
Abstract
Background and purpose
We aimed to investigate the association of statin treatment with outcomes in patients with acute ischemic stroke.
Methods
Over a 4.5-year period (starting November 2007), 12 781 patients (mean age, 72·8 ± 12·6 years; 48·6% women) with acute ischemic stroke from 15 hospitals in Schleswig-Holstein, Germany, were enrolled in a population-based study and prospectively evaluated.
The primary outcomes were the mortality during hospitalization and the disability (modified Rankin Scale score ≥2) at discharge from hospital. The secondary outcomes were the mortality and disability at three-months after discharge.
Results
A total of 7535 patients (59%) with acute ischemic stroke were treated with statins. During hospitalization (mean, nine-days), the in-hospital mortality rate (4·7%; 95% confidence interval, 4·3–5·1%) was lower in patients treated with statins than in those without statins (2·3% vs. 7·9%, respectively; P < 0·001). At three-months after discharge, the mortality rate (6·9%; 95% confidence interval, 6·4–7·5%) was lower in patients treated with statins than in those without statins (5·0% vs. 10·6%, respectively; P < 0·001). Adjusted logistic regression analysis showed that statin treatment was associated with reduced rates of in-hospital mortality (odds ratio, 0·39; 95% confidence interval, 0·31–0·48; P < 0·001) and three-month mortality (odds ratio, 0.47; 95% confidence interval, 0·34–0·63; P < 0·001). A comparison of the patient groups revealed that patients on statins were likely to have lower disability rates at discharge (59% vs. 67%, respectively; P < 0·001) and after three-months (33% vs. 42%, respectively; P < 0·001) in patients who had survived the stroke.
Conclusion
Statin treatment may improve the outcomes in patients with acute ischemic stroke. Further studies are necessary to confirm this finding.
Introduction
Stroke-related death and disability will rise as a consequence of an increase in stroke incidence. The occurrence of stroke has severe consequences for patients, their family members, and society. These consequences include the loss of patient independence, higher costs of care, and loss of individual productivity (1). The rates of stroke occurrence and stroke death depend on ethnicity, gender, and income status of countries (2,3). To date, recombinant tissue-plasminogen activator is the only approved medical therapy for acute ischemic stroke (AIS) that improves patient outcomes (4). Other medical options for treating ischemic stroke are not available for clinical daily use.
Clinical studies have shown that the administration of cholesterol-lowering 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors (statins) prevents stroke and cardiovascular events in individuals (5–7). Research has also suggested that pretreatment with statins may reduce in-hospital mortality in patients suffering from AIS (8). Other randomized studies investigating the impact of statins have revealed their beneficial effects on stroke and total mortality, most notably a decrease in cerebrovascular disease mortality (9). In addition, research has revealed that the administration of statin immediately after stroke (≤72 h) may improve stroke outcomes (10). Therefore, international guidelines recommend that patients suffering from AIS should be treated with statins for secondary prevention that may be due to pleiotropic effects and low-density lipoprotein-lowering effects (11).
We decided to investigate the association between the statin treatment and the stroke outcomes in patients suffering from AIS.
Methods
Study population
The Quality Association for Acute Stroke Treatment in Schleswig-Holstein (QugSS2) is an ongoing population-based cohort study on stroke in Schleswig-Holstein, a German state with 2·8 million inhabitants. The QugSS2 study, which began in 2007, includes all hospitals involved in treating patients with cerebrovascular diseases. The 15 sites involved in the present study included two university departments of neurology, eight departments of neurology at nonuniversity hospitals, and five departments of internal medicine at nonuniversity hospitals. Approval for the study was obtained from the local ethics committee of the University of Lübeck. The inclusion in the stroke registry is part of the quality assessment program for stroke treatment in Schleswig-Holstein. The entry in the stroke registry is obligatory. A written consent form was required for the inclusion in the three-month follow-up questionnaire.
