in the included studies: (a) 400 ml of 0·9% NaCl, 40 ml of 3% KCl, 10 ml of 25% magnesium sulfate and Farmasulin (Farmak, Ukraine) (13); (b) infusion of insulin (Human Actrapid, Novo Nordisk, Bagsværd, Denmark) with dosage adjustment according to a sliding scale (4); (c) 500 ml glucose-potasium-insulin regimen of 10% dextrose and 20 mmol potassium chloride with an initial insulin dose of 16 units of soluble recombinant human insulin (11); (d) 50 IU of actrapid insulin in 50 ml of 0·9% sodium chloride with an initial infusion dose of 2 IU/h (6); (e) 25 IU in 500 ml normal saline (5); (f) 50 IU normal insulin in 50 ml of 0·9% saline solution (9); (g) Novolin brand insulin in normal saline (1 U/1 ml) as a continuous infusion (10); (h) 500 ml of 10% dextrose, 20 mmol potassium chloride, and 16 units of soluble recombinant human insulin (8); and (i) soluble human Actrapid insulin was administered in an intravenous continuous infusion with hourly dose adaptation (7). The control group was treated with normal saline in three studies (4,8,11) or subcutaneous insulin in five studies (5–7,9,10). Various target glycemia levels were used: 3·9–6·1 mmol/l (10), 4–7 mmol/l (8,11), 4·4–6·1 mmol/l (9), 4·4–7 mmol/l (6), 5–7·2 mmol/l (5), 5–7·9 mmol/l (4), and < 7 mmol/l (7,13).
Favorable outcome was defined with the modified Rankin score in six studies (5–9,11) and the Barthel index in two studies (10,13). Favorable outcome and mortality were assessed at 1 (8,13), 3 (5–7,10,11), or 4 (9) months after stroke. Hypoglycemia was defined as a glucose value <4 mmol/l in two studies (8,11), <3·3 mmol/l in three studies (5,6,9), and <3 mmol/l in two studies (7,10).
In the analysis of mortality, there was no statistically significant difference in mortality between intravenous insulin and control intervention (OR: 1·16, 95% CI: 0·89–1·49) (Fig. 2). The effect of intravenous insulin was similar irrespectively of the control intervention (OR: 1·10, 95% CI: 0·59–2·07 compared with subcutaneous insulin and OR: 1·16, 95% CI: 0·89–1·49 compared with normal saline) (Fig. 2). Similarly, the rate of favorable outcome was not statistically different between intravenous intervention and control treatment (OR: 1·01, 95% CI: 0·81–1·26) (Fig. 3), independently of the type of the control intervention (OR: 1·20, 95% CI: 0·80–1·80 compared with subcutaneous insulin and OR: 0·90, 95% CI: 0·68–1·19 compared with normal saline) (Fig. 3).
