
Abstract
Cilostazol is an antiplatelet drug often used in Asian countries like Korea, Japan, and China. However, it is rarely used in the west. Cilostazol inhibits phosphodiesterase, increases cyclic AMP concentrations, and consequently inhibits platelet aggregation. Interestingly, it also has vasodilatory activity, inhibits vascular smooth muscle proliferation, and protects the endothelium. Studies in Asia have shown that cilostazol is effective in the secondary prevention of stroke. Moreover, it is significantly less likely to cause bleeding complications than aspirin. Additional trials have shown that cilostazol is effective in the prevention of intracranial atherosclerosis progression. Unfortunately, cilostazol has rarely been studied in non-Asian stroke patients and, accordingly, the benefits of cilostazol are less well appreciated in Europe and America than in Asia. Although further studies are required, we suggest that at least some stroke patients (e.g., patients prone to bleeding, patients with intracranial atherosclerosis, etc.) may readily benefit from cilostazol regardless of ethnicity.
Introduction
Antiplatelet drugs are generally used for secondary stroke prevention. Among them, aspirin is the most widely used, principally because of medical economics. However, the efficacy of aspirin is modest, and the risk of bleeding – including cerebral hemorrhage – is increased. Cilostazol is an antiplatelet drug which is often used in Asian countries like Korea, Japan, and China. Cilostazol inhibits phosphodiesterase, increases cyclic AMP concentration, and consequently inhibits platelet aggregation. Interestingly, it also has vasodilatory activity, inhibits vascular smooth muscle proliferation, and protects the vascular endothelium. Unlike aspirin, it is associated with a low risk of bleeding complications.
The research on cilostazol has been performed mostly in Asia. Therefore, there is a conceptual gap between the East and West; cilostazol is widely used in some parts of Asia, while it is not in Europe and America (1). In this article, we review the research conducted in Asia that examines the effects of cilostazol on the secondary prevention of stroke. We will then discuss whether these results can be applied to non-Asian patients.
Trials using cilostazol conducted in Asia
Among the 213 articles found by searching PubMed using the search string ‘cilostazol’ AND ‘clinical trial’ AND ‘humans’, 10 articles (2,–11) included randomized controlled clinical trials using cilostazol for treatment of ischemic stroke. In addition, an article recently published by one of the authors was included (12). As shown in Table 1, the 11 trials recruited 6718 patients from Asian countries including Japan, China, Korea, Thailand, and the Philippines.
Trials using cilostazol conducted in Asia
