
Abstract
Background
Treatment rates with intravenous tissue plasminogen activator vary by region, which can be partially explained by organizational models of stroke care. A recent study demonstrated that prehospital factors determine a higher thrombolysis rate in a centralized vs. decentralized model in the north of the Netherlands.
Aim
To investigate prehospital factors that may explain variation in thrombolytic therapy between a centralized and a decentralized model.
Methods
A consecutive case observational study was conducted in the north of the Netherlands comparing patients arriving within 4·5 h in a centralized vs. decentralized stroke care model. Factors investigated were transportation mode, prehospital diagnostic accuracy, and preferential referral of thrombolysis candidates. Potential confounders were adjusted using logistic regression analysis.
Results
A total of 172 and 299 arriving within 4·5 h were enrolled in centralized and decentralized settings, respectively. The rate of transportation by emergency medical services was greater in the centralized model (adjusted odds ratio 3·11; 95% confidence interval, 1·59–6·06). Also, more misdiagnoses of stroke occurred in the central model (P = 0·05). In postal code areas with and without potential preferential referral of thrombolysis candidates due to overlapping catchment areas, the odds of hospital arrival within 4·5 h in the central vs. decentral model were 2·15 (95% confidence interval, 1·39–3·32) and 1·44 (95% confidence interval, 1·04–2·00), respectively.
Conclusions
These results suggest that the larger proportion of patients arriving within 4·5 h in the centralized model might be related to a lower threshold to use emergency services to transport stroke patients and partly to preferential referral of thrombolysis candidates.
Introduction
Treatment with intravenous tissue plasminogen activator (tPA) is the only proven treatment for patients with acute ischemic stroke if started within 4·5 h (1–3). However, treatment rates with tPA in acute ischemic stroke vary considerably by region (4,5). The reasons for this variation are largely unknown. Different organizational models of acute stroke care have been suggested as explanatory variables.
We previously demonstrated a 50% greater likelihood of tPA treatment in a centralized vs. decentralized model of acute stroke care (6). In this study, the centralized model consisted of four hospitals, in which tPA treatment was only provided in University Medical Centre Groningen (UMCG), acting as a regional stroke center. The decentralized model consisted of nine general hospitals each providing tPA treatment for patients in their catchment area. The centralized model yielded a larger proportion of patients presenting to the Emergency Department (ED) within the 4·5 h time window (onset-to-door). Thus, more patients were eligible for thrombolytic therapy in the centralized model based on prehospital factors.
Aim
The aim of this study was to investigate which prehospital organizational factors determine this benefit of the centralized model.
Methods
Study design and setting
We performed a consecutive case observational study in the north of the Netherlands. The centralized model consisted of four hospitals in which thrombolysis is provided by the UMCG, acting as stroke center. Within its catchment area, arrangements were made with general practitioner (GP) offices and emergency medical services (EMS) to transport suspected stroke patients potentially eligible for thrombolysis to the UMCG, thereby bypassing community hospitals that may be located closer to the patient. The centralized stroke model served an approximate population of 0·58 million inhabitants with a population density of 250 inhabitants/km2. The decentralized model consisted of nine community hospitals all treating patients with thrombolysis within their own catchment area. The decentralized model served a population of 1·14 million inhabitants with a population density of 190 inhabitants/km2. Distances and access to health-care services, such as the GP and EMS were comparable for both models (7).