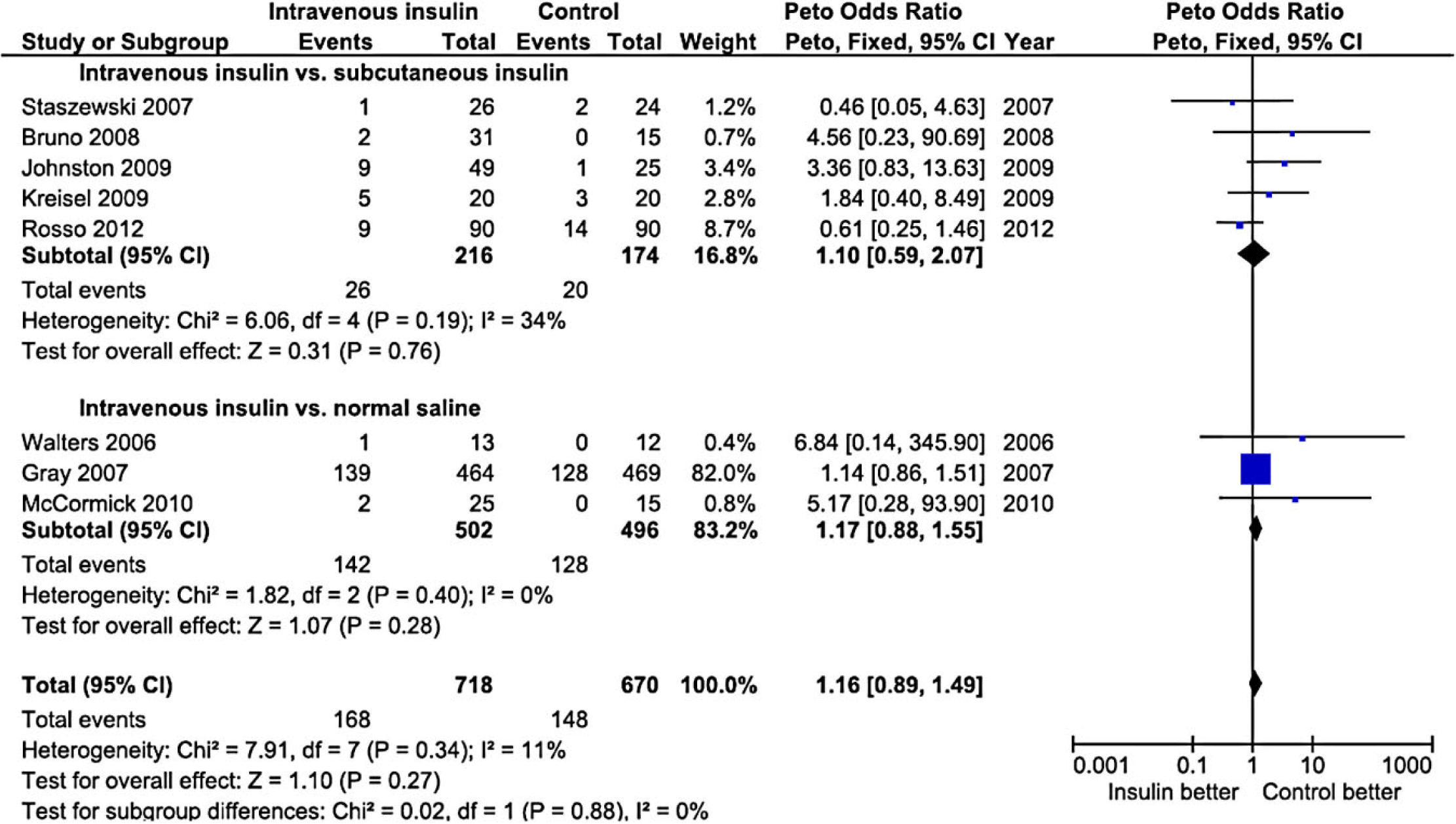
Forest plot of the effect of intravenous insulin vs. control on mortality.