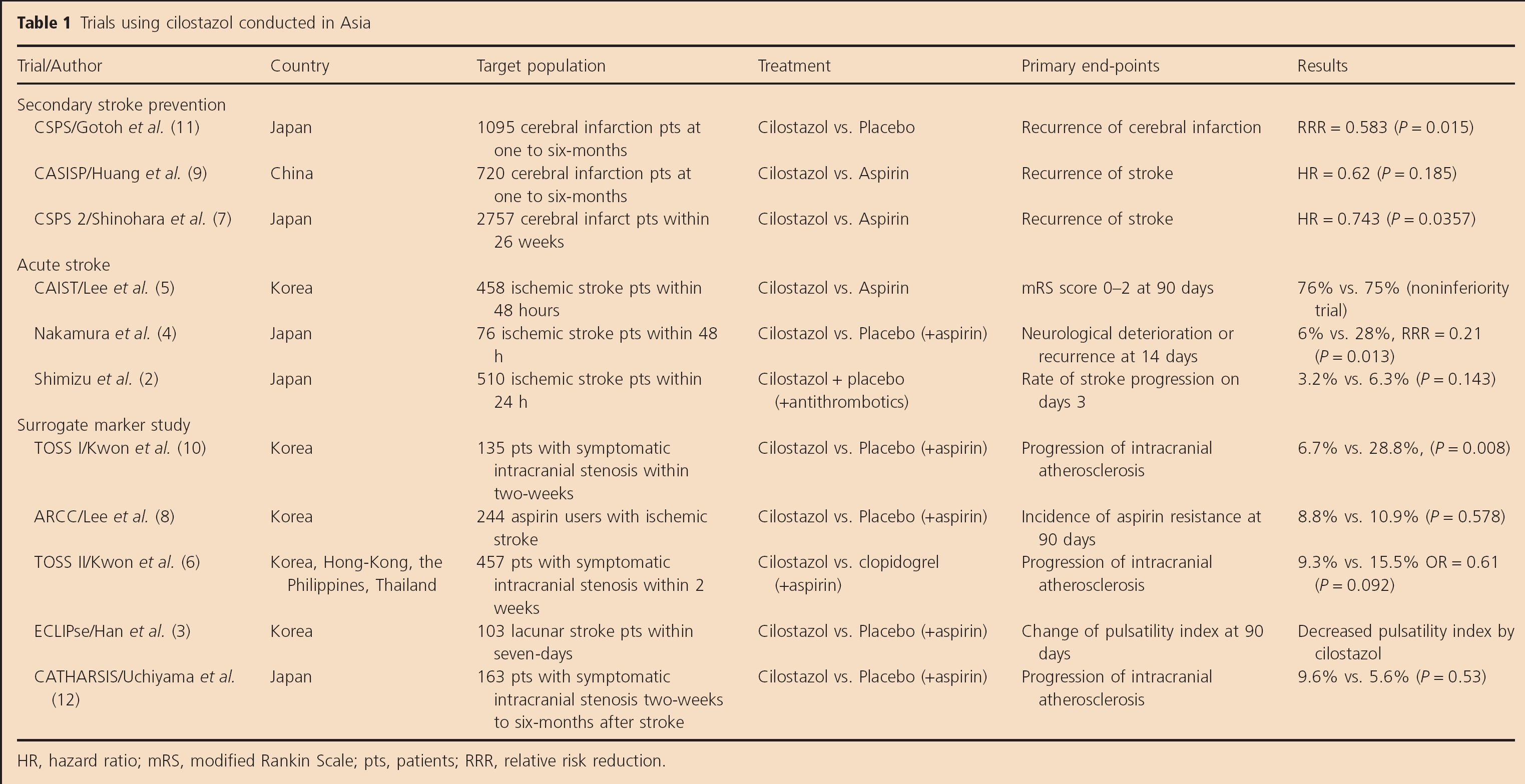
HR, hazard ratio; mRS, modified Rankin Scale; pts, patients; RRR, relative risk reduction.
Secondary stroke prevention
The Cilostazol Stroke Prevention Study (CSPS) (11) was the first clinical trial to examine the secondary stroke prevention efficacy of cilostazol. It recruited 1095 Japanese, ischemic stroke patients within one to six-months of stroke onset. Patients were randomized to receive either cilostazol or a placebo. Cilostazol treatment significantly reduced recurrent ischemic stroke [42.3%; 95% confidence interval (CI) = 10.3% to 62.9%, P = 0.0127]. Additionally, it did not increase the incidence of bleeding complications compared with the placebo.
Subsequently, two large trials compared the safety and efficacy of cilostazol and aspirin in ischemic stroke patients. Investigators from the Cilostazol vs. Aspirin for Secondary Ischemic Stroke Prevention (CASISP) study hypothesized that cilostazol may be better than aspirin for Chinese ischemic stroke patients due to the higher prevalence of aspirin-related cerebral hemorrhages in China (9). Patients who had suffered an ischemic stroke in the last 1–6 months (n = 720) were randomized into a cilostazol and an aspirin group and treated for 12–18 months. Recurrent strokes occurred in 12 patients in the cilostazol and 20 in the aspirin group [hazard ratio (HR) = 0.62; 95% CI = 0.30–1.26; P = 0.185]. Hemorrhagic stroke was reported in six patients, of whom only one had received cilostazol. Additionally, follow-up magnetic resonance imaging (MRI) revealed that asymptomatic cerebral hematoma occurred in four patients in the aspirin group and in only one patient in the cilostazol group.
In the Cilostazol Stroke Prevention Study 2 (CSPS2), 2757 Japanese patients were randomized into a cilostazol group and an aspirin group (7). The mean follow-up period was 29 months. The primary end-point (the first occurrence of stroke including cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage) was reached by 2.76%/year (n = 82) in the cilostazol and 3.71% (n = 119) in the aspirin group (HR = 0.743; 95% CI = 0.564–0.981; P = 0.0357). A significantly lower incidence of major hemorrhagic events occurred in the cilostazol group (HR = 0.458; 95% CI = 0.296–0.711; P = 0.0004).
Based on these large-scale clinical trials, it can be concluded that cilostazol is at least as effective as aspirin for secondary stroke prevention, and associated with significantly less frequent bleeding complications than aspirin.
Treatment of acute ischemic stroke
Three clinical trials have examined the efficacy of cilostazol in the acute stage of stroke: Cilostazol in Acute Ischemic Stroke Treatment (CAIST) (5), Tohoku Acute Stroke Progressing Stroke Study (2), and a small pilot study performed in Japan (4).
