
Abstract

About two-years ago, an editorial in this journal entitled The Razors Edge* (1) reviewed the situation around transvascular stroke treatment after the three negative trials presented at the International Stroke Conference in Honolulu, 2013 (what seemed like the doomsday for endovascular treatment) and was published February 2013 (2–4).
The use of old device types, long treatment times, the high number of patients treated outside the trials, underestimation of the recombinant tissue plasminogen activator (rtPA) response, and inclusion of far distal vessel occlusions were identified as reasons for the failure of these trials. At that time, several trials were already recruiting and a few more were planned. The uncertainty that arose from the negative trials resulted in a massive attitude change among endovascular trialists. It was now understood that the whole approach was at risk (the razor's edge) and that more futile trials could result in completely abandoning a promising therapeutic approach. It was agreed that randomization was key and they stopped treating patients outside the trials. The fact that a governmental decision in the Netherlands granted reimbursement for endovascular treatment only in the context of a randomized trial was also helpful. The new trials had much faster recruitment rates, short treatment time windows, included mostly proximal occlusions, had co-treatment with rtPA, and used new-generation stent-retrievers.
The news
Within seven-months, we received welcome news from seven randomized clinical trials of endovascular recanalization using new devices, mostly so-called stent-retrievers (5–11). Table 1 gives a summary of the most important trial characteristics; however, it is interesting to review the sequence of events.
Synopsis of the recent IAT trials (modified after Grotta and Hacke (12))
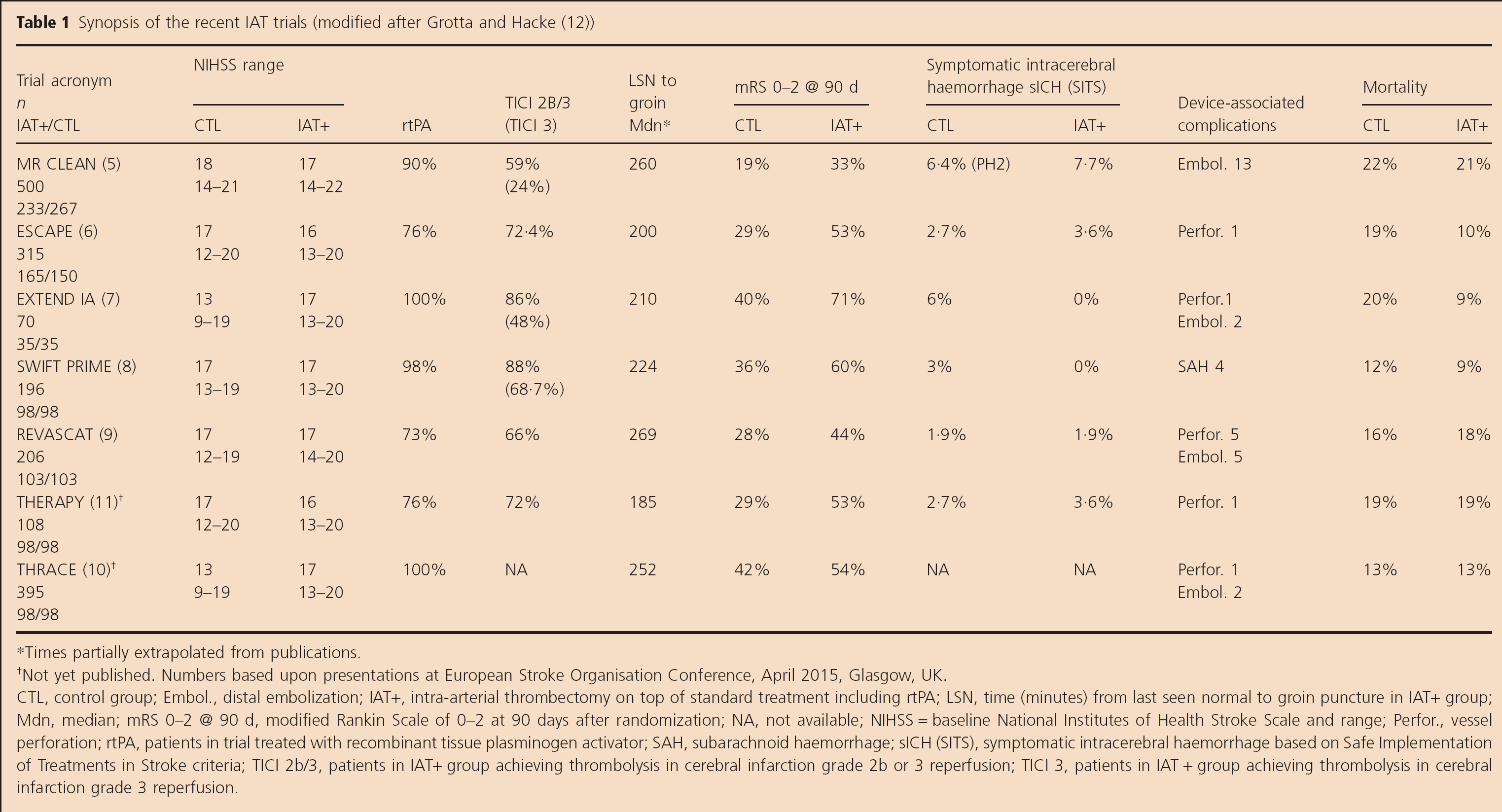
Times partially extrapolated from publications.