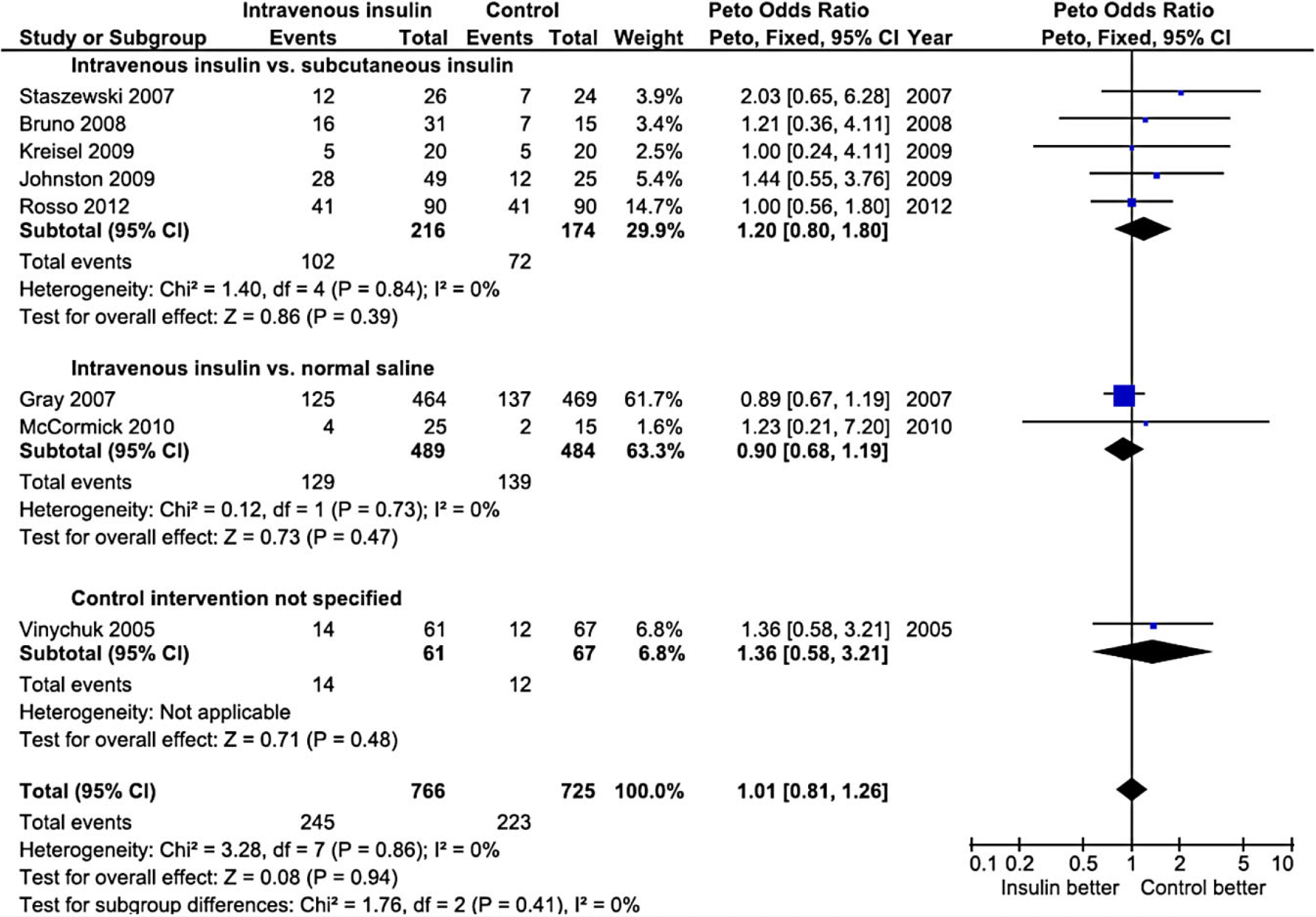
Forest plot of the effect of intravenous insulin vs. control on functional outcome.
In the analysis of the other safety outcomes, any hypoglycemia was more frequent in patients treated with intravenous insulin compared with any control treatment (OR: 8·19, 95% CI: 5·60–11·98), subcutaneous insulin (OR: 5·59, 95% CI: 2·67–11·71), or normal saline (OR: 9·40, 95% CI: 6·03–14·65) (Fig. 4). Similarly, the rate of symptomatic hypoglycemia was more frequent in patients treated with intravenous insulin compared with any control treatment (OR: 6·15, 95% CI: 1·88–20·15) and subcutaneous insulin (OR: 6·22, 95% CI: 1·68–23·01) but not compared with normal saline (OR: 5·85, 95% CI: 0·35–97·90) (Fig. 5).
