
Abstract

Dear editor,
The Stanford type A aortic dissection (AD) manifesting with acute stroke presents a unique diagnostic and therapeutic challenge. Stroke is the most important neurologic complications, and has been reported to affect 5 to 10% of these patients (1–3).
We retrospectively collected the data of the patients with AD admitted to our Department, because of acute ischemic stroke or TIA, for a period of 20 years. Patients' baseline characteristics are described in Table 1.
Baseline characteristics of patients with stroke due to AD
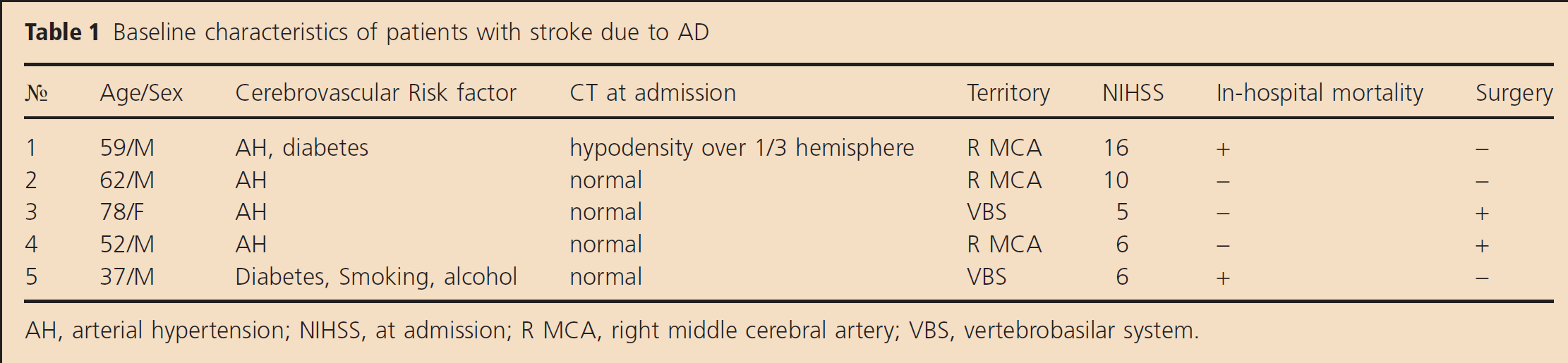
AH, arterial hypertension; NIHSS, at admission; R MCA, right middle cerebral artery; VBS, vertebrobasilar system.
The initial clinical presentation of our patients was not typical for AD. On arrival, they had no chest pain or pulse deficit. Transient arterial hypotension was detected only in one patient. The chest X-rays were negative and the electrocardiograms did not show ischemic changes. Blood test and cardiac enzymes were within normal limits.
In four of the cases, the first method of detecting the underlying pathology was extracranial ultrasonography (continuous wave and color duplex Doppler sonography) because of the highly specific and characteristic Doppler pattern (4) of the double lumen of common carotid artery (unilateral – in three cases, bylateral – in one), as well as the specific changes of sonograms of the internal carotid artery. Carotid abnormal ultrasound findings were combined with typical simultaneous flow changes in the right vertebral and subclavian arteries (in three cases). AD was confirmed by CT aortography in three cases and post-mortem in two of them. Thrombolytic treatment was considered in two patients before the diagnosis of a dissection; however, it was not performed due to the other exclusion criteria.
In conclusion, the patients with AD in our small cohort were predominantly men with hypertension. Despite the rare incidence of AD in stroke (5,6), this pathology should be presumed and subsequently excluded in all acute stroke cases, especially when considering thrombolytic treatment, to prevent poor outcome and severe complications. Ultrasonography could help with detecting AD before the initiation of thrombolysis.