Not yet published. Numbers based upon presentations at European Stroke Organisation Conference, April 2015, Glasgow, UK.
CTL, control group; Embol., distal embolization; IAT+, intra-arterial thrombectomy on top of standard treatment including rtPA; LSN, time (minutes) from last seen normal to groin puncture in IAT+ group; Mdn, median; mRS 0–2 @ 90 d, modified Rankin Scale of 0–2 at 90 days after randomization; NA, not available; NIHSS = baseline National Institutes of Health Stroke Scale and range; Perfor., vessel perforation; rtPA, patients in trial treated with recombinant tissue plasminogen activator; SAH, subarachnoid haemorrhage; sICH (SITS), symptomatic intracerebral haemorrhage based on Safe Implementation of Treatments in Stroke criteria; TICI 2b/3, patients in IAT+ group achieving thrombolysis in cerebral infarction grade 2b or 3 reperfusion; TICI 3, patients in IAT + group achieving thrombolysis in cerebral infarction grade 3 reperfusion.
Chapter 1
The Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) trial was presented at the World Stroke Congress in Istanbul, October 25, 2014. The results showed undisputed superiority for the endovascular approach in a trial that had about 85% rtPA co-treatment and 90% use of stent-retrievers, and included 500 patients across 17 centers in the Netherlands. The paper was published in December 2014 (5).
Chapter 2
Several of the other ongoing trials were put on hold, their Data and Safety Monitoring Boards performed interim analyses, and two trials [Endovascular Treatment for Small Core and Anterior Circulation Proximal Occlusion with Emphasis on Minimizing CT to Recanalization Times (ESCAPE), November 6, 2014 and Extending the Time for Thrombolysis in Emergency Neurological Deficits — Intra-Arterial (EXTEND IA), November 4, 2014] were stopped for overwhelming efficacy. Solitaire with the Intention for Thrombectomy as Primary Endovascular Treatment (SWIFT PRIME), the only industry-sponsored trial of the four trials, was also put on hold in November; the formal first interim analysis planned for 200 patients was performed after 196 patients followed up for three-months and the trial was stopped on February 4,2015.
Chapter 3
The three new trials were presented at the International Stroke Conference in Nashville, February 15, 2015, and all had strikingly positive results (Table 1).
Chapter 4
Three further trials, put on hold and terminated in the meantime — Randomized Trial of Revascularization with Solitaire FR Device versus Best Medical Therapy in the Treatment of Acute Stroke Due to Anterior Circulation Large Vessel Occlusion Presenting within Eight Hours of Symptom Onset (REVASCAT), Trial and Cost Effectiveness Evaluation of Intra-Arterial Thrombectomy in Acute Ischemic Stroke (THRACE), and The Randomized, Concurrent Controlled Trial to Assess the Penumbra System's Safety and Effectiveness in the Treatment of Acute Stroke (THERAPY) — are published (REVASCAT) and presented at the European Stroke Organisation (ESO) Conference, April 17 and 18, 2015 in Glasgow, Scotland (THRACE, THERAPY, REVASCAT).
What do the trials have in common?
The use of new-generation stent-retrievers, mostly Stent-Retrievers, early treatment under six-hours to reperfusion, hub and spoke approaches, selection of appropriate severe stroke patients with large vessel occlusion, and rtPA co-treatment in the far majority of patients seem to be overarching principles of the trials.
Despite some variations in imaging and clinical inclusion criteria, the seven new trials had many aspects in common (Table 1). All patients had at least computed tomography-angiography (CTA) confirming vessel occlusion prior to decision for intra-arterial thrombolysis (IAT) and plain CT without (MR CLEAN) or with (ESCAPE, SWIFT PRIME) assessment of Alberta Stroke Program Early CT score (ASPECTS) (5) 6–10 scores. Assessment of collaterals and mismatch imaging was only performed in about 140 patients and seemed to provide additional precision in identifying best responders (EXTEND IA, SWIFT PRIME).