The CAIST study investigators recruited 458 Korean ischemic stroke patients. Within 48 h of the onset of stroke, they were treated with cilostazol (200 mg/day) or aspirin (300 mg/day) for 90 days. The primary end-point [the proportion with a modified Rankin Scale (mRS) score of 0–2] was achieved in 76% of the cilostazol group and 75% of the aspirin group. The rates of bleeding complications were not significantly different. The Tohoku Acute Stroke Progressing Stroke Study recruited 510 Japanese patients with noncardioembolic ischemic stroke within 24 h of stroke onset. Patients were randomized to receive either cilostazol (200 mg/day) or no medication apart from routinely used antiplatelets. The primary end-point was progressing stroke, defined as an increase in National Institutes of Health Stroke Scale (NIHSS) score by 4 points or more on day 3 and/or on day 5. The proportion with progressing stroke was 3.2% in the cilostazol group and 6.3% in the control group (P = 0.143). The number of patients in the cilostazol group with an mRS score of 0–2 after 90 days was comparable with the control group (88.1% vs. 84.8%).
Trials using surrogate end-points
Five trials used surrogate markers as a primary end-point to show the beneficial effect of cilostazol in a certain group of stroke patients. The Trial of Cilostazol in Symptomatic Intracranial Stenosis (TOSS I) study (10) investigated the effect of cilostazol on intracranial atherosclerosis (ICAS). The investigators randomized 135 Korean patients with acute symptomatic stenosis in the middle cerebral artery or basilar artery into either the cilostazol or placebo group. Aspirin (100 mg/day) was also administered to all patients. The degree of stenosis was assessed at the time of enrollment and six-months after treatment using magnetic resonance angiography and the transcranial Doppler test. Progression of symptomatic stenosis occurred in 6.7% of the cilostazol group, and in 28.8% of the placebo group. Furthermore, the regression rate was higher in the cilostazol (24.4%) than in the placebo (15.4%) group. The differences were significant both for the progression (P = 0.008) and overall changes of stenosis (P = 0.018).
The similarly designed, TOSS II study compared the efficacy of dual antiplatelet therapies (aspirin plus cilostazol vs. aspirin plus clopidogrel) in the management of symptomatic ICAS (6). Medication was administered for seven-months, and progression of intracranial stenosis was assessed. Progression occurred in 20 patients in the cilostazol group (9.3%) and in 32 from the clopidogrel group (15.5%). The difference was not statistically significant (P = 0.092). However, the overall change in the stenosis was more favorable (i.e., less progression and more regression) in the cilostazol group (P = 0.049). These results are consistent with studies showing that long-term administration of cilostazol reduced the intima-media thickness in diabetic (14,15) and non-diabetic patients (13,16).
Another trial, Cilostazol-Aspirin Therapy against Recurrent Stroke with Intracranial Artery Stenosis (CATHARSIS) recruited 163 Japanese patients with ischemic stroke due to ICAS and compared aspirin plus cilostazol vs. aspirin monotherapy (12). Unlike TOSS studies, the patients were recruited from two-weeks to six-months after stroke onset and treated with study medication for two-years. The progression rate during two-year observation period was much lower than that of previous TOSS studies, and occurred in similar frequency between the two treatment groups. This unexpectedly lower rate of ICAS progression may be attributable to the improvement of risk factor management and inclusion of relatively chronic patients. However, certain combined secondary end-points, such as stroke and silent brain infarcts, occurred less frequently (P = 0.04) in the cilostazol group.
In patients undergoing coronary artery stenting, the usual treatment with aspirin and clopidogrel occasionally fails to suppress platelet aggregation, which may be reversed with additional cilostazol treatment (17,18). An improvement in antiplatelet activity in chronic ischemic stroke patients following the administering of cilostazol was also found by Lee et al. in a trial involving 244 chronic aspirin users with ischemic stroke (8). Resistance was decreased by the addition of cilostazol compared with placebo.
Finally, the Effect of Cilostazol in Acute Lacunar Infarction Based on Pulsatility Index of Transcranial Doppler (ECLIPse) study was conducted using transcranial Doppler tests to investigate the effect of cilostazol on the pulsatility index (PI) of middle cerebral and basilar arteries (3). Patients with acute lacunar infarction (n = 203) were randomized into a cilostazol and placebo group. Cilostazol treatment significantly reduced the PI, which may be related to vasodilatation or improvement of endothelial function mediated by cilostazol. The clinical significance of this result remains to be investigated.
The results of meta-analysis of cilostazol research
Six trials compared the efficacy of cilostazol with that of placebo with respect to various clinical or surrogate end-points. Another five trials compared the efficacy and safety of cilostazol against aspirin (or clopidogrel in one trial). As shown in Fig. 1, compared with placebo, cilostazol treatment significantly reduced the risk of ischemic stroke recurrence [risk ratio (RR) = 0.58; 95% CI = 0.40–0.84; P = 0.004], and did not increase the risk of hemorrhagic stroke (RR = 0.62; 95% CI = 0.23–1.64; P = 0.33). Therefore, cilostazol treatment in ischemic stroke patients significantly reduced the risk of overall stroke (RR = 0.58; 95% CI = 0.41–0.82; P = 0.002). Compared with aspirin or other antiplatelets, cilostazol treatment did not reduce the risk of ischemic stroke significantly (RR = 0.85; 95% CI = 0.65–1.10; P = 0.22). However, it markedly (by 61%) reduced hemorrhagic stroke (RR = 0.39; 95% CI = 0.25–0.61; P = 0.0001).