The primary outcomes were in-hospital mortality and disability [defined here as a modified Rankin Scale (mRS) score ≥2] at discharge from hospitals. The secondary outcomes were the mortality and disability at three-months after discharge. During hospitalization, the occurrence of a recurrent stroke and symptomatic intracerebral hemorrhage were included in the secondary outcomes. The symptomatic intracerebral hemorrhage was defined as bleeding that was detected by computed tomography scan that was not seen on initial investigation and was associated with clinical worsening [National Institutes of Health Stroke Scale (NIHSS) ≥ 4 points].
The three-month mortality did not include the in-hospital mortality, and mRS equal to 6 (death) was not included in the disability at discharge and at three-months later.
Hypercholesterolemia (HCH) was diagnosed when the value of the fasting cholesterol was greater than 200 mg/dl at the time of the acute stroke in patients who were newly diagnosed with HCH. In addition, prior records and historical data about the presence of HCH were taken into during the diagnostic evaluation of HCH.
The statin treatment was performed during the hospitalization after admission in patients with AIS who were not treated with statin before. In accordance to the protocol of QugSS2, the statin treatment should be performed after the value of fasting cholesterol was measured, ideally within 24 h of admission in stroke patients with newly diagnosed HCH. Statin treatment was also initiated as a secondary prophylaxis in stroke patients with evidence of stenosis of brain-supplying arteries and in patients with microangiopatic stroke.
Furthermore, statin treatment was administrated for plaque stabilization in patients with AIS when plaques were seen in the carotid bifurcation using the duplex sonography. The treating physician or neurologist determined the indication for statin treatment.
Data acquisition
From November 2007 through March 2012, all patients suffering from AIS who are over the age of 18 years and reside in Schleswig-Holstein (one of the 16 States in Germany) are entered into the stroke registry (QugSS2). The inclusion criteria for patients in the present population-based study were a diagnosis of AIS (characterized in accordance with the definition put forth by the World Health Organization), main residence in Schleswig-Holstein, and admission to hospital. The exclusion criteria for patients were age under 18 years and a diagnosis of intracerebral hemorrhage, transient ischemic attack, or subarachnoid hemorrhage.
The follow-up evaluation was three-months after discharge. Patients were questioned by letter and/or telephone interview. When patients did not respond to the letter and could not be contacted, we evaluated the mortality at three-months after discharge by making an online request to the registration office of the German federal state of Schleswig-Holstein. If patients changed their address during the follow-up period of three-months after discharge, were no longer residing in the state of Schleswig-Holstein, and could not be contacted by telephone, they were considered lost to follow-up.
Statistical analysis
Data were analyzed with Statistical Product and Service Solutions software (version 20; IBM SPSS Statistics, Armonk, NY, USA). Data were described with mean and standard deviation (SD) values for continuous variables, absolute numbers and percentages for categorical variables, and median and interquartile range (IQR) values for ordinal variables. A chi-square test to determine the correlation between categorical variables, a t-test to compare continuous variables, and a Mann–Whitney U-test to compare ordinal variables were performed. Adjusted logistic regression analysis was carried out to estimate the odds ratio (OR). All variables of clinical parameters that were associated with outcomes (mortality and disability) with P less than 0·1 were entered into the logistic regression model (Tables 2 and 3). A P value of less than 0.05 was considered significant.
Results
A total of 12 781 patients (mean age, 72·8 ± 12·6 years; 48·6% women; median NIHSS score, 4 [IQR: 2–9]) were diagnosed with AIS and entered into the stroke registry for the German federal state of Schleswig-Holstein. All patients were investigated over a period of 4·5 years (starting November 2007 through March 2012) in a population-based study. The frequencies of brain imaging investigations were 95% by cranial computed tomography scan and 53·4% by magnetic resonance imaging.
Medical treatment with statin drugs was administered to 7535 patients (59%) before hospital admission and/or early after stroke during hospitalization. A comparison between patients treated with statins and those not treated with statins is shown in Table 1.