The overall effect on outcome was lowest in MR CLEAN, the trial with the broadest (imaging) inclusion criteria. Only 14% of the control patients (87% rtPA) in a 4·5-h time window reach a modified Rankin Scale (mRS) of 0–2, and the response rate of 33% in the endovascular arm is also very low compared with the other, more selective trials. Outcome data from REVASCAT, which allowed a slightly longer time window and included rtPA failures, were also relatively low in both treatment arms. Using broad inclusion also resulted in more patients with larger infarct core and more advanced ischemic injury, which is also reflected in the rate of patients subsequently undergoing hemicraniectomy. It is worth mentioning that at least three of the seven trials also showed significantly lower mortality rates associated with endovascular treatment, which was so far only seen for hemicraniectomy (6,7,10).
Not surprisingly, recanalization rates with stent-retrievers were far superior to standard rtPA in all trials. Recanalization also differed between the trials, with SWIFT PRIME showing the highest centrally adjudicated thrombolysis in cerebral infarction (TICI) 3 percentages ever reported.
For which patients and conditions do the results apply?
The enthusiasm for these positive trials is understandable, but researchers must remain cautious not to over-interpret the results and prematurely lobby for massive changes in stroke care systems, which may apply only to a limited number of patients.
The results refer to a population of stroke patients with the following characteristics: severe stroke [National Institutes of Health Stroke Scale (NIHSS) median 17], proven internal carotid artery terminal or M1 occlusion (M2 under 8%), CT selection with plain CT (n = 500), with Aspects Core (n > 400) and penumbral imaging (n = 140), co-treatment with rtPA within 4·5 h in over 90% of cases, and successful recanalization using stent-retriever devices in about five-hours.
Overall, the patients studied represent a relatively small cohort of stroke patients. The results were generated in centers with very well-established stroke management systems, established referral systems, and high rtPA rates in the range of 20–25%, far higher than the respective rates countrywide. It is probably correct to assume that between 20 and 30% of rtPA-eligible patients may become candidates for thrombectomy; in some major referral centers, the numbers may be higher, but that is not generalizable. Under these conditions, high impact on outcome and mortality can be generated, as these are patients that would be left dead or severely disabled if not treated. The high rates of good outcome achieved in some studies are astonishing, but seem to be very robust. Overall, the results of the seven randomized controlled trials (RCTs) do not suggest that treatment with recanalization devices other than stent-retrievers, in a time window beyond six-hours, in patients with very large infarct size at treatment, with mild symptoms, with distal occlusions of the M2, and without rtPA bridging can be recommended.
What we do not know yet?
Do less severely affected patients, that is, M2 occlusion strokes with mild to moderate NIHSS, benefit from IAT? About 95% of patients in above trials had an NIHSS > 12. Uncertainty remains for less severe strokes (which rarely come with proximal occlusions). Uncertainty also remains for patients with a severe stroke, caused by M2 occlusion, which may respond equally well to intravenous (IV) rtPA.
The results published apply for IAT using stent-retrievers. There is no convincing evidence that these results would also apply to other devices such as the Penumbra suction device (THERAPY, which did not show significant superiority) (11) or simple intra-arterial rtPA (although some trial protocols would have allowed for alternatives, none were used).
How much more extrapolation regarding variations of IAT is permissible? Can we assume that the results will also apply for other types of endovascular instruments or maneuvers? While some talk about a class effect for stent-retrievers (although in the far majority, a single stent-retriever brand was used), the results of the trials are not transferrable to suction devices, rotation ablation, or simple mechanical manipulation of thrombus. The results of THERAPY, so far known, indicate a much smaller treatment effect of just 8%, which failed to show superiority in an underpowered early terminated trial. Nevertheless, it is intriguing for other companies with different devices to claim that IAT (and not only stent-retrievers) is now proven beneficial. Another interesting aspect is also how we will deal in the future with technical improvement and innovation and what kind of evidence will we, as scientists and clinicians, require before they enter the market. We should never forget the misleading outcome results reported in the uncontrolled series that finally led to the approval of Mechanical Embolus Removal in Cerebral Ischemia and first-generation Penumbra.
How shall we deal with patients with major early infarct core? In most studies, the protocol required CT-ASPECTS scoring or the application of the one-third rule for patients to be entered into the study. Only MR CLEAN did not require this explicitly. Despite a similar stroke severity, the outcome and mortality results in that trial were the poorest of all seven studies. A considerable number of patients underwent hemicraniectomy (5,13). It seems that stent-retrievers work in this population as well, but it is obvious that one could do better with better selection.
What about the time window? Do patients benefit in >six-hours? The results we received apply to early treatment. Although REVASCAT allowed a longer time window and included rtPA failures, thereby adding 30 min to the endovascular treatment time, the median was still clear below 6 h. We have good evidence that the effect disappears with time. Should we treat those patients arriving six-hours and later, in whom recanalization can be achieved, not before eight- to nine-hours after stroke onset? Probably not.