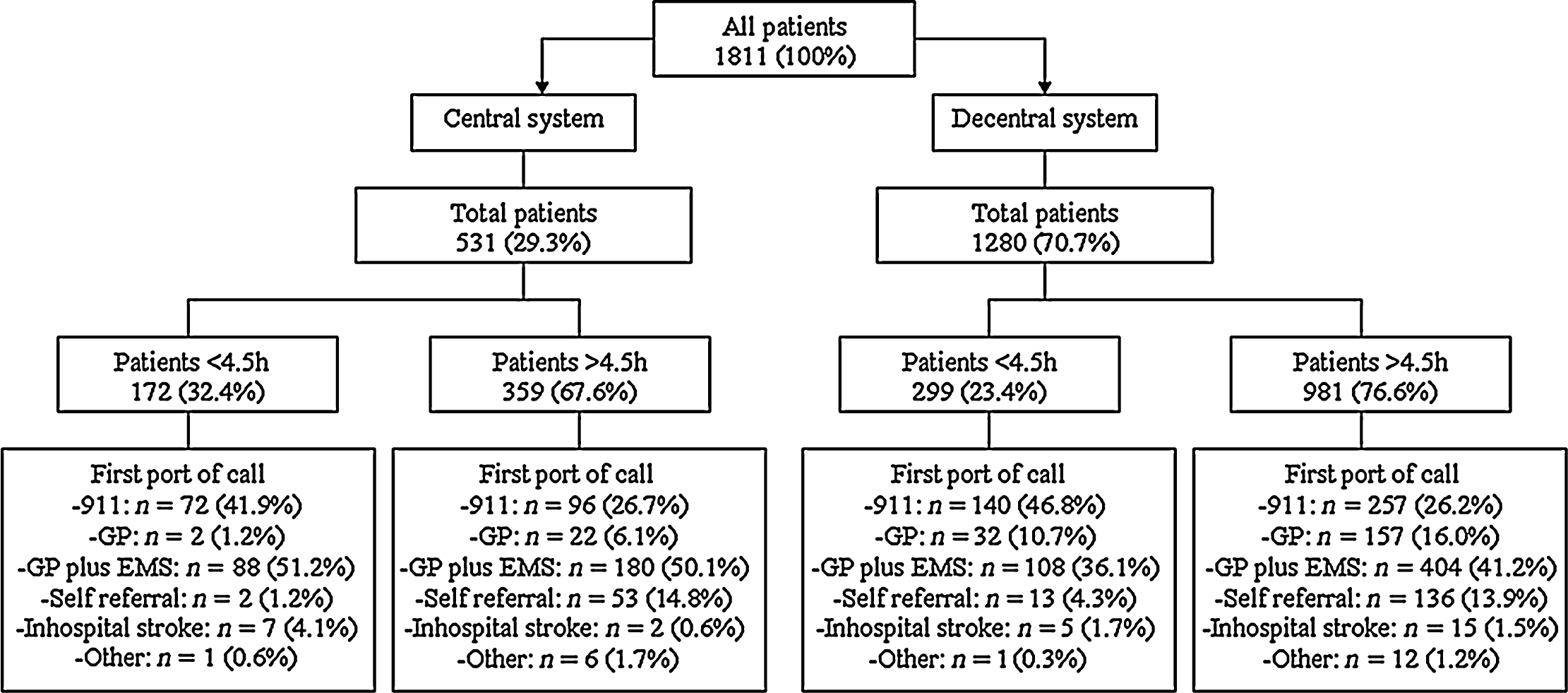
In this study we focused on assessing prehospital organizational factors across patients arriving at the hospital within 4·5 h, regardless of the final hospital discharge diagnosis. This means that, as opposed to a previous publication in which we focused on ischemic stroke patients (6), those patients suffering from transient ischemic attack (TIA), hemorrhage, and alternative diagnoses were also included in the current analysis (Fig. 1). We also expanded the study period to August 30, 2010.
GP, general practitioner; EMS, emergency medical services.
Selection of participants
Inclusion criteria included patient age 18 years and older who presented to the GP, EMS, or the ED from February 1 to August 30, 2010, and who were triaged as a possible stroke victim. Recurrent strokes were considered eligible for study enrollment. No limitations were made for upper age limits based on experiences in our setting and others (8,9).