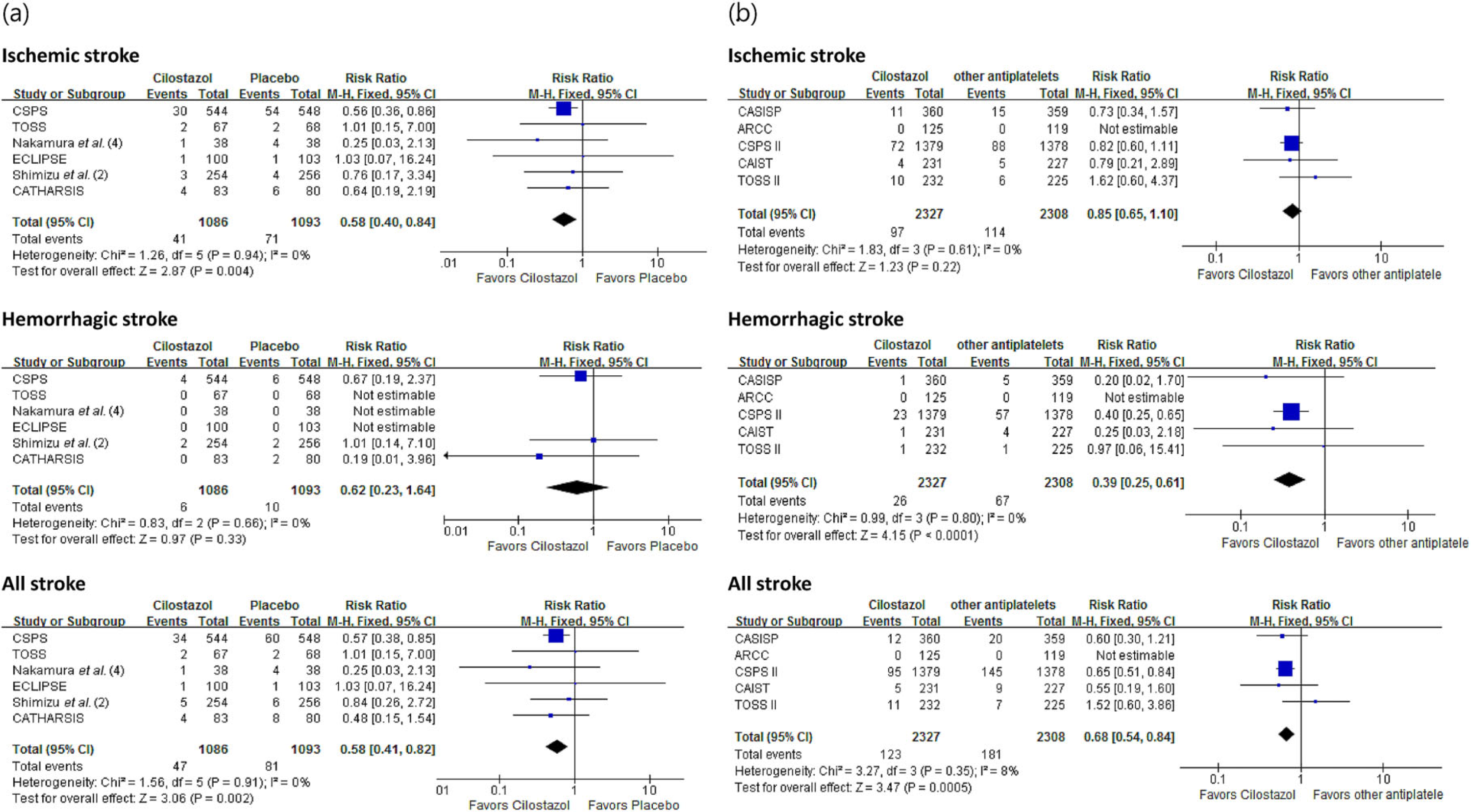
Meta-analysis of cilostazol research conducted in Asia, (a) Cilostazol vs. Placebo, (b) Cilostazol vs. other antiplatelet agents.
Are there patients who would benefit more from cilostazol treatment?
Based on the studies discussed, there seem to be three types of patients who would particularly benefit from cilostazol treatment.