Baseline characteristics and comparison between patients with statins vs. without statins
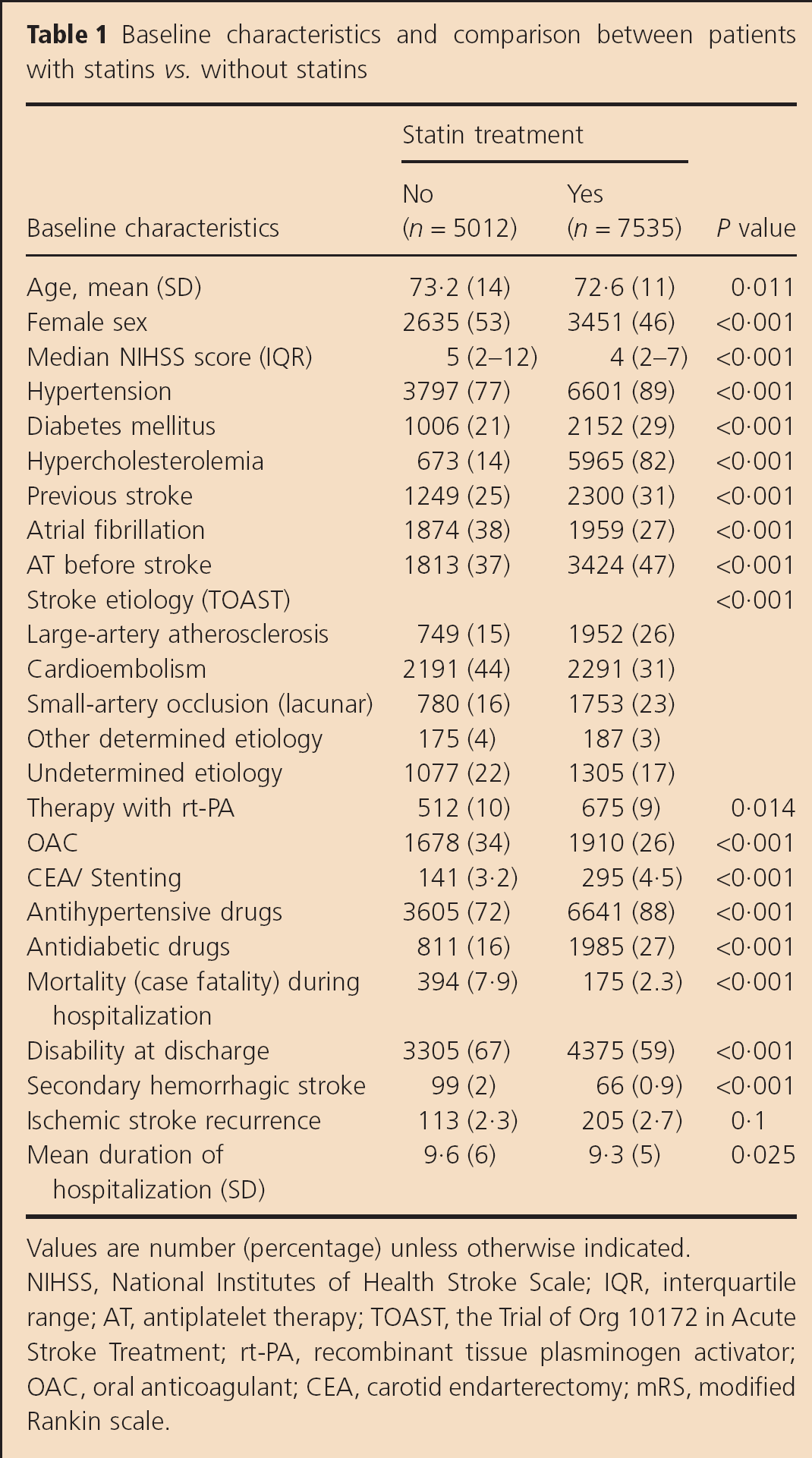
Values are number (percentage) unless otherwise indicated.