Data collection
Identical protocols for tPA treatment (adjusted European Cooperative Acute Stroke Study III (10)), identification and triage of suspected stroke patients, and 911 systems were used in both models. Prehospital data were gathered by ambulance personnel using a survey containing 16 data fields that were completed for each suspected stroke patient they transported. Hospital data were gathered upon ED arrival for all suspected stroke patients by the neurologist on call using a survey containing 28 items. Identical surveys were used by all EMS systems and hospitals participating in this study. All information was entered electronically into a central database by either the stroke neurologist, stroke nurse, or the principal investigator (M. L.). Identical stroke guidelines (11) and EMS protocols were available for GP offices and for dispatch (12) and ambulance personnel (13). In case of possible candidacy for tPA treatment high priority transport was assigned, defined as a normative value of 15 min between 911 call and ambulance arrival at the location of the patient. Both ambulance personnel and the GP (either by telephonic or visit) used the Face Arm Speech Test (14) as stroke identification tool. Hospital prenotification of the ED was performed in both models. National public campaigns about stroke symptoms and how to act were similar in both models.
Outcome measures
Factors investigated were: (1) time from stroke onset to call for help, (2) mode of referral, i.e. via EMS (911 call), via GP and subsequent self-transport, via GP and subsequent EMS transport or self-transport to hospital, (3) mode of transportation and high prioritization, (4) prehospital diagnostic accuracy, and (5) preferential referral of tPA candidates.
Prehospital diagnostic accuracy was determined by comparing EMS triage stroke diagnosis to the hospital discharge diagnosis.
In postal code areas, where strokes victims might be routed through both organizational models preferential referral of potential tPA candidates to one particular model may be considered a selection bias (15). Therefore, we calculated the odds ratio (OR) of presenting in hospital with a stroke within 4·5 h for centralized vs. decentralized care. These ORs were compared between a group of postal code areas with more than 90% of all stroke patients referred to one predominant model of care and postal code areas with a choice of models (<90% of patients in one model). We assumed that in postal code areas that refer (>90% of cases) within one model, the proportion of potential tPA candidates among all stroke patients is a model characteristic not influenced by selection bias.
Statistical analysis
Mann–Whitney U, Fisher's exact tests, and ORs were calculated for continuous and categorical variables in both organizational models. Odds ratios were adjusted for baseline characteristics age, gender, and the short version of the National Institutes of Health Stroke Scale (16) using logistic regression. All factors with P < 0·10 in the univariate analysis were entered into the final model.
Informed consent and study approval
Informed consent was obtained from all subjects participating in this study. The study was approved by the institutional review board of the UMCG.
Results
Characteristics of study subjects
A total of 471 patients arriving at the hospital within 4·5 h were enrolled in the study, 172 in the centralized vs. 299 in the decentralized model. Three patients suffered a recurrent stroke during the study period. Figure 1 shows the distribution of the patients across both settings. Within the centralized model, 126 (73·2%) suffered ischemic stroke, 11 (6·4%) TIA, 13 (7·6%) intracranial hemorrhage, and 22 (12·8%) were diagnosed with a disease other than stroke. The leading final discharge diagnoses for the 22 patients with alternative diagnosis in the centralized model included: epilepsy or seizure (n = 6), migraine (n = 5), functional or medically unexplained symptoms (n = 5), infection (n = 3), altered level of consciousness (n = 1), and other (n = 2). Mean age was 67·5 years, and 90 (52·3%) were women. In the decentralized model, 237 (79·3%) suffered ischemic stroke, 9 (3·0%) TIA, 38 (12·7%) intracranial hemorrhage, and 15 (5·0%) were diagnosed with a disease other than stroke. The 15 patients with alternative diagnosis in the decentralized model included: epilepsy or seizure (n = 5), functional or medically unexplained symptoms (n = 3), malignancy (n = 2), migraine (n = 1), vertigo (n = 1), delirium (n = 1), and other (n = 2). Mean age was 71·3 years, and 135 (45·3%) were women. Table 1 describes the baseline characteristics and Table 2 outcome measures for this subset of patients.
