
Abstract
Background
Thirty percent of ischemic stroke (IS) patients suffering from acute stroke are under antiplatelet therapy.
Aims
We evaluated whether prior antiplatelet use before intravenous (IV), intra-arterial (IA) or combined IV/IA therapy may be associated with worse outcomes and an increased intracerebral hemorrhage (ICH) risk after reperfusion therapies.
Methods
We analyzed data from our patient registry (n = 874) and conducted a systematic review of previous observational studies. The primary outcome was the percentage of patients who developed symptomatic ICH (sICH), defined in our registry per ECASS-II definition.
Results
We identified 43 previous reports that evaluated the impact of prior antiplatelet use on outcomes after reperfusion therapy in AIS patients. Prior antiplatelet use was found in 35% of AIS patients, eligible for reperfusion therapies and was associated with a worse vascular profile. In an unadjusted meta-analysis that included our registry data, prior antiplatelet use was associated with more sICH per ECASS-II definition (OR, 1·78 (95% CI, 1·48–2·13), and less favorable outcome (OR, 0·86; 95% CI, 0·77–0·98). However, in multivariate analyses conducted in our registry showed that prior antiplatelet use was not associated with worse outcome (P > 0·23); and in the systematic review, only 3 studies reported a slight, but significant adjusted increase in sICH risk, of whom one had conflicting results according to sICH definition.
Conclusions
These results suggest no significant detrimental effect of prior antiplatelet use in AIS patients treated by IV, IA or combined IV/IA therapy. Further studies are needed to assess the specific impact of different and cumulative antiplatelet agents.
Introduction
Intracerebral hemorrhage (ICH) remains the major safety issue with alteplase administration in the setting of acute ischemic stroke (AIS). This related bleeding risk raises the question of reperfusion therapy eligibility in AIS patients under antiplatelet drugs. The ARTIS trial has shown that administration of intravenous (IV) aspirin, at the dosage of 300 mg, within 90 min after IV alteplase increases the risk of symptomatic intracranial hemorrhage (sICH) (1). These evidences reinforced the current guidelines that preclude the use of any antiplatelet agent within 24 h after IV alteplase administration. Prior antiplatelet use is, however, not a contraindication to IV or intra-arterial (IA) thrombolysis (2), but the increased ICH risk, if any, is source of controversy. Previous studies, mostly restricted to AIS patients treated by IV thrombolysis, have shown conflicting results according to the impact of prior antiplatelet use on symptomatic ICH risk and favorable outcome (3–6). The heterogeneity of the sICH definition used in IV thrombolysis registries contributes to the conflicting evidences (7). In addition, antiplatelet-specific data in patients treated with IAT or other endovascular therapy is limited in comparison to the aforementioned IVT studies. This clinical condition is relevant, as the proportion of IV alteplase-treated patients under antiplatelet therapy may be as high as 30% (7).
We therefore evaluated whether prior antiplatelet use before IVT, IAT or combined therapy may be associated with worse outcomes by examining data from our prospective clinical registry and conducting a systematic review of previous observational or interventional studies.
Methods
Bichat clinical registry
Stroke program
We identified patients from a prospective clinical registry of AIS patients treated between February 2002 and February 2013 at Bichat University Hospital. As described previously, before April 2007, all patients were treated with conventional IV thrombolysis, and none with an IA approach (8). After April 2007, patients eligible for IV thrombolysis were treated with conventional IV thrombolysis in case of no documented arterial occlusion and with a systematic IV–IA approach in case of documented arterial occlusion. Patients ineligible for IV treatment, with a documented arterial occlusion, were treated by the IA approach.
Standard protocol approvals, registration, and patient consents
Informed consent was obtained from the patient or their representative and the research protocol was approved by the Ethics Committee from Ambroise Paré Hospital.