NIHSS, National Institutes of Health Stroke Scale; IQR, interquartile range; AT, antiplatelet therapy; TOAST, the Trial of Org 10172 in Acute Stroke Treatment; rt-PA, recombinant tissue plasminogen activator; OAC, oral anticoagulant; CEA, carotid endarterectomy; mRS, modified Rankin scale.
Of 12 781 patients, 596 [4·7%; 95% confidence interval (CI), 4·2–5·1%] died during a mean hospital stay of nine-days (SD, 5·5) after onset of AIS. In the population, the rate of in-hospital mortality was lower in patients who were treated with statins compared with those who were not treated with statins (2·3% vs. 7·9%, respectively; P < 0·001) (Fig. 1). At discharge from acute care hospitals, the rate of disability (defined as mRS score ≥2) was significantly lower in patients treated with statins compared with those without statins (59·2% vs. 67·4%, respectively; P < 0·001) (Fig. 2).
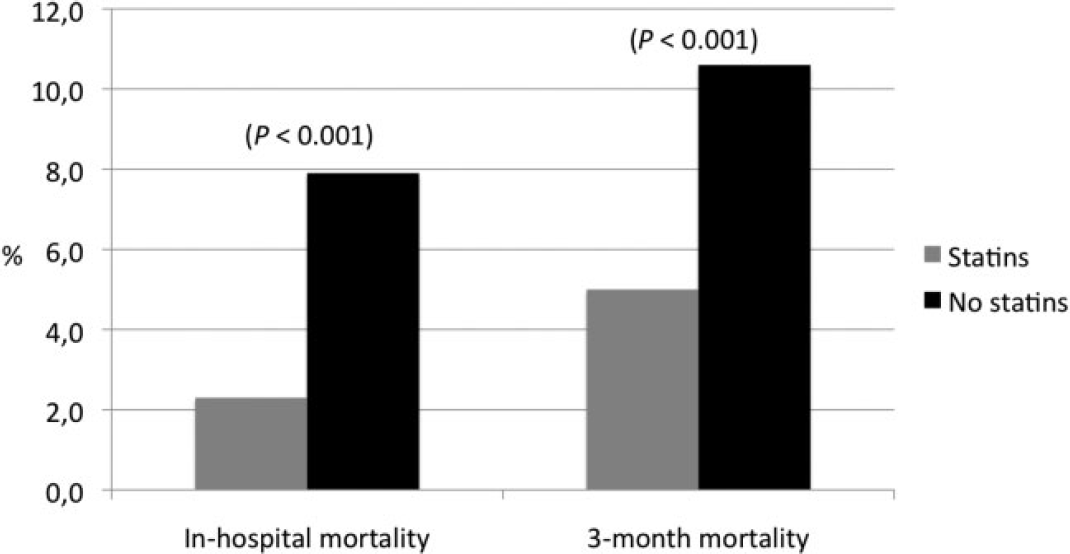
In-hospital mortality and three-month mortality in patients treated with statins vs. those without statins. Mortality recorded in percent. Differences between groups, P < 0·001.