Baseline characteristics patients <4·5 h
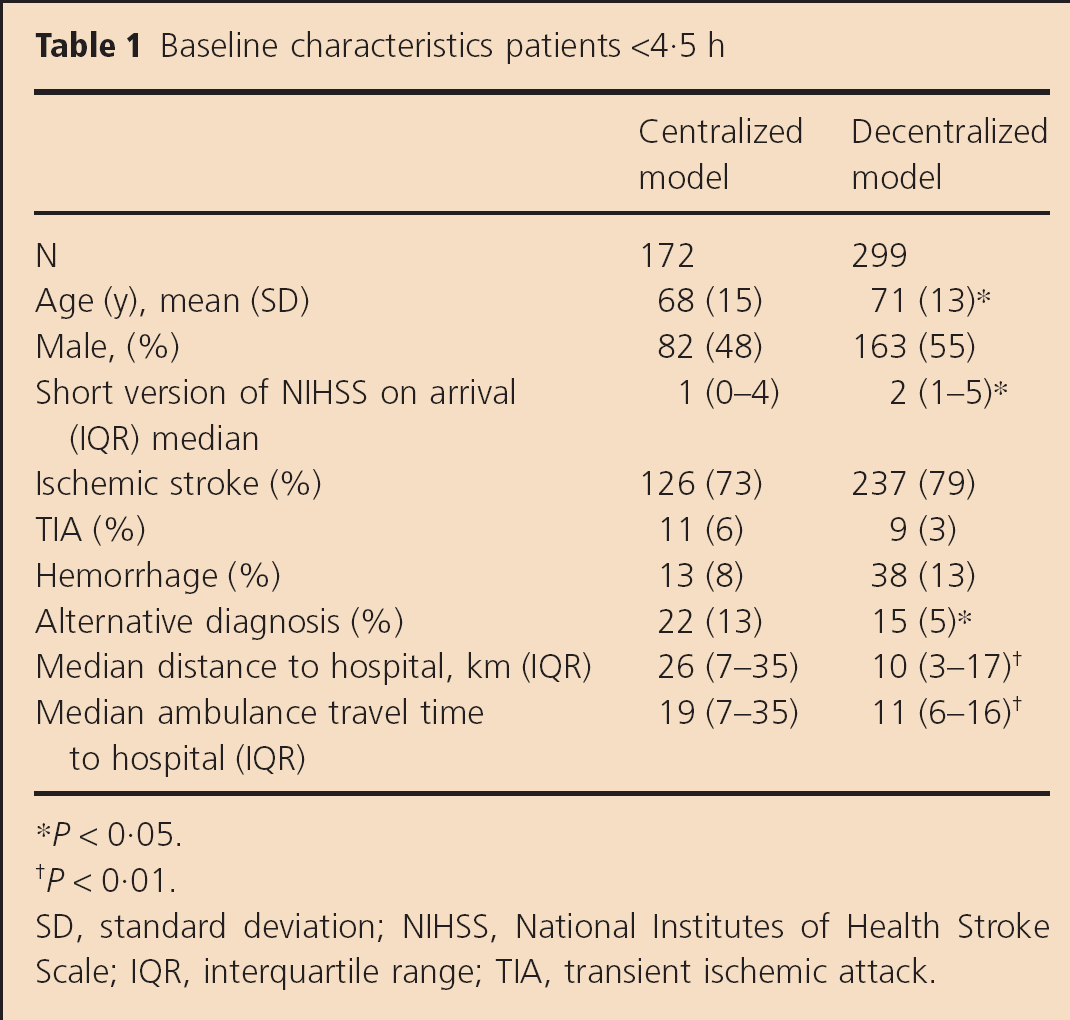
P < 0·05.
P < 0·01.
SD, standard deviation; NIHSS, National Institutes of Health Stroke Scale; IQR, interquartile range; TIA, transient ischemic attack.