Data collection and definitions
Information on patients' demographic characteristics, medical history, current medications, laboratory and imaging findings, vital signs before treatment, National Institutes of Health Stroke Scale (NIHSS) scores (at admission, and at 1, 3 and 24 h after the initiation of treatment), clinical outcomes were collected prospectively using a structured questionnaire. Times from symptom onset (or from when the patient was last seen in a normal condition) to treatment initiation were also recorded. All patients had a computed tomography (CT) or magnetic resonance imaging (MRI) scan 24 h after treatment onset to assess hemorrhagic complications. For patients receiving IA therapy, the recanalization status of the occluded artery was monitored with conventional angiography, and the time to recanalization was noted. Recanalization was measured with the Thrombolysis In Myocardial Infarction (TIMI) score (reference) by two members of staff (E. M. and M. M.) and was used for all imaging modalities. Modified Rankin Scale (mRS) at three-months was assessed during face-to-face interviews or via telephone calls by a senior vascular neurologist (E. M. or M. M.), who was certified for mRS scoring.
Outcome definitions
The primary study outcome was the percentage of patients who developed sICH, defined as a hemorrhage on the follow-up CT/MRI scan associated with an increase of ⩾4 points in NIHSS score (9). Secondary outcomes included any ICH, favorable outcome (defined as an mRS of 0–2 at 90 days), excellent outcome (defined as an mRS of 0–1 at 90 days), 90-day mortality, and early neurological improvement (defined as an NIHSS score of 0–1 at 24 h or a ⩾ 8 points decrease in NIHSS score at 24 h). Tertiary outcomes were evaluated in subset of patients treated by IA therapy, included any recanalization (defined by TIMI 2–3) and complete recanalization.
Systematic review
Search strategy and study selection
We performed a computerized PubMed search of articles published between January 1996 and April 2013 to identify all observational and interventional studies that described the impact of ⩾1 antiplatelet medications (regardless the class and combination) current use on safety and/or efficacy outcomes in AIS patients treated by an IV and/or IA strategy. We used the search terms [thrombolysis OR fibrinolysis OR thrombolytic OR IV OR IA OR endovascular OR mechanical OR thrombectomy] AND stroke without any language restriction. One author (J. L.) selected relevant articles based on the title and abstract, and obtained the full text for detailed review. We also searched the reference lists of retrieved articles and published review articles for additional studies. Studies were selected using the following criteria: (1) involving subjects aged ⩾18 years; (2) retrospective or prospective (observational or interventional) studies with at least 100 patients with AIS treated by IV and/or IA approach; and (3) that reported a statistical analysis on the association of outcomes (safety and/or efficacy) with current antiplatelet medications. We did not select studies according to treatment strategy, time to treatment or the reported outcome definitions. We screened duplicate publications based on the same data sets (i.e. overlapped data among different studies). When multiple end-points were reported in separate publications, duplicate publications were included. For other duplicate publications, only the report with the most complete data was included.
Data extraction
Two authors (J. L. and E. M.) independently extracted data using a standardized form, and any disagreement was resolved by consensus. We did not contact the authors of the studies to request incomplete or unpublished data. We collected the following data: report characteristics (first author's name, journal, year of publication); study design [country, study period, number of centers, AIS treatment (IV agents, IA chemical agents, IA mechanical therapy)]; study sample [sample size, mean age, sex ratio, mean admission NIHSS, mean onset to treatment time, number (%) of patients under antiplatelet medication], incidence and definition of outcomes (functional outcome, neurological improvement, recanalization, mortality, intracranial hemorrhage), direction of association between antiplatelet medications and each outcome, and, if available, a measure of the strength of the association in univariate and multivariate analyses.
Statistical analysis
Statistical testing was done at the two-tailed α level of 0·05 except in tests for homogeneity in which an α level of 0·10 was used. Data were analyzed using the SAS software version 9·3 (SAS Institute, Cary, NC).
Bichat clinical registry
We made univariate comparisons between antiplatelet and non-antiplatelet groups using chi-square tests for categorical variables (Fisher's exact test was used when the expected cell frequency was <5) and Student's t-test for continuous variables (Mann–Whitney U-test was used for non-Gaussian distributions). We investigated the effect of prior antiplatelet use on clinical and recanalization outcomes using logistic regression model adjusted for baseline characteristics differences. Further analyses were done by treatment strategy (IV alone vs. combined IV/IA therapy vs. IA alone).