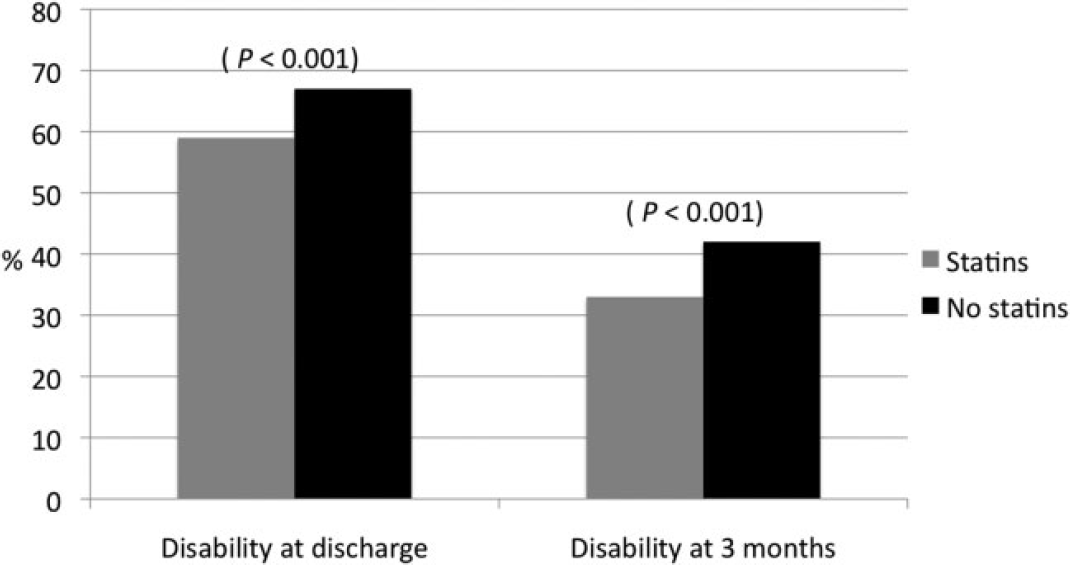
Disabiltiy (mRS ≥ 2) at discharge and three-months after discharge in patients with statins vs. those without statins. Disability recorded in percent. Differences between groups, P < 0·001.
Adjusted logistic regression analysis (Table 2) revealed that the administration of statin medication was associated with a reduction in the rate of in-hospital mortality [odds ratio (OR), 0·39; 95% CI, 0·29–0·52; P < 0·001] and in disability at discharge in patients treated with statins (OR, 0·8; 95% CI, 0·6–0·78; P < 0·001) in patients who survived the stroke.
Baseline characteristics and association with outcomes in the unilateral analyses and logistic regression
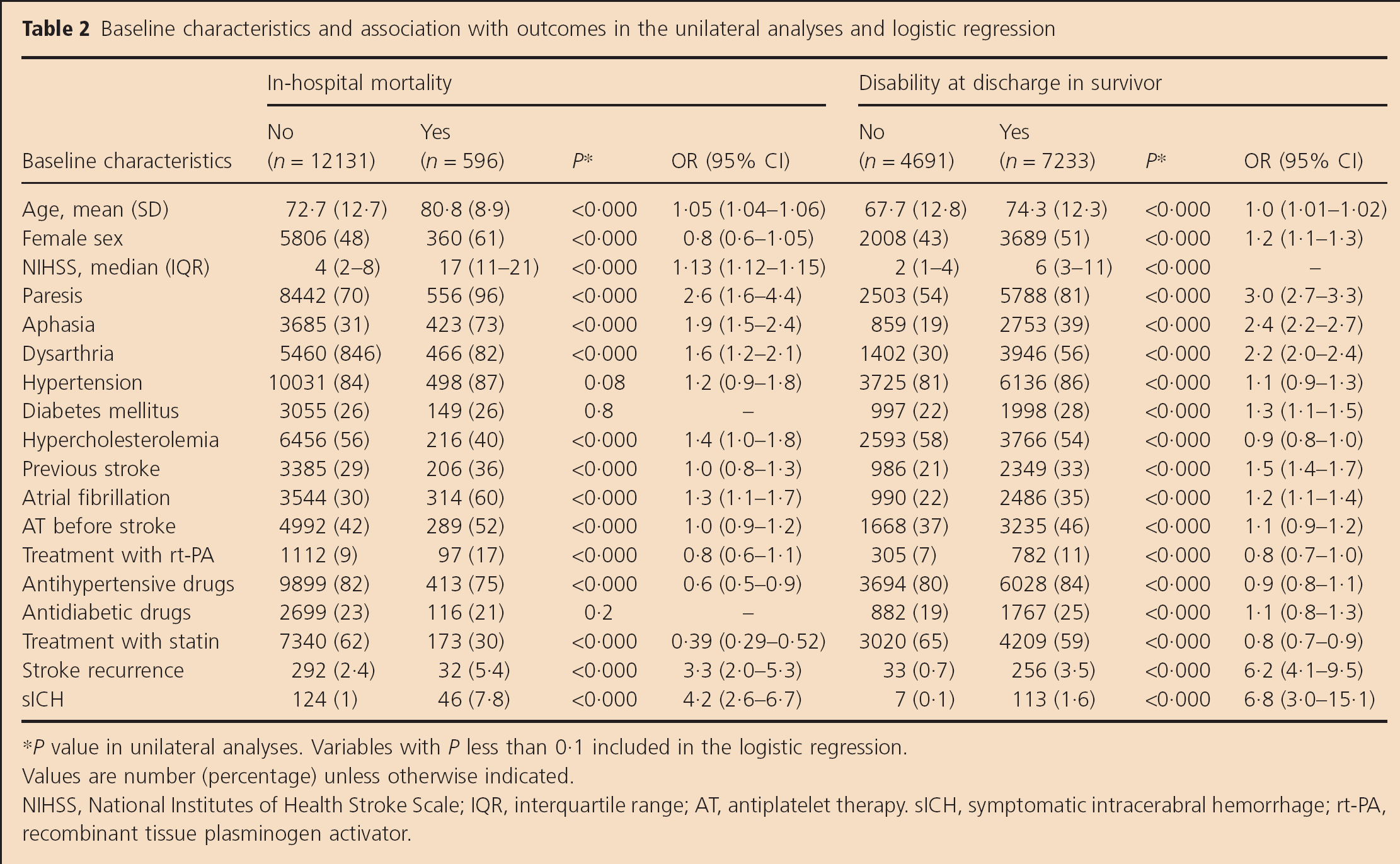
P value in unilateral analyses. Variables with P less than 0·1 included in the logistic regression.
Values are number (percentage) unless otherwise indicated.
NIHSS, National Institutes of Health Stroke Scale; IQR, interquartile range; AT, antiplatelet therapy. sICH, symptomatic intracerabral hemorrhage; rt-PA, recombinant tissue plasminogen activator.