Outcome measures patients <4·5 h
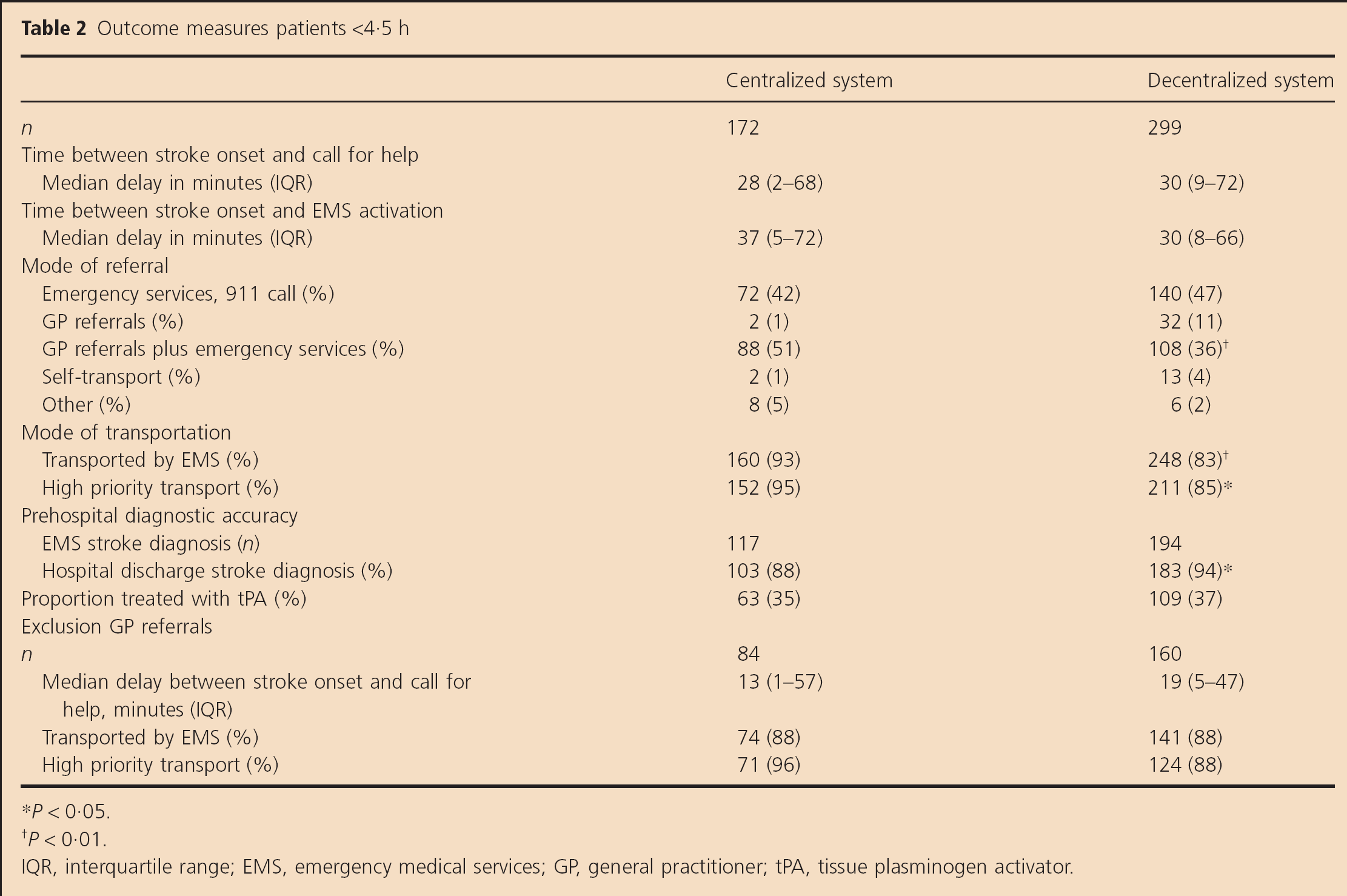
P < 0·05.
P < 0·01.
IQR, interquartile range; EMS, emergency medical services; GP, general practitioner; tPA, tissue plasminogen activator.