Systematic review
Using all available data, we calculated individual unadjusted odds ratios (ORs) and 95% confidence intervals (CIs) for sICH and favorable outcome using non-antiplatelet users as the reference group. Pooled ORs were computed using the inverse-variance weighted random-effects model; heterogeneity between studies was examined using the chi-square test for homogeneity followed by the calculation of the I2 statistic. A subgroups analysis was done based on sICH definitions.
Results
Bichat clinical registry
From February 2002 to February 2013, 879 consecutive AIS patients were treated with IV and/or IA therapy. Of these, five patients were excluded since no information on current use of antiplatelet therapy before stroke onset could be obtained (supplemental Fig. S1). In the study sample, 288 patients (33%) were currently treated with antiplatelets before stroke occurrence. Patient's baseline characteristics are described in Table 1. Antiplatelet users were older, had more often hypertension, hypercholesterolemia, cardioembolic strokes, and had a higher blood glucose level than their counterparts. No significant differences between antiplatelet and non-antiplatelet users were found in respect to stroke severity (assessed by the NIHSS), arterial occlusion (presence and site of occlusion), treatment strategy or onset time to treatment.
Bichat clinical registry: baseline characteristics according to prior antiplatelet use
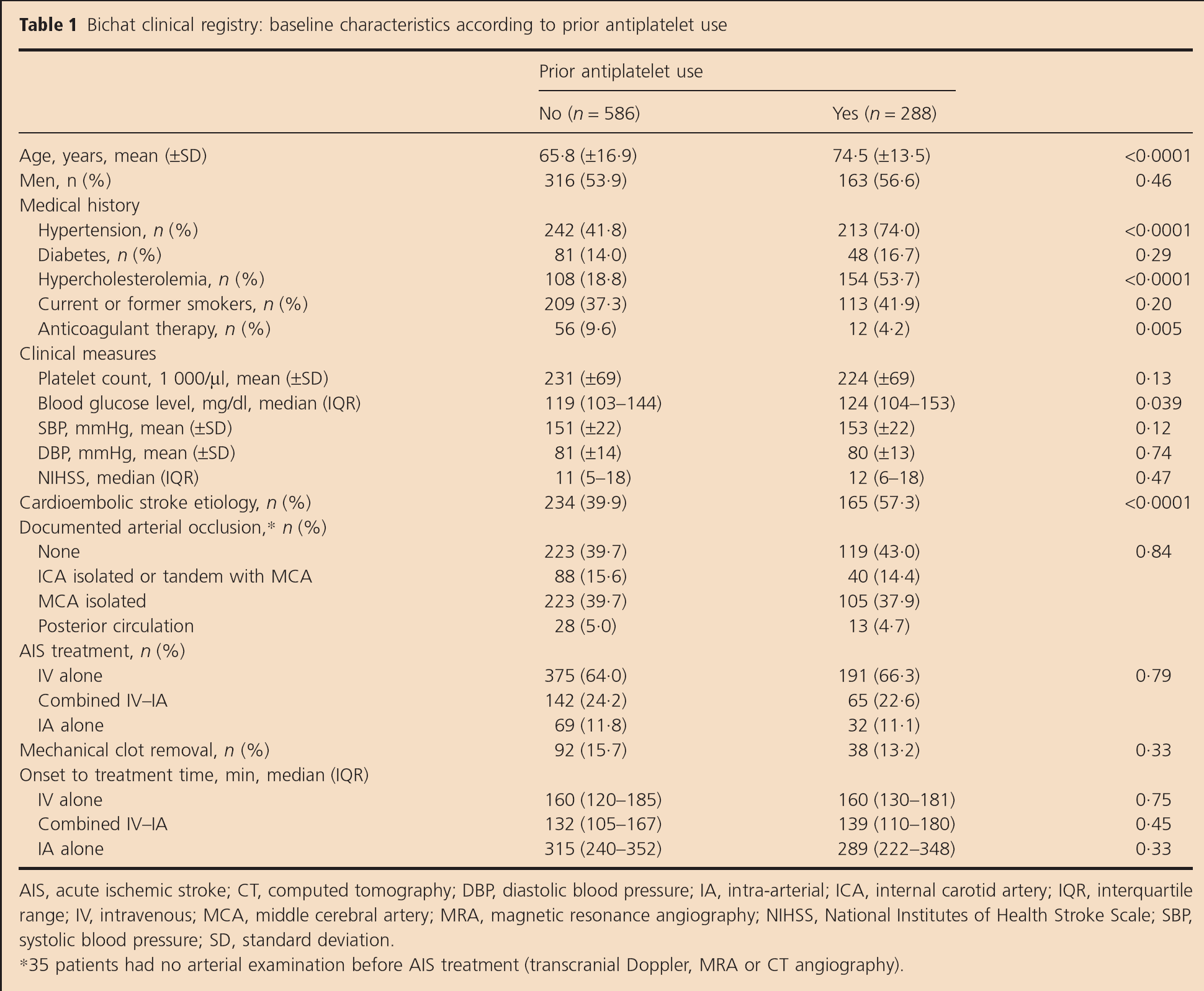