During hospitalization, the frequency of secondary hemorrhagic stroke was significantly lower in the patients on statin medication than in those who did not receive statins (0·9% vs. 2·0%, respectively; P < 0·001), whereas the frequeny of ischemic stroke recurrence did not differ significantly between patients on statins and those not on statins (2·7% vs. 2·3%, respectively; P = 0·1) (Table 1).
Of the patients who were discharged alive (n = 12 181), 7601 patients (63%) agreed to be included in the three-month follow-up. The three-month mortality was obtained for 7195 of 7601 patients (95%). Among these patients (n = 7195), statin medication was administered to 4683 patients (65%). During the follow-up period of three-months after discharge, 498 patients (6·9%; 95% CI, 6·4–7·5%) died. The three-month mortality was lower in patients on statins than in those not on statins (5% vs. 10·6%, P < 0·001) (Fig. 1). In addition, the incidence of disability (mRS ≥ 2) at three-months after discharge was lower in patients on statins than in those not on statins (33% vs. 42%, P < 0·001) in patients who had survived the stroke (Fig. 2). Adjusted logistic regression analysis (Table 3) showed that the administration of statin medication was associated with reductions in the three-month mortality (OR, 0·48; 95% CI, 0·36–0·65; P < 0·001) and the three-month disability (OR, 0·79; 95% CI, 0·67–0·93; P = 0·004).