Main results
In the centralized model, 172 of 531 patients (32·4%) arrived within 4·5 h after stroke onset compared with 299 of 1280 (23·4%) in the decentralized setting [adjusted OR 1·96; 95% confidence interval (CI) 1·51–2·53].
For those patients arriving within 4·5 h, the median patient delay from symptom onset to call for help was 28 min (interquartile range, 2–68) in the centralized model vs. 30 min (interquartile range, 9–72) in the decentralized model (P = 0·16). Comparing centralized to decentralized care, referral via 911 occurred in 41·9% vs. 46·8% (adjusted OR, 0·85; 95% CI, 0·56–1·28), referral by GP followed by self transport in 1·2% vs. 10·7% (adjusted OR, 0·08; 95% CI, 0·02–0·35), GP plus EMS transport in 51·1% vs. 36·1% (adjusted OR, 2·02; 95% CI, 1·33–3·06), and self-transport in 1·2% vs. 4·3% (OR, 0·26; 95% CI, 0·06–1·16), respectively. Transportation by ambulance occurred in 93·0% in the centralized model vs. 82·9% in the decentralized model (adjusted OR, 3·11; 95% CI, 1·59–6·06). High priority transportation occurred in 95·0% vs. 85·1%, respectively (adjusted OR, 3·67; 95% CI, 1·65–8·17). Of all patients triaged by EMS as stroke, 88·0% actually had a stroke in the centralized model vs. 94·3% in the decentralized model (P = 0·05). In regions with and without possible preferential referral, the ORs for hospital arrival within 4·5 h for centralized vs. decentralized care were 2·15 (95% CI, 1·39–3·32) and 1·44 (95% CI, 1·04–2·00), respectively (P < 0·01).
Discussion
This study demonstrated that prehospital factors in patients potentially eligible for tPA treatment differed between a centralized and decentralized acute stroke care model. The results of this study suggest a greater use and lower threshold to transport, prioritize, and refer patients potentially eligible for tPA treatment in the centralized model.
The results showed no difference between models for the time from stroke onset to call for help. Within the centralized model there was a higher rate of (1) EMS transportation of stroke patients both in the overall study population and for those referred by the GP, and (2) high priority EMS transportation. The increased use of EMS in the centralized model may have shortened prehospital delay in this group and led to a larger proportion of patients arriving within 4·5 h (17,18). This may explain part of the variation in tPA use between both models. The need to transport patients to more distant centers in the centralized system might have provoked the more frequent use of EMS (i.e. patients to be cared for at nearby hospitals might reasonably be more likely to use private or other transport than those to be cared for at more distant hospitals). Because not all patients arriving within 4·5 h were assigned high priority transport (i.e. 95% in the centralized and 85% in the decentralized model), there is still room for improvement regarding the education of EMS providers in both models. Importantly, travel times and distances were significantly longer in the centralized model, and hence could not have contributed to the difference in the proportion of patients arriving quickly. Less severe strokes were observed in the centralized model, possibly reflecting a lower threshold of EMS services to transport potential stroke victims. Despite comparable stroke recognition tools and transport protocols for EMS systems, the threshold to transport, prioritize, and refer patients potentially eligible for tPA treatment differed between both models. Possible explanations for this difference may include the presence of a stroke champion in the centralized model, who actively promotes rapid identification and transport of potential stroke victims among GPs, EMS dispatchers, and ambulance personnel.
Analysis of patients arriving outside the 4·5 h time window showed an identical mode of referral between models. However, in both models patients arriving outside 4·5 h were more often triaged by the GP, and less often called 911. Notably, this appears to suggest that raising public awareness to call 911 in response to stroke symptoms might result in earlier presentation at the hospital and increased tPA use, as demonstrated in other studies (19).