Patients with a high risk of bleeding complications, including those with small vessel disease (SVD)
Increased risk of bleeding is the primary concern when antiplatelets are used in stroke patients. Results from animal (19) and human (7,9) studies and our own meta-analysis (Fig. 1) have shown that cilostazol causes fewer bleeding complications than aspirin. The relative safety of cilostazol can be explained by several observations. First, it was demonstrated that bleeding time – reflecting in vivo physiological hemostasis – was prolonged by aspirin or clopidogrel, but not by cilostazol. Moreover, an increase in bleeding time was not observed when cilostazol was co-administered with aspirin or clopidogrel in patients with peripheral arterial disease (Fig. 2) (20). These results suggest that unlike aspirin or clopidogrel, cilostazol does not affect physiological hemostasis and thus does not increase bleeding risk. Second, cilostazol has an endothelial protective effect and prevents blood-brain barrier disruption in the ischemic brain (19,21). This involves up-regulation of nitric oxide (22,–25), and suppression of adhesion molecules (26,27), cytokines (28), and free radicals (28). Additionally, in a murine stroke model, cilostazol has been shown to protect microvasculature in the ischemic brain by reducing matrix metalloproteinase-9 activity (29). These results support the explanation that the endothelium-protective effect of cilostazol lowers the risk of intracranial hemorrhages.
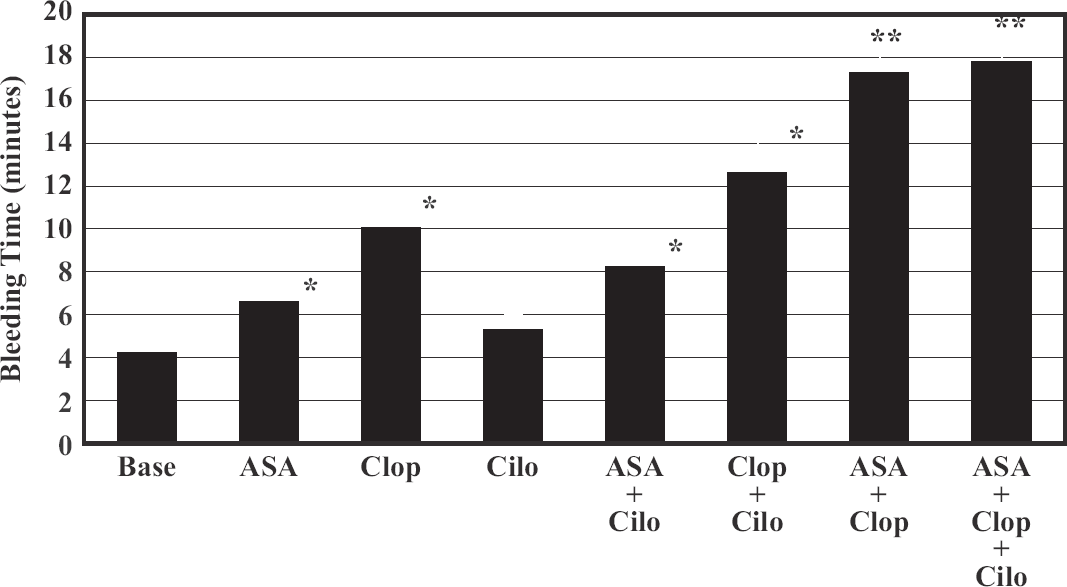
Average bleeding time for each treatment phase in patients with peripheral artery disease. Base, baseline bleeding time; ASA, aspirin 325 mg QD; Clop, clopidogrel 75 mg QD; Cilo, cilostazol 100 mg BID. *P < 0.05 vs. baseline, **P < 0.05 vs. all single agents and vs. ASA + Cilo and Clop + Cilo.
Therefore, cilostazol may be particularly useful in patients with SVD, which is associated with disorganized endothelium due to hypertension and carries a high risk of bleeding when antiplatelets are used. In the subgroup analysis of the CSPS2 study, a significant difference between the cilostazol and aspirin groups was observed with respect to the incidence of hemorrhagic stroke in patients with lacunar stroke (Fig. 3) (30). In another subanalysis that considered patients' blood pressure, the difference in the incidence of hemorrhagic stroke was particularly prominent in patients with systolic blood pressure ≥140 mmHg than in those with lower blood pressure (Fig. 4). Therefore, cilostazol seems to be safer than aspirin in terms of the risk of hemorrhagic stroke, especially in hypertensive, SVD patients.