AIS, acute ischemic stroke; CT, computed tomography; DBP, diastolic blood pressure; IA, intra-arterial; ICA, internal carotid artery; IQR, interquartile range; IV, intravenous; MCA, middle cerebral artery; MRA, magnetic resonance angiography; NIHSS, National Institutes of Health Stroke Scale; SBP, systolic blood pressure; SD, standard deviation.
35 patients had no arterial examination before AIS treatment (transcranial Doppler, MRA or CT angiography).
Prior antiplatelet use and clinical outcome
Overall, any ICH occurred in 193 patients (22%), including 59 sICH (6·8%) according to the ECASS II definition. In univariate analysis, as well as, in multivariate analysis, no significant difference was found in hemorrhagic complication and 90-day mortality rates according to prior antiplatelet use (Table 2). Similar findings were found in stratified analyses by treatment approach (supplemental Table S1). Regarding the efficacy outcome, only a trend toward lower rates of favorable outcome in antiplatelet users compared with non-antiplatelet users was found in univariate analyses (53% vs. 60%; P = 0·03). However, after adjustment for baseline between-group differences, this difference remained not significant (OR, 0·81; 95% CI 0·58–1·15; P = 0·23).
Bichat clinical registry: outcomes according to prior antiplatelet use
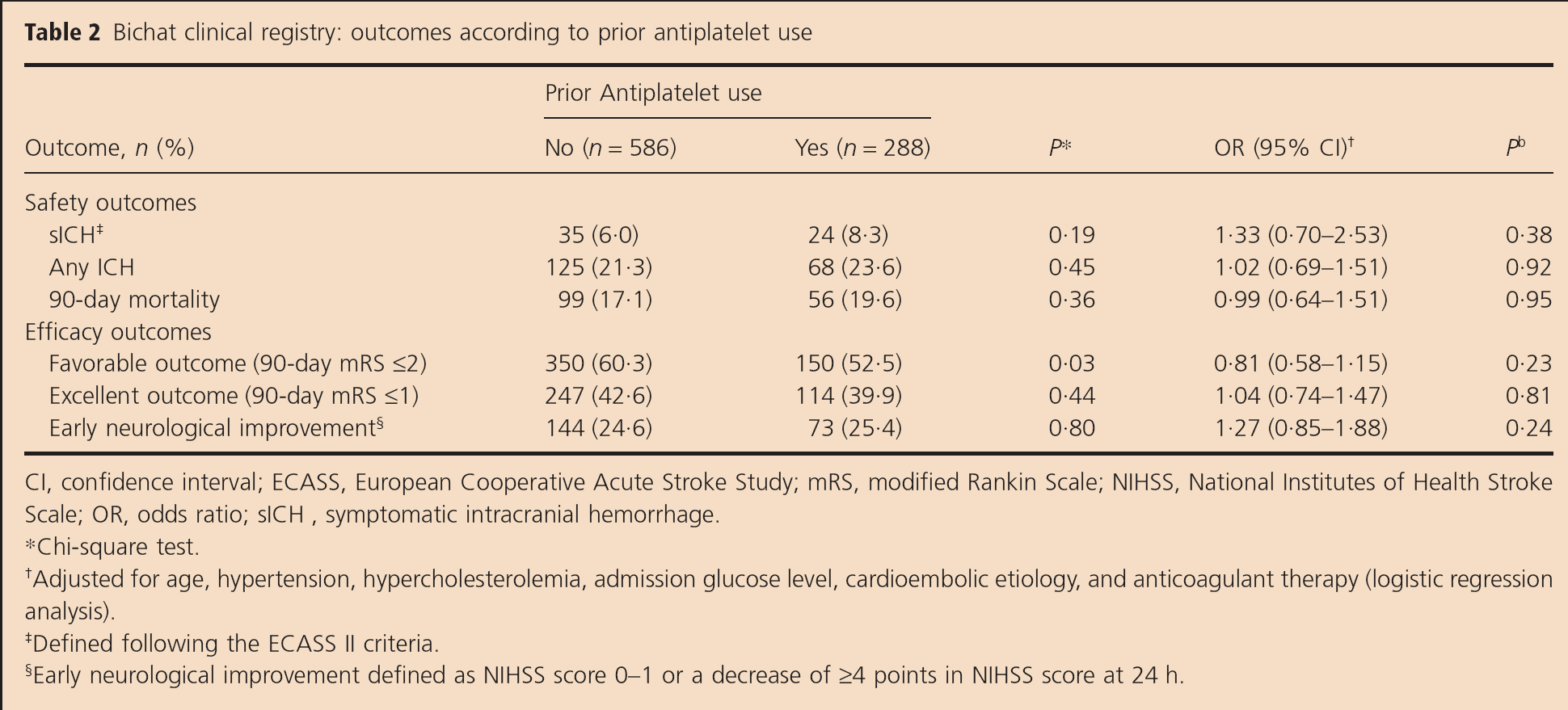
CI, confidence interval; ECASS, European Cooperative Acute Stroke Study; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio; sICH, symptomatic intracranial hemorrhage.
Chi-square test.
Adjusted for age, hypertension, hypercholesterolemia, admission glucose level, cardioembolic etiology, and anticoagulant therapy (logistic regression analysis).