What about patients not receiving rtPA? There are two scenarios — those who simply do not get it, although they could, and those who are uneligible for rtPA. The new study results largely refer to rtPA co-treatment. Currently, we do not have enough data to make a judgment about non-rtPA patients. Maybe future joint analyses will help to understand this situation better. Do the results also apply for rtPA-uneligible patients? We do not have data to confirm that, but we also face the situation that these are the patients who, if they do not receive mechanical recanalization, will not get any specific treatment. So the suggestion is to treat; however, the evidence is low.
The recent ESO-Karolinska recommendations include the use of IAT in rtPA-uneligible patients (14).
What about peri- and post-interventional treatment? Should we use general anesthesia (GA) or conscious sedation (CS)? Stroke unit, neuro-intensive care unit (ICU), or general ICU? For the latter, we have no data at all. Patients are admitted to the ward that is available irrespective of experience in this new field. What about GA? There are centers and even regions that prefer GA over CS, based on personal preferences. Others claim that outcome may be worse with GA. We have some subgroup data from MR CLEAN, presented orally, that indicate that the advantage of thrombectomy may disappear with GA. However, these are non-randomized subgroups and it is possible that features of the patient's condition, which require GA, also carry a risk for an overall poorer outcome. The pooled analyses and the results of an ongoing single-center RCT (Sedation vs. Intubation in Endovascular Stroke Treatment) (15) may give more insight into this complex issue.
What kind of results can we expect in clinical praxis?
The response rates differ largely between the trials. As with rtPA, off-label treatment will become frequent, influencing the results that we may see in future registries or center reports. Patients will be treated late, with large infarct cores and more distal occlusions. It may be that the results that we will generate in everyday practice will be close to those of MR CLEAN, simply because the patient population may be similar. The phenomenal response rates of >60% mRS and under 10% mortality will probably only be reachable in single, high-class, and high-volume centers treating highly selected patients only. The broader the use of thrombectomy will be, the more patients with limited response will be included. Nevertheless, the significant advantage over single rtPA in these relatively severe patients will prevail.
How many interventional stroke centers are necessary and what needs to change in our management structures?
Let's try to guess how many patients will be candidates for endovascular treatment.
As a rule of thumb, a stroke center that admits 1000 acute ischemic stroke (AIS) patients per year may have an IV thrombolysis rate of 25% (16). Such a center usually serves as a hub for several connected smaller stroke units and will receive transferrals [not only for thrombectomy and AIS, but also for intracerebral haemorrhage, subarachnoid haemorrhage (SAH), aneurysm coiling or clipping, decompressive surgery, and other neuro-ICU conditions]. Such a center may have between 80 and 150 transvascular interventions for AIS, which is about 10% of the patients presenting with AIS. This seems to be an acceptable number to achieve enough expertise and to base successful training programs upon. Such a center can usually cover a catchment area of roughly one million inhabitants; this is how the MR CLEAN trial was able to cover a country with 17 million inhabitants and be so successful. It is important to mention that these centers take care of a reasonably large number of acute SAH cases and other elective endovascular procedures and usually have several endovascular specialists.
Similar to other fields in medicine, minimum numbers must be linked to the certification of interventional centers. The Comprehensive Stroke Center concept with coordinated, expert, multidisciplinary teams from pre-hospital to endovascular suite is essential for delivering the best possible results. Creating endovascular centers for AIS only seems not to be a wise idea. Smaller comprehensive stroke centers with less than 300–400 acute admissions per year may not reach the critical number of interventions to call it routine practice. Working day and day time-only services provided by a single interventionalist or five full transvascular programs in a city of 500 000 inhabitants are not desirable, but they will be created.
Patients with suspected large artery occlusion and who may be IAT candidates should be taken or sent to a center with 24/7 endovascular capability if logistics would allow onset to groin within six-hours of last seen normal. Under no circumstances should we wait for a lack of rtPA response — it is not about rtPA failures, but about the combination of rtPA and IAT.
The improvement of pathways to select candidates' transferal to major centers based on clinical features, CT (or magnetic resonance imaging) imaging, and maybe vascular imaging, although not for every transfer should a CTA be required. This is especially true when the transfer time will be longer than an hour, which would prompt the center to repeat the CTA on arrival to check whether the occlusion is still present. We need to get consensus about how to select patients for endovascular procedures in community hospitals.
Outlook
The results of REVASCAT, THRACE, and THERAPY (9–11) were presented in April at the ESO Conference in Glasgow and widely supported the results of the previous trials. Two trials showed positive results for the primary end-point; only the trial using non-stent-retriever devices (THERAPY) failed.
Stroke treatment will change. We will have to increase the number of endovascular centers in countries with a well-financed health system, but not to the extent some of us believe. We will need to further improve referral and stroke pathways. Stroke management systems will become more expensive. And we will see the gap between stroke medicine in high income regions and the others increase further. Over time changes will come also to underpriviledged regions.
Are you ready*? Currently, only few regions are.