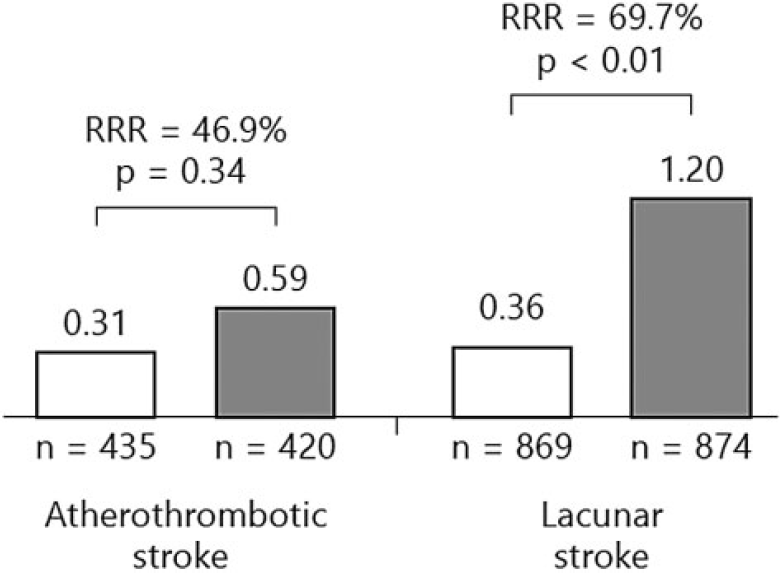
Subgroup analysis between ischemic stroke subtypes in CSPS2 study. There was no significant difference in the incidence of hemorrhagic stroke between both groups among patients with atherothrombotic stroke, while the incidence of hemorrhagic stroke was much lower among patients with lacunar stroke in the cilostazol than in the aspirin group. RRR, relative risk reduction.
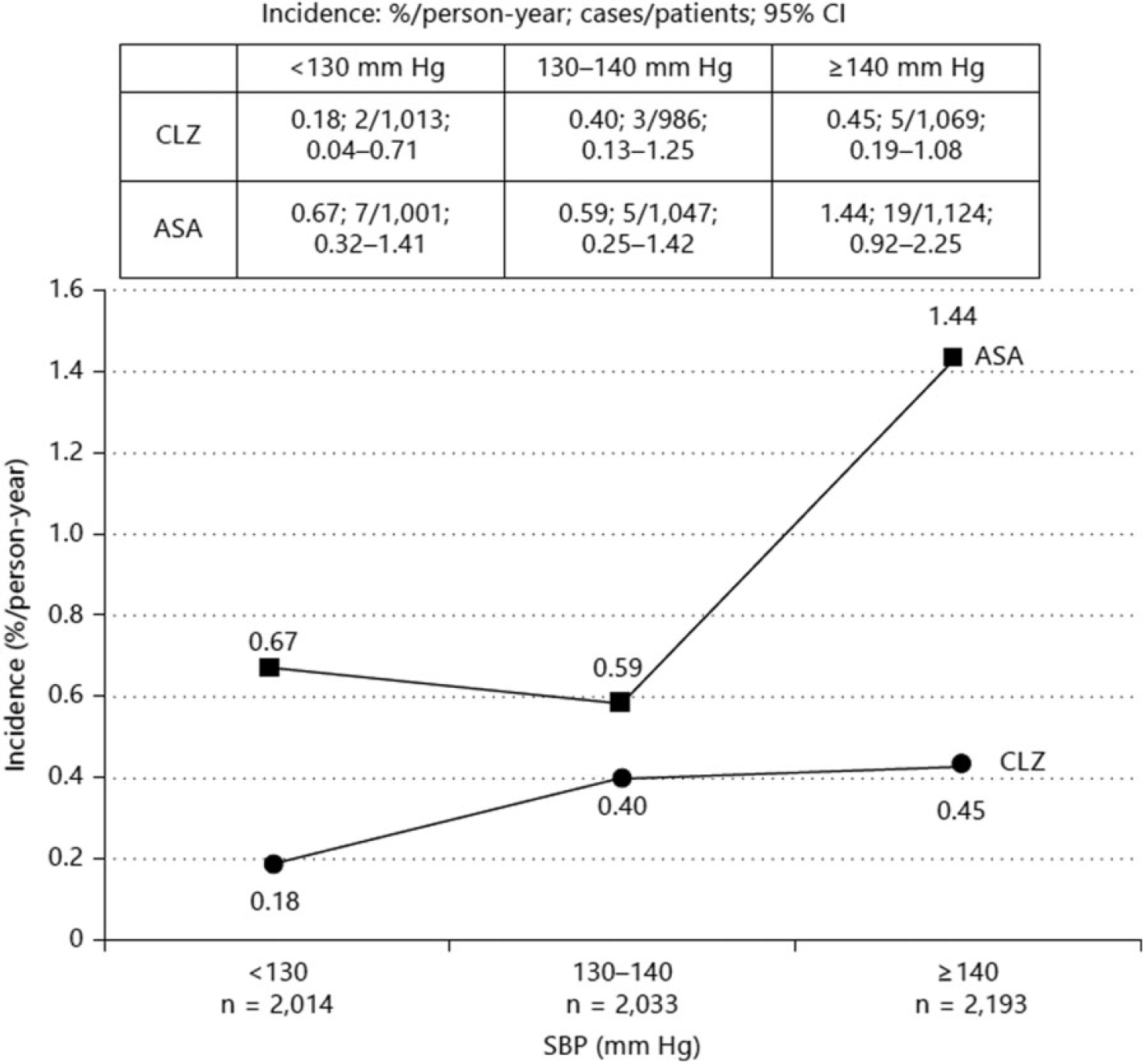
Incidence of hemorrhagic stroke according to systolic blood pressure categories. P = 0.61 for interaction; P < 0.01 for treatment. In this figure, ‘patients’ mean number of patients who showed the classified value at least once. ASA, aspirin; CLZ, cilostazol.