Defined following the ECASS II criteria.
Early neurological improvement defined as NIHSS score 0–1 or a decrease of ⩾4 points in NIHSS score at 24 h.
Prior antiplatelet use and recanalization in IA-treated patients
Among the 308 IA-treated patients, there was only a nonsignificant trend toward lower recanalization rates in antiplatelet users compared with non-antiplatelet users. Recanalization rates (TIMI 2–3) were 67% in antiplatelet users and 77% in non-antiplatelet users (P = 0·06); complete recanalization rates (TIMI 3) were respectively of 42% and 53% (P = 0·09). In multivariate analyses, OR associated with prior antiplatelet use were 0·60 (95% CI, 0·33–1·12; P = 0·11) for any recanalization and 0·83 (95% CI, 0·47–1·45; P = 0·51) for complete recanalization. In the subset of patients who achieved any recanalization (n = 228), the median time from symptom onset to recanalization was 264 min (IQR, 224–302 min) in antiplatelet users and 258 min (IQR, 208–346 min) in non-antiplatelet users (P = 0·84).
Crude meta-analysis
Systematic review is available in online only (see supporting information). The literature search identified 17 347 citations of which 248 full articles were read and 43 (included separate publications on different outcomes based on the same or subset data sets) were judged eligible for inclusion in the systematic review (supplemental Fig. S2). The main baseline characteristics, treatment strategies, outcomes (definitions and incidences), and direction of association between prior antiplatelet use and outcome are summarized in supplemental Table S2.
