
Abstract
Stroke is the fifth leading cause of death and the first cause of long-term disability in Puerto Rico. Trained staff reviewed and independently validated the medical records of patients who had been hospitalized with possible stroke at any of the 20 largest hospitals located in Puerto Rico during 2007, 2009, and 2011. The mean age of the 5005 newly diagnosed stroke patients (51·2% female) was 70 years. At the time of hospitalization, women were 41/2 years older, were less likely to be married (60·2% vs. 39·9%, P < 0·001), smoked less (5·8% vs. 13·4%, P < 0·001), and had significantly higher proportion of diabetes (56·0% vs. 54·8%), hypertension (89·1% vs. 85·0%), and low density lipoprotein-cholesterol (LDL-Chol) > 100 mg/dL (65·7% vs. 57·5%) P < 0·05. Ischemic stroke represented 75% of all types of strokes. Atrial fibrillation was mentioned in 7·9% of the medical records. The risk for dying before discharge was similar for both genders, but was 40% higher for women than for men at one-year follow-up: age-adjusted odds ratio = 1·4 (95% confidence interval = 1·2–1·5).
Puerto Rico is a commonwealth of the United States and it is located in the Caribbean, east of the Dominican Republic. Its 3·7 million people are 99% Hispanic and span over 9104 km2 with a population density of 406·4/km2 (1). The proportion of residents over the age of 65 has increased from 11·2% in 2000 to 15·2% in 2011 (2). Stroke is a leading cause of death and disability in Puerto Rico, and the Puerto Rico Stroke Registry is the first island-wide stroke registry that collects ongoing, standardized, and reliable data on incidental, consecutive strokes. The registry was established in 2007 to obtain information on demographics, stroke subtype, medical and stroke severity measures, diagnostic evaluation, revascularization, in-hospital management, discharge disposition, in-hospital mortality and follow-up survival, and quality of care indicators from the 20 largest adult, nonmilitary medical centers in Puerto Rico with emergency care facilities. This manuscript focuses on the demographic profile; the distribution for known comorbidities for stroke including atrial fibrillation, diabetes, hypercholesterolemia, hypertension, and current smoking; the distribution of stroke type; and the in-hospital and long-term mortality among Puerto Ricans.
Trained physicians and nurses obtained information on age, sex, and marital status, and independently validated the medical records of patients who had been hospitalized with possible stroke International Classification of Diseases, 9th Edition, Clinical Modification (ICD-9-CM) codes 430–438, but without transient ischemic attacks (TIAs), i.e., ICD-9-CM code 435) at any of the 20 participating hospitals (all of which had emergency room capability) during study years 2007, 2009, and 2011. Since we were interested in documenting the incidence rates of newly diagnosed strokes, we restricted our study sample to patients hospitalized with an initial stroke. Patients initially hospitalized in one hospital and then transferred to another during the same event were counted only once. Each case was validated using the computed tomography or magnetic resonance imaging report provided in the medical record and classified as ischemic or hemorrhagic type. The detailed data collection and validation methodologies have been described elsewhere (3). Patients were classified as having diabetes and hypertension whenever these comorbidities were mentioned in the medical record, or if they were treated with hypoglycemic or antihypertensive agents, respectively. Patients treated with cholesterol-lowering drugs and/or documented low density lipoprotein (LDL) >100 mg/dL were considered having hyperlipidemia. Current smoking refers to the proportion of those who smoke at the time of hospitalization. The mortality rate during hospitalization was directly abstracted from the medical records, whereas the one-year survival status after discharge was obtained from the National Death Index and/or the Puerto Rico Department of Health vital statistics databases.