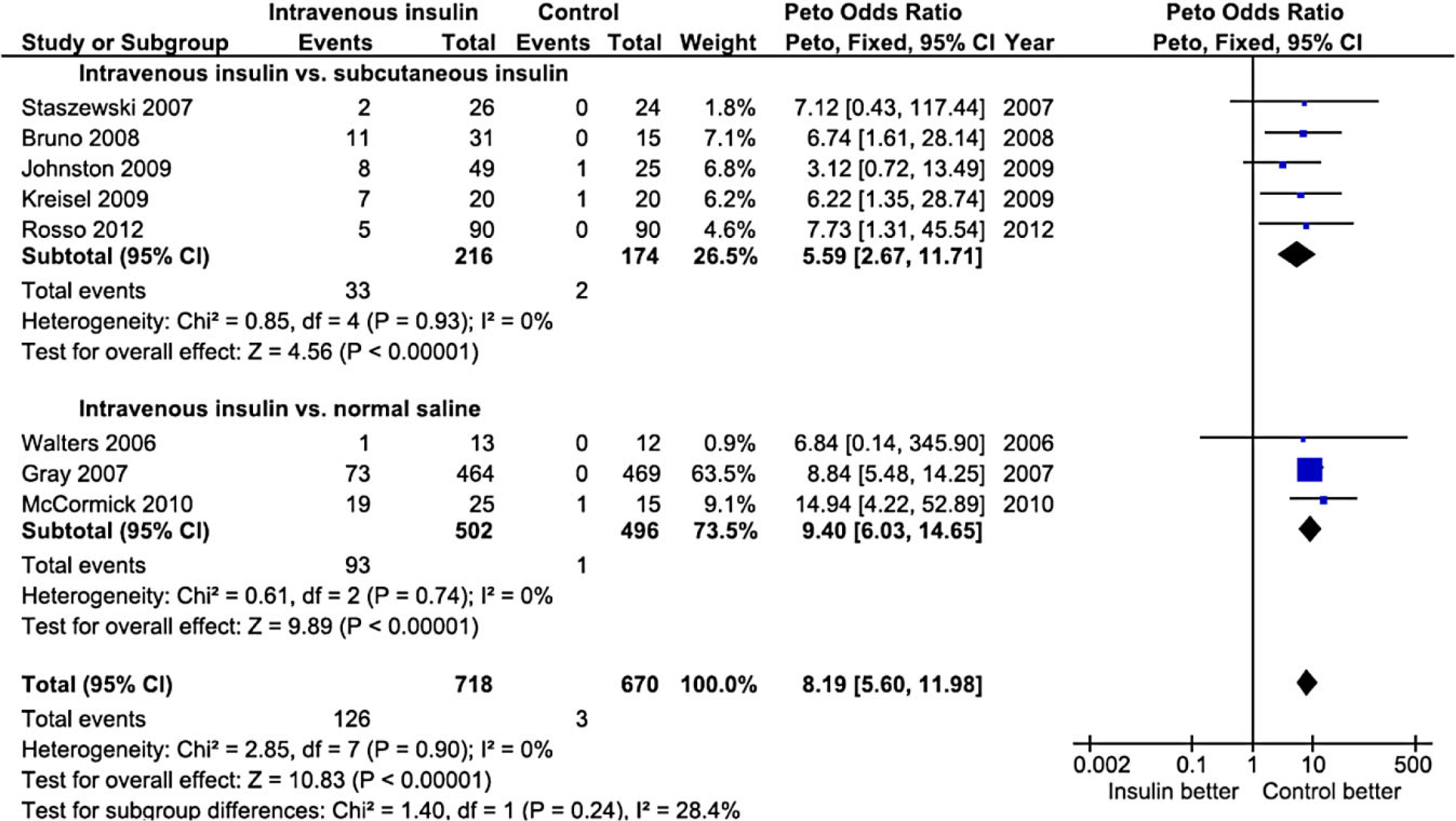
Forest plot of the effect of intravenous insulin vs. control on any hypoglycemia (symptomatic or asymptomatic).