Prior antiplatelet use and ICH
When combining the available unadjusted results for sICH outcome, we found a significant increased sICH risk in antiplatelet users compared to nonusers (Fig. 1). Similarly, we found a significant detrimental effect of antiplatelets, whatever the sICH definition used, with a pooled OR of 1·75 (95% CI, 1·41–2·17) for sICH per NINDS, 1·78 (95% CI, 1·48–2·13) for sICH per ECASS-II, and 2·49 (1·90–3·27) for sICH per SITS-MOST (Fig. 1). Overall and by sICH definitions, there is no major heterogeneity detected across studies. Sensitivity analysis restricted to single-center studies yielded similar results, with a pooled OR for antiplatelet use of 1·89 (95% CI, 1·45–2·46; I2 = 0%).
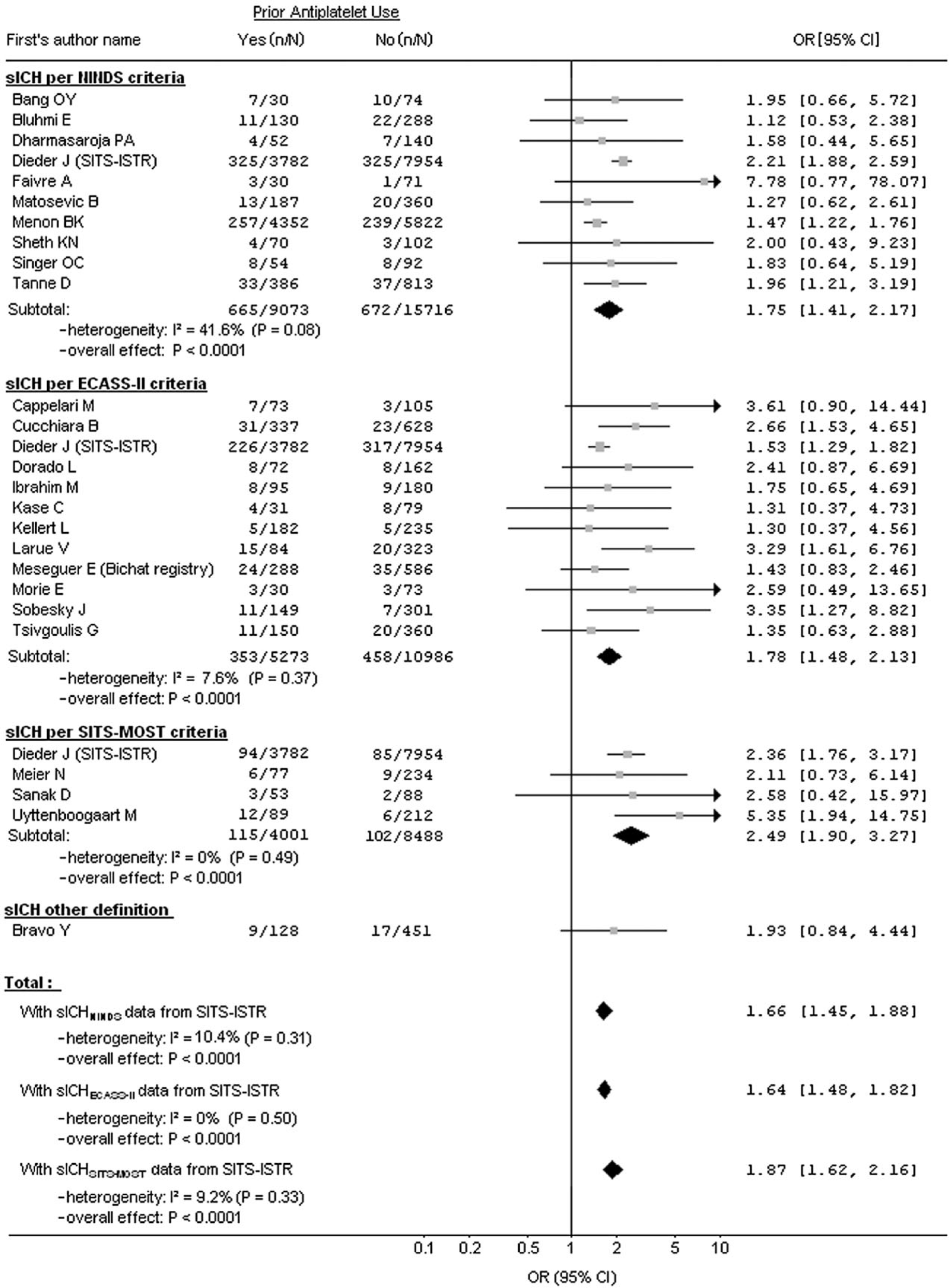
Forest plots of unadjusted ORs for sICH associated with prior antiplatelet use. CI, confidence interval; OR, odds ratio; sICH, symptomatic intracranial hemorrhage.
