
Abstract

Dear editor,
Opalski syndrome is a rare variant of the lateral medullary syndrome of Wallenberg accompanied by an ispilateral hemiparesis (1). However, the anatomic basis for this syndrome is not clear. In addition, hemimedullary infarct or bilateral medial medullary infarct is a rare disease and a combination of both is even rarer (2). We report a case of Opalski syndrome that progressed to hemimedullary infarct and contralateral medial medullary infarct and suggest a possible pathologic mechanism for Opalski syndrome. Previous reports have described the progression of lateral medullary to total hemimedullary infarct (3) or the progression of unilateral medial to bilateral medial medullary infarct (4), but to our knowledge no report described the pattern observed in this patient.
A 63-year-old man with a history of hypertension, diabetes, dyslipidemia, and coronary heart disease developed dizziness, left-beating nystagmus, right ptosis, hoarseness, dysphagia, and deteriorating right hemiparesis. Two decades previously, he had suffered a stroke and had recovered with a stable deficit of mild right hemiparesis. Deep tendon reflexes were more active on the right than the left. Diffusion-weighted imaging (DWI) obtained 90 min after onset revealed right lateral medullary infarct (Fig. 1a). One-day later, he developed left hemiparesis and hypalgesia of the right side of the body, but a repeat DWI showed no additional lesion (Fig. 1b). Three days later, vibration and joint position senses were diminished in the right hemibody and the left leg. T2-weighted MRI demonstrated progression of the initial right lateral medullary infarction to hemimedullary infarction extending to the cervical spinal cord and occurrence of the left medial medullary infarction (Fig. 1c and d). Magnetic resonance angiography showed absent right vertebral artery flow (Fig. 1e).
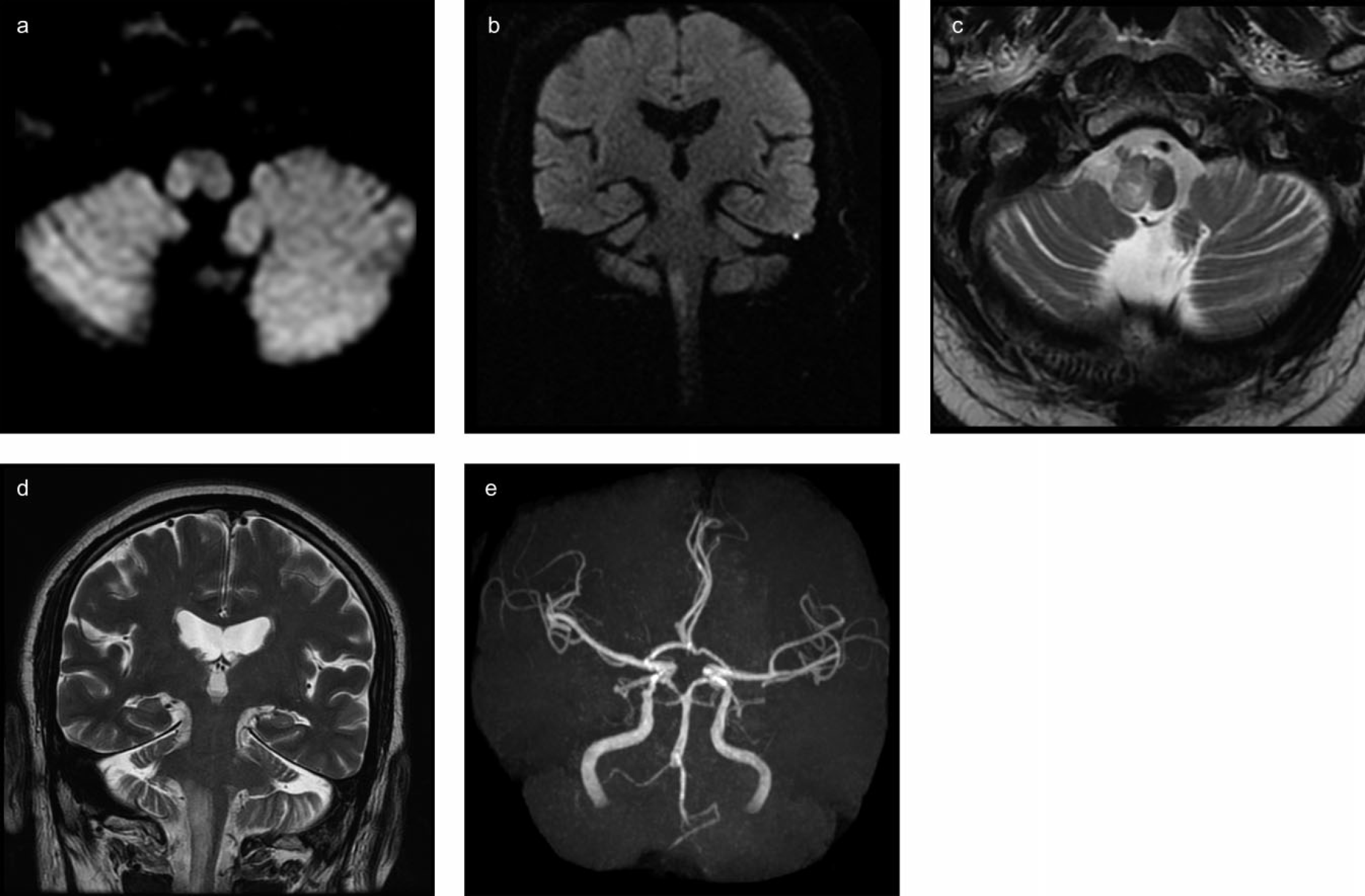
DWI obtained 90 min (a) and 18 h (b) after symptom onset demonstrates the right lateral medullary infarct. T2-weighted MRI (c and d) obtained four days after onset demonstrates progression of the initial right lateral medullary infarction to hemimedullary infarction extending to the cervical spinal cord and occurrence of the left medial medullary infarction. Magnetic resonance angiography (e) shows absent right vertebral artery flow.
This patient is of interest for two reasons. First, he developed hemimedullary infarct and contralateral medial medullary infarct, which is a rare combination. Second, he had right hemiparesis although the initial DWI revealed infarction in the right lateral medulla only. Therefore, the initial diagnosis was Opalski syndrome. Interestingly, the repeat MRI revealed the progression to the right hemimedullary and left medial medullary infarct. The right hemiparesis could be secondary to the lesion of the right lower medulla or spinal cord below the pyramidal decussation or to the lesion of the left medial medulla above the decussation, and these lesions might not be detected by the initial DWI. DWI performed within 24 h after onset do not often detect medial medullary infarct (5). Patients with Opalski syndrome should undergo repeat MRI to document additional lesions.