More misdiagnoses by EMS were observed in the centralized model. This may suggest a more liberal referral policy of EMS. However, this policy may also lead to higher proportions of patients eligible for tPA treatment. Further cost-effectiveness studies are needed to evaluate this liberal policy of EMS services. The proportion of cerebral emergencies that ultimately did not appear to be an ischemic stroke, particularly TIA, did not differ across organizational models. This category of patients, however, does imply that emergency services have to be well trained and alert to perform adequate triage.
The analyses on preferential referral showed that, in regions where more than 90% of patients were referred to one predominant model of care, patients were one and a half times as likely to present in hospital within 4·5 h in the centralized setting. This may be the result of a combination of experience and exposure to tPA, continuing medical education and new trainees entering into the workforce (20). In regions where both models coexisted and competed for stroke patients, a preference for the central model was revealed. This may be due to the EMS recognizing the UMCG and its stroke team as actively promoting thrombolysis and always available, resulting in preferential hospitalization of thrombolysis candidates (21). The causes for this selection preference deserve further study, as this preference may ultimately affect further implementation efforts.
There are several study limitations. First, the subgroup analysis concerning preferential referral was only defined a posteriori and cannot definitively refute or confirm preferential referral. Nonetheless, it is a novel explorative analysis that gives a good indication of the impact a selection preference may have had on the results of the comparative cohort study and addresses concerns that were raised in the literature (15). Also, it may allow a more accurate estimation of the gains to be made by reorganizing acute stroke care. Second, because only suspected stroke victims were investigated, and not all patients, transported by ambulance to the participating hospitals during the study period, we were unable to estimate the total number of true and false negative triages. Finally, it cannot be excluded that prehospital factors not identified in this study may partly explain some of the differences between the models. Specifically, nonorganizational prehospital factors such as demographic and other patient characteristics including race ethnicity, educational level, facial droop, comorbidity, living status, and risk factors for stroke such as diabetes or a history of heart failure (22) lay outside the scope of this study and were therefore not included in the analysis. Demographic studies of the adherence areas, however, did not reveal any relevant differences across respective catchment areas (23).
In summary, lower threshold for use of EMS and high priority transport of potential stroke patients, and partly a preferential referral of potential tPA candidates to a centralized organizational model were identified as prehospital factors contributing to variation in tPA use. These factors warrant further concerted action to improve acute stroke care.
Footnotes
Acknowledgements
We wish to express our gratitude to all participating hospitals, emergency medical services, and general practitioner out of hours co-op for providing data for this study: S. Schade van Westrum, MD, Martini Hospital Groningen, the Netherlands; K. M. Horvath, MD, PhD, Refaja Hospital Stadskanaal, the Netherlands; A. van As, MD, Ommelander Hospital Group, Location Delfzicht Delfzijl, the Netherlands; C. Felisiak, MD, Ommelander Hospital Group, Location Lucas Winschoten, the Netherlands; W. J. Schuiling, MD, PhD, Medical Centre Leeuwarden, the Netherlands; R. F. Duyff, MD, Hospital The Tjongerschans Heerenveen, the Netherlands; K. Beintema, MD, Hospital Nij Smellinghe Drachten, the Netherlands; A. M. H. P. Boreas, MD, PhD, Antonius Hospital Sneek, the Netherlands; G. Sulter, MD, PhD, Hospital Sionsberg Dokkum, the Netherlands; J. N. Wessel, MD, Wilhelmina Hospital Assen, the Netherlands; L. Koops, MD, and J. Trip, MD, Diaconessen Hospital Meppel, the Netherlands; C. de Langen, MD, and P. Oomes, MD, Bethesda Hospital Hoogeveen, the Netherlands; R. de Vos, MD, Emergency Medical Services Groningen, the Netherlands; T. Sandjer, MD, Emergency Medical Services Drenthe and Friesland, the Netherlands; R. Kijlstra, Emergency Medical Services Friesland, the Netherlands; J. Post, MD, PhD, General Practitioner Out Of Hours Co-op Groningen, the Netherlands.
Netherlands Organisation for Health Research and Development (ZonMw). Ref: 80-82800-98-104.
None.