In the meta-analysis combining the available unadjusted results with our results, the incidence of good outcome was significantly lower in antiplatelet users compared to nonusers (Fig. 2). A similar result was found in sensitivity analysis excluding SITS-ISTR (unadjusted pooled OR, 0·84; 95% CI, 0·71–0·98; P = 0·03).
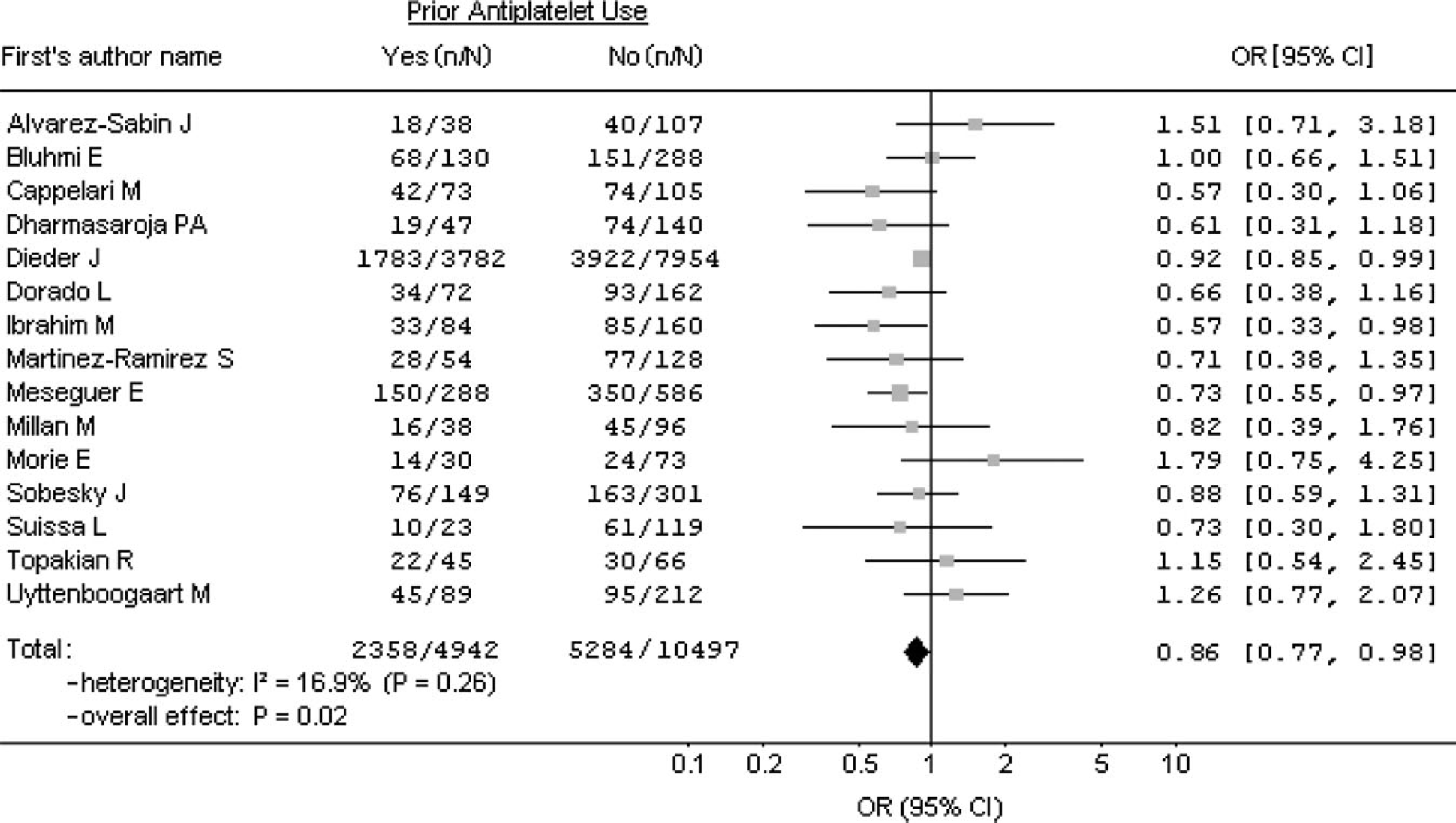
Forest plots of unadjusted ORs for favorable outcome associated with prior antiplatelet use. CI, confidence interval; OR, odds ratio.