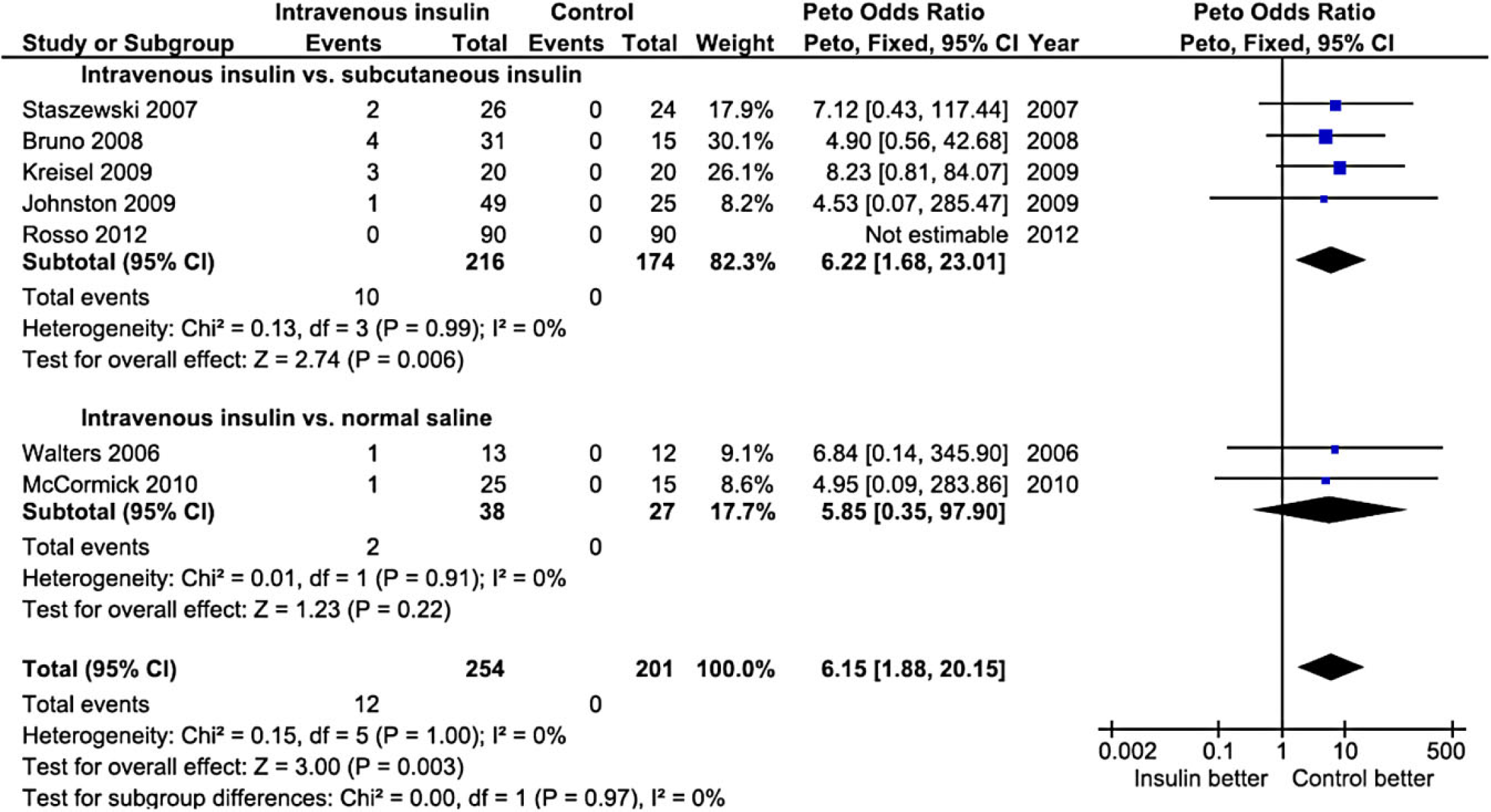
Forest plot of the effect of intravenous insulin vs. control on symptomatic hypoglycemia.