The geographic distribution of the 20 participating hospitals is shown in Fig. 1. A total of 5005 incidental acute stroke cases (mean age was 70 years and 51·2% female) were registered during 2007, 2009, and 2011 (Table 1). The proportion of strokes reached a peak at age 75–84 years and then declined in both genders. Atrial fibrillation was mentioned in the medical records in 7·9% of all cases. Women were less likely to be married than men (39·9% vs. 60·2% P < 0·001), showed smaller BMI (25·9 ± 6·3 vs. 28·3 ± 5·6, P < 0·001), and to be current smokers (5·8% vs. 13·4%, P < 0·001). Out of 10 stroke patients, approximately 5 had diabetes, 8 had hypertension, 3 had hyperlipidemia, and 1 was a current smoker. Women were more likely than men to have hypertension (89·1% vs. 81%, P = 0·010) and higher levels of low density lipoprotein-cholesterol (LDL-Chol) > 100 mg/dL (65·7% vs. 57·5%, P = 0·018). Although overall ischemic strokes (74·5%) accounted for the majority of stroke subtypes, women were more likely to have hemorrhagic strokes than men (20·0% vs. 16·7%, P = 0·02) (Table 2). The mortality rate during hospitalization was similar for both genders (10·2% for women and 8·9% for men, P = 0·15), but the age-adjusted risk for dying was 40% higher for women than for men at one-year follow-up odds ratio = 1·4 (95% confidence interval = 1·2–1·5).
Demographics, comorbidities, and mortality, by gender: the Puerto Rico stroke registry, 2007, 2009, and 2011
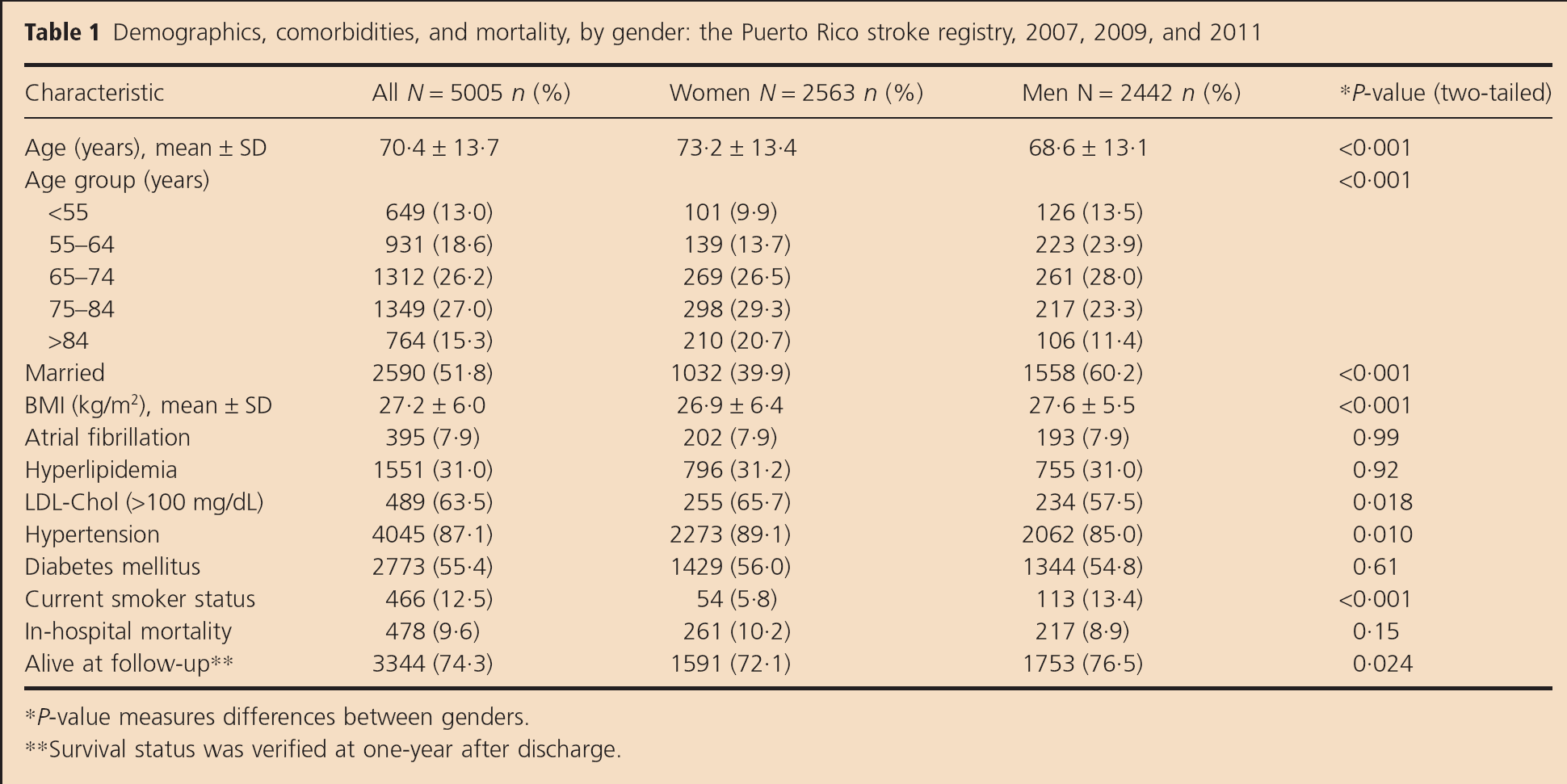
P-value measures differences between genders.