Discussion
This systematic review, including our registry data, shows that 35% of AIS patients eligible for reperfusion therapies are under an antiplatelet regimen. This condition is associated in univariate analysis with a detrimental effect on ICH risk, and functional outcome. However, in our registry and most of the retrieved previous studies, the profile of antiplatelet users included older patients, with significantly more vascular risk factors known to be associated with ICH risk and unfavorable outcomes (e.g. high glucose level and cardioembolic sources) (10). In our registry, when multivariate analyses were conducted, prior antiplatelet use was not associated with ICH increased risk, as well as, with other clinical outcomes. Although the crude meta-analysis showed a significant increase of sICH and lower rates of favorable outcome in antiplatelet therapy users, no definitive conclusions can be drawn due to the absence of adjustment on confounders. Unfortunately, we could not perform an adjusted meta-analysis since no adjusted effect size was available in most of the retrieved studies. Among them, only three reported an increased sICH risk, both in univariate and multivariable analyses, including 11 736 patients from the SITS-ISTR (with SITS-MOST and ECASS-II SICH definition but not with NINDS definitions). In addition, none of retrieved studies reported a detrimental effect on favorable outcome in statistical analyses including the highest number of covariables. These findings are similar to those obtained in studies conducted on statins (8) or warfarin (11) where the impact of vascular risk factors has been reported to overwhelm the role of the studied drug.
Regarding the routes of reperfusion therapy, we found similar results in patients treated by endovascular therapy in our registry, suggesting that the available evidence for IV thrombolysis can be extended to endovascular therapy. Moreover, in accordance with the five previous studies that reported recanalization outcomes, there was no significant impact of antiplatelet therapy on recanalization rates in patients eligible for IA therapy. Thus, the weight of evidence in this systematic review, including our registry data, favors an absence of impact of prior antiplatelet use on safety and efficacy outcomes after acute reperfusion therapies.
One of the major limits in our study is the scarce data on the antiplatelet drug type. Although different antiplatelets are available, published data do not include the type and combination of antiplatelet agent, including our registry where this information was not prospectively collected. Three studies described in multivariate analyses a detrimental effect of antiplatelets other than aspirin (12–14) and one described a greater detrimental effect of double antiplatelets therapy compared with a single antiplatelet therapy (6). Further studies are needed to confirm these findings and to assess the safety and efficacy of new antiplatelet agents such as P2Y12 inhibitors (ticagrelor or plasugrel) in AIS patients eligible to reperfusion therapies.
In addition to the previous limitations, the present findings are derived from observational analyses that are subject to well-known limitations, as the potential for confounding by measured or unmeasured variables, which cannot be ruled out. The heterogeneity in sICH definition used among studies could explain the differences found in the results. In our study and likely in previous studies, prior antiplatelet use was based on patients or family reports, which is a potential source of bias. Finally, we cannot excluded that some relevant studies were not included in our review, since our search was limited to published reports in the PubMed data base.
In summary, on the basis of available literature, including the data from our registry, prior antiplatelet use should not considered as a criterion of ineligibility for any AIS revascularization. Prior antiplatelet use has to be considered as an indicator of past vascular disease, which is by itself associated with unfavorable outcome. Further studies are needed to assess the specific impact of different and combination of antiplatelet agents.