Baseline characteristics and association with outcomes at three-months after discharge in unilateral analyses and logistic regression in patients included in the follow-up (n = 7195)
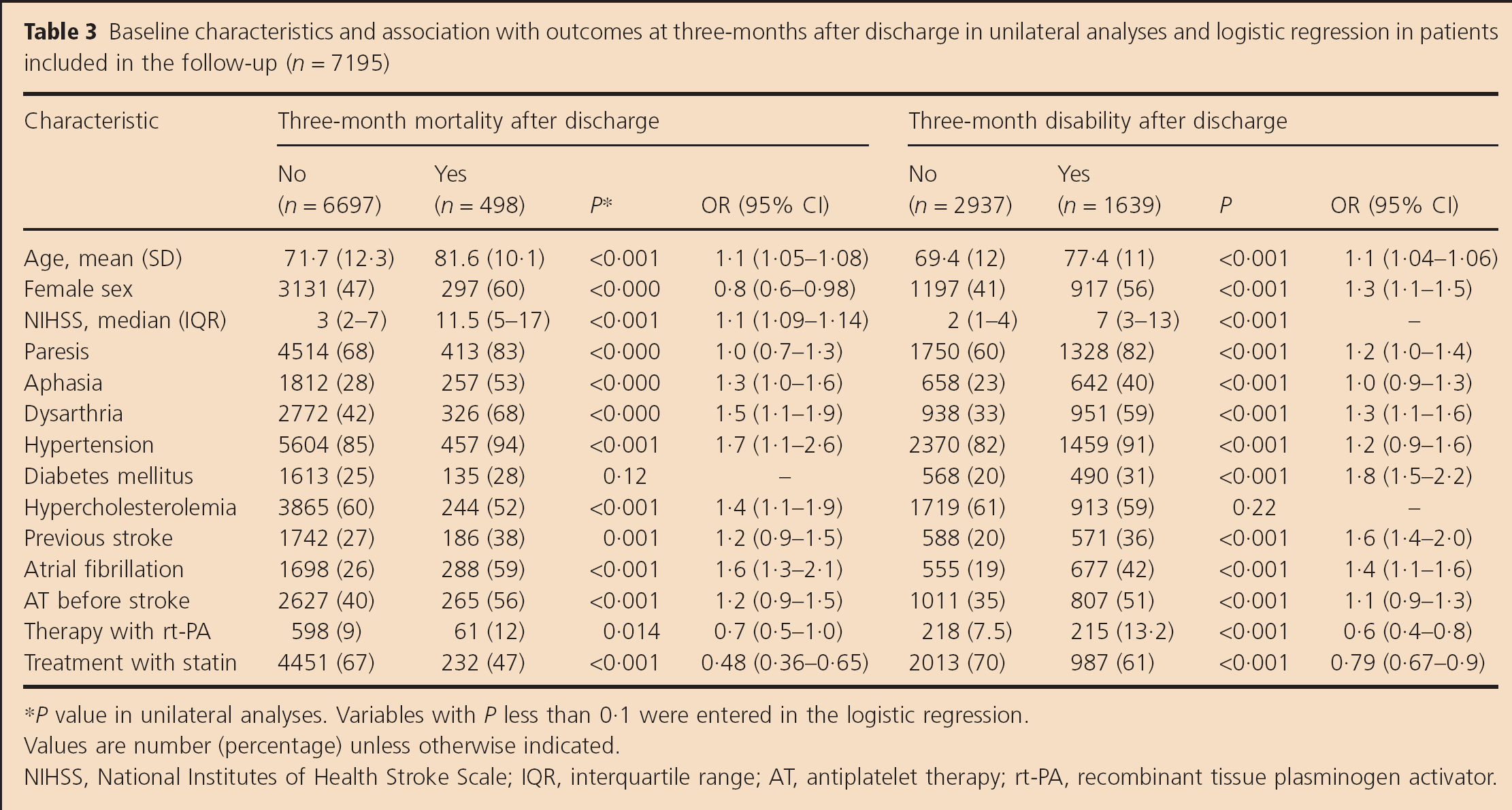
P value in unilateral analyses. Variables with P less than 0·1 were entered in the logistic regression.
Values are number (percentage) unless otherwise indicated.
NIHSS, National Institutes of Health Stroke Scale; IQR, interquartile range; AT, antiplatelet therapy; rt-PA, recombinant tissue plasminogen activator.