There was no significant heterogeneity across the included trials in all outcomes studied. In particular, the I2 index was 0% in the meta-analyses of functional outcome, hypoglycemia and symptomatic hypoglycemia and 11% in the meta-analysis of mortality.
Discussion
In this meta-analysis, we aimed to investigate the efficacy on mortality and functional outcome and the safety of intravenous insulin infusion in hyperglycemic patients with acute stroke. The results show that intravenous insulin infusion does not influence mortality or improve functional outcome; on the other hand, it is associated with higher rates of hypoglycemia.
Hyperglycemia is a frequent finding in patients with acute stroke (1). Several mechanisms account for this: first, preexisting abnormalities in glucose metabolism like diabetes mellitus, insulin resistance, or glucose intolerance is very prevalent in stroke patients (15). Second, a generalized stress reaction during the acute phase of stroke leads to stress hyperglycemia; this is mediated by multiple pathophysiologic pathways like activation of the hypothalamic-pituitary-adrenal axis and increased production of catecholamines, cortical, and glucagon, which promote gluconeogenesis, proteolysis, lipolysis, and insulin resistance (2). Third, this stress reaction results in release of several cytokines such as tumor necrosis factor and interleukins 1 and 6, which in turn enhance the generalized stress reaction and insulin resistance (2).
Human and animal model studies confirmed the deleterious effect of hyperglycemia in the ischemic brain mediated by several pathophysiologic pathways: impaired recanalization (due to increased thrombin–antithrombin complexes and downregulation of the plasminogen activator inhibitor), decreased reperfusion (due to reduction of nitric oxide levels accompanied by elevation of prostaglandin production), increased reperfusion injury (due to oxidative stress, promotion of the inflammatory response, and increased cytokine production), and direct tissue injury (mediated by mitochondrial dysfunction and lactic acidosis) (2). Indeed, clinical studies confirmed that poststroke hyperglycemia is associated with unfavorable outcome (16) and increases the bleeding risk after thrombolysis (17). In this context, several trials investigated the role of intensive glucose management with intravenous insulin to improve stroke outcome in a controlled, randomized fashion (4–12). The present meta-analysis summarizes these trials and shows that intravenous insulin does not influence mortality or functional outcome significantly after acute stroke. Therefore, this treatment applied in the current form, doses, and time window cannot be recommended for general use in hyperglycemic acute stroke patients.
The present study is limited by the inherent shortcomings of most meta-analyses: differences in the selection criteria among trials, variations in the definitions of hyper- and hypoglycemia, comorbidities and outcomes used in the trials, differences in the intensity, and monitoring of the intravenous insulin treatment and differences in the length of follow-up among trials. Additionally, in five of the included studies the control group was treated with subcutaneous insulin. This therapeutic modality might have resulted in favorable effects in the control group, attenuating the possibility to detect a significant difference. Moreover, the number of patients that were available and eligible for inclusion was relatively small, allowing for potential type 2 error, i.e. the erroneous nondetection of an effect of this treatment on mortality or functional outcome. Finally, there were insufficient data in the randomized trials to investigate whether occlusion status modifies the effect of intravenous insulin on infarct growth, as it was identified in the SELESTIAL trial in which insulin exacerbated infarct growth in patients with persistent arterial occlusion. This needs to be addressed in future trials (8).
The results of ongoing trials like the SHINE trial (18) may provide further insight into this controversial issue. Future trials may need to target specific populations such as patients with severe hyperglycemia, a significant amount of salvageable tissue, presence or absence of arterial occlusion (8) and recanalization treatment, treated at earlier time windows, and avoid potentially deleterious hypoglycemia that might increase mortality in these patients (16). Pending the results of such trials, the present meta-analysis suggests that the generalized use of intravenous insulin in hyperglycemic acute stroke patients does not seem to reduce mortality or improve functional outcome.