Patients with symptomatic ICAS
As described above, the TOSS I, TOSS II studies showed that cilostazol is beneficial when the overall changes in symptomatic ICAS are taken into account. This beneficial effect may be attributed to either endothelial stabilization or inhibition of vascular smooth muscle proliferation. A favorable effect on lipid concentrations such as an increase in high-density lipoprotein (HDL) mediated by cilostazol is also a potential mechanism (31). The primary end-points in these studies were the magnetic resonance angiogram changes, but not clinical events. However, because progressive narrowing of arteries in ICAS patients is closely related to stroke recurrence (32), the results may be clinically extrapolated.
Asian patients
The incidence of SVD is higher in Asians than in Caucasians (33,34), as is intracranial hemorrhage associated with antiplatelet use. For example, the annual incidence of hemorrhagic stroke with aspirin in clinical trials for secondary stroke prevention was 0.17–0.28% in global trials such as the Clopidogrel vs. Aspirin in patients at Risk of Ischemic Events (CAPRIE) (35), Clopidogrel for High Atherothrombotic Risk of Ischemic Stabilization; Management, and Avoidance in High-Risk Patients (CHARISMA) (36), and the Prevention Regimen for Effectively Avoiding Second Strokes (PRoFESS) studies (37); whereas it was much higher (0.84–1.00%) in Japanese trials such as the Sarpogrerate-Aspirin Comparative Clinical Study for Efficacy and Safety in Secondary Prevention of Cerebral Infarction (S-ACCESS) (38), Japanese Aggrenox Stroke Prevention vs. Aspirin Programme (JASAP) (39), and CSPS 2 studies (7). Moreover, Asians more often have ICAS than Caucasians (40). Therefore, cilostazol may be a safer and more effective choice of antiplatelet for Asian stroke patients (41).
Can Asian research results be applied to non-Asian patients?
Based on the favorable study results from Asia, many Asian countries consider cilostazol a primary drug for treating stroke patients (Table 2). However, cilostazol is less widely recommended by European and American guidelines. For example, although one guideline from the USA reads: ‘In patients with a history of noncardioembolic ischemic stroke or TIA (transient ischaemic attack), we recommend long-term treatment with aspirin (75–100 mg once daily), clopidogrel (75 mg once daily), aspirin/extended-release dipyridamole (25 mg/200 mg bid), or cilostazol (100 mg bid) over no antiplatelet therapy (Grade 1A), oral anticoagulants (Grade 1B), the combination of clopidogrel plus aspirin (Grade 1B), or triflusal (grade 2B)’, cilostazol was considered a less effective agent than others: ‘Of the recommended antiplatelet regimens we suggest clopidogrel or aspirin/extended release dipyridamole over aspirin (Grade 2B) or cilostazol (Grade 2C)’ (42). It seems that although the total number of patients enrolled in the CSPS1, CSPS II, and CASISP studies reaches to 4572, the results from these studies were not considered sufficiently convincing by non-Asian physicians.