Discussion
In the present study, the mortality was lower in patients who received statin despite the fact that vascular risk factors were more common (Table 1). However, adjusted logistic regression, which was performed to assess all demographic, clinical parameters, and therapeutic procedures in univariate analyses (P < 0·1), revealed that statin therapy was associated with reductions in mortality and disability in patients with AIS (Tables 2 and 3).
Our findings are similar to those of other studies that have reported on the potential impact of pre- and poststroke treatment with statins on the severity of stroke and mortality in patients with AIS (12–14). A study by Kawashima et al. showed that statins reduce the stroke-associated infiltration of inflammatory cells, superoxide production in the brain parenchyma, and cerebral damage caused by stroke, as well as delay the appearance of stroke-associated symptoms and death in stroke-prone, spontaneously hypertensive mice (15). Another animal study demonstrated that the protective effect of statins on cerebral ischemia and thrombus formation was lost two to four-days after withdrawal of treatment with statins, independent of the level of cholesterol (16). An association between a brief withdrawal of statin and functional outcomes has also been found in clinical studies (17,18).
Moreover, statins have been found to increase cerebral blood flow, improve blood supply to ischemic cerebral parenchyma, and reduce stroke size; they have also been linked to the presence of more extensive collateral arteries in the brain (19–22). In addition, research has demonstrated that statins are associated with a reduction in platelet activation and with the stabilization of carotid artherosclerotic plaques (23,24). However, no difference in stroke recurrence during hospitalization was detected between patients on statins and those not on statins in the present study.
The primary prevention of ischemic stroke in statin users may be related to the lipid-lowering properties of statins; however, the reduction in stroke severity and mortality and the improvement in functional outcomes in statin users may be caused by antithrombotic and antiinflammatory effects, as well as by the effect on blood vessel dilation and the promotion of collateral artery growth, independent from the cholesterol-lowering effect. All these potential effects and actions of treatment with statins may have had a directly and indirectly impact on decreasing the severity of stroke, mortality, and disability after AIS in our population. In addition to the reduction in the risk of stroke, the administration of statin has been associated with a higher risk of hemorrhagic stroke in patients with prior stroke, according to the analysis put forth by the Stroke Prevention by Aggressive Reduction in Cholesterol Levels study (6,25). By contrast, the rate of secondary hemorrhagic stroke during hospitalization in our population was significantly lower in patients on statins than in those not on statins. Previous study by Biffi et al. showed that statin use improved the functional outcomes in patients who suffered from intracerebral hemorrhage (26). In the present study, the positive influence of the statin on the rate of the secondary hemorrhage may be due to the neuroprotective mechanisms and effect on cerebral blood flow of statin.
Our study has several limitations. One limitation is that 37% of patients did not agree to be included in the follow-up evaluation. The lack of agreement may be correlated to the stroke-related speech dysfunction (aphasia and dysarthria) whose rates were higher in patients who were not entered in the follow-up evaluation. Another limitation is that on the follow-up evaluation we did differ between patients who were interviewed by letter and those by telephone. Lastly, one limitation of this study was that we did not differentiate between patients who were on statins before stroke and those who received statin treatment early after admission. Therefore, potential for bias in the cases of poststroke statin administration and confounding by indication may contribute to benefits seen with early poststroke statin medication. Despite these limitations, our study has several strengths. It is the largest population-based study ever reported that includes patients who received standardized management and treatment of stroke in adherence to the guidelines of the German Stroke Society (27).
Our results are comparable with the findings of the meta-analysis by Ni Chroinin et al. among observational studies. However, a reduction of fatality was not found on meta-analysis of three randomized controlled trials. Furthermore, in studies that included only patients who were treated with recombinant tissue plasminogen activator, the statin seem to increase the fatality at three-months (28).
In summary, we found that the use of statin in patients with AIS may reduce the rates of mortality and disability after stroke, and that these patients may benefit from the possible neuroprotective effects of statin. Further studies are necessary to confirm these findings.