Survival status was verified at one-year after discharge.
Percentage of stroke subtype distribution, by gender: the Puerto Rico stroke registry, 2007, 2009, and 2011
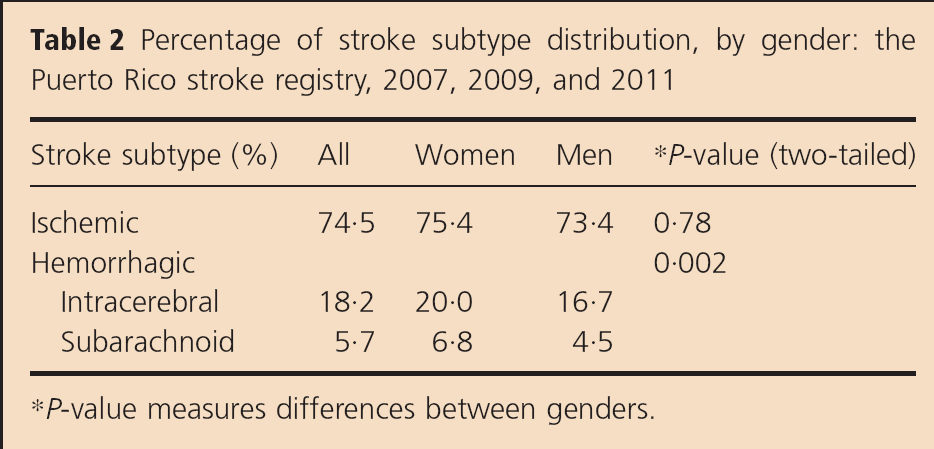
P-value measures differences between genders.

Geographic location of participating hospitals: the Puerto Rico stroke registry.
It is well documented that the incidence of stroke increases with age; this fact worsens the burden of stroke in Puerto Rico given that the proportion of Puerto Rican residents 65 years old and over has increased during the past decade by 34% from 11·2% to 15·2%. As compared with men, women in our study were more frequently hospitalized with a validated stroke, were in average 4 1/2 years older, were less likely to be married, had lower BMI, and smoke less, but had higher proportion of diabetes, hypertension, and LDL-Chol > 100 mg/dL. The higher age for suffering a first-time stroke and increased risk for stroke among women observed in our study is consistent with other findings reported in the published literature (4,5). The lower proportion of married women in our study is also similar to the proportion of married women suffering strokes in a national US sample (6). The proportion of diabetics in our study (56%) was substantially higher than the proportion reported by Go AS et al. in the United States (7·3%). Similarly, the proportion of patients with hypertension (88·9%) in our study was higher than the 77% reported in the Atherosclerosis Risk in Communities Study (ARIC), Cardiovascular Heart Study (CHS), and the Framingham Heart Cohort and Spring Studies (7). These differences may be in part explained by the higher prevalence of diabetes and hypertension observed in the Puerto Rican population as compared with US national figures (8). In our study, approximately 61% of patients hospitalized with an acute stroke had LDL-Chol >100 mg/dL, which is similar to findings reported in other epidemiological studies (9). The lower percentage of ischemic strokes in our study (74·5%) as compared with the 88% reported in the Greater Cincinnati/Northern Kentucky Stroke Study (GCNKSS-NINDS) (7) may be partially explained by the higher proportion of hypertension and consequently higher probability of intracerebral hemorrhage among our patients, especially among Puerto Rican women. The percentage of ischemic strokes attributable to atrial fibrillation has been reported to range between 1·5% among 50–59 years old to 23·5% among 80–89 years old in white populations in the United States (10) compared with (7·9%) our population. This difference may be partially explained because we did not include patients with TIAs.