Mentions of cilostazol in Asian stroke guidelines
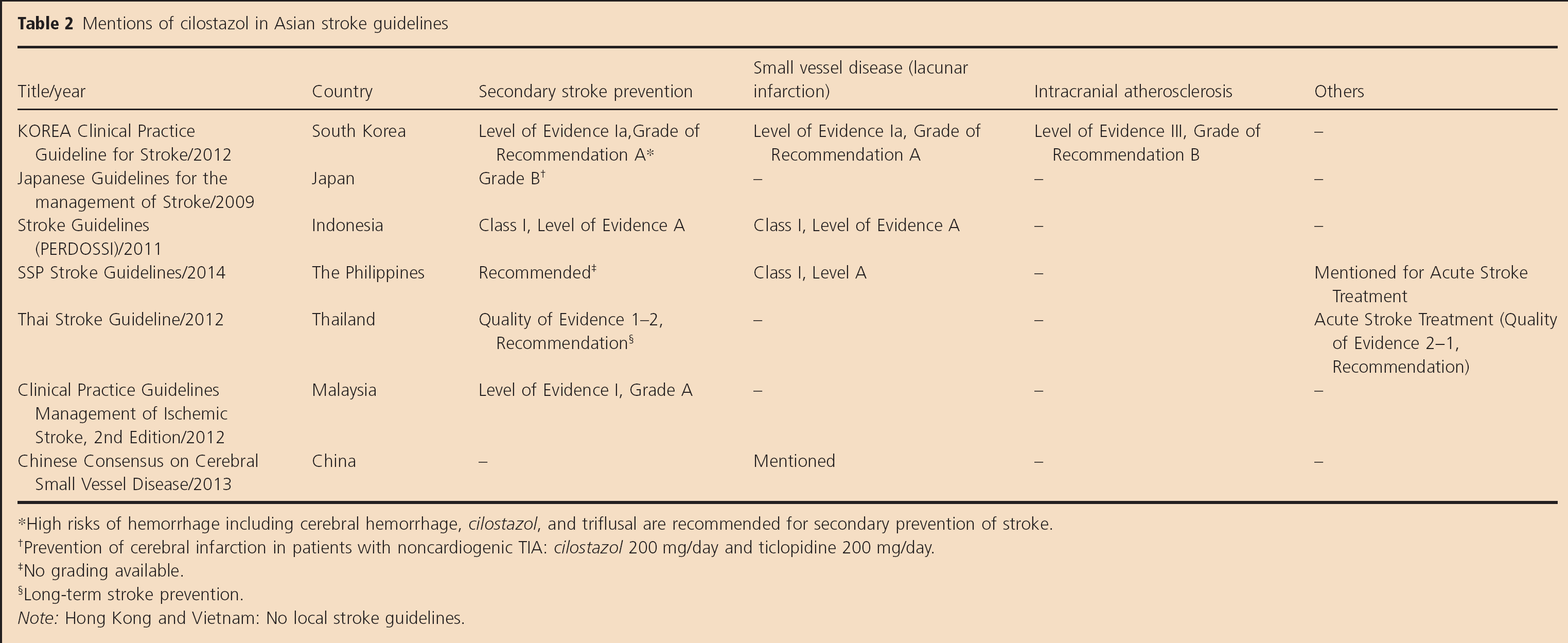
High risks of hemorrhage including cerebral hemorrhage, cilostazol, and triflusal are recommended for secondary prevention of stroke.
Prevention of cerebral infarction in patients with noncardiogenic TIA: cilostazol 200 mg/day and ticlopidine 200 mg/day.
No grading available.
Long-term stroke prevention.
Note: Hong Kong and Vietnam: No local stroke guidelines.
Because TOSS I and TOSS II demonstrated that cilostazol is effective in the prevention of symptomatic ICAS progression, cilostazol is popularly used to treat ICAS patients in Asia (Table 2). However, it is not mentioned in European guidelines, and not recommended by American guidelines. A recent guideline from the USA states that: ‘For patients with recent stroke or TIA (within 30 days) attributable to severe stenosis (70%–99%) of a major intracranial artery, the addition of clopidogrel 75 mg/d to aspirin for 90 days might be reasonable (Class IIb; Level of Evidence B)’ and that: ‘For patients with stroke or TIA attributable to 50% to 99% stenosis of a major intracranial artery, the data are insufficient to make a recommendation regarding the usefulness of clopidogrel alone, the combination of aspirin and dipyridamole, or cilostazol alone (Class IIb; Level of Evidence C)’ (43).
The results of the TOSS I and TOSS II studies are not accredited probably due to the small number of patients enrolled and the use of surrogate markers rather than clinical end-points. However, studies that are focused on ICAS are rare in the West (44), and TOSS I, TOSS II, and CATHARSIS appear to be the only studies that compared the efficacy of antiplatelets in patients with ICAS. In TOSS II, aspirin plus cilostazol provided more favorable results than aspirin plus clopidogrel, a regimen recommended in the USA guideline, at least when the overall change in the stenosis was considered. Although a larger trial may still be needed to confirm the beneficial effects of cilostazol, patients with ICAS may benefit from aspirin plus cilostazol regardless of race-ethnicity – at least for the prevention of progression of atherosclerosis.
Finally, it seems quite clear that cilostazol is safer than aspirin and probably safer than other antiplatelets in terms of reducing bleeding complications, especially hemorrhagic strokes. All the previous results are directed to the same conclusion. Therefore, even in Europe and America, patients with bleeding prone conditions, such as those with SVD (especially with multiple microbleeds) or patients who experienced hemorrhagic strokes, are likely to benefit from cilostazol.
In conclusion, we think that large trials including European and American patients are still needed. Nevertheless, based on current evidence, we suggest that at least a certain group of patients would readily benefit from cilostazol, regardless of ethnicity.
Author contributions
The authors contributed to writing, reviewing, and revising of the manuscript. They also take full responsibility for the content and expression of the submitted manuscripts.