
Abstract
Background
Controversy exists regarding the question of whether weight change decreases or increases the risk of mortality.
Aim
The aim of this study was to evaluate the prognostic importance of weight change on short-term outcomes in acute ischemic stroke patients.
Methods
A total of 654 patients with acute ischemic stroke were enrolled in this study from March 2010 to May 2013. We assessed the weight change of each participant between admission and discharge from the Department of Neurology. Weight change was defined as change ≥0.05 kg/baseline body mass index unit. We evaluated the short-term outcomes using a modified Rankin Scale at three-months after the onset of a stroke.
Results
Among the 654 patients, 35.2% were included in the weight-change group. Weight loss occurred in 24.6% of the participants during the hospital stay following the stroke, which lasted an average of nine-days. Compared with the weight-stable group, the pronounced weight-loss group had a higher risk of unfavorable outcomes (odds ratio 2.43; 95% confidence interval 1.12-5.25).
Conclusions
Short-term weight loss after stroke appears to be more common than we expected, and our results suggest that it is associated with unfavorable functional outcomes. Therefore, clinical nutrition should be considered as a component of medical treatment and weight loss should be monitored as an indicator of malnutrition.
Introductions
The prevalence of obesity has increased and has reached epidemic levels worldwide (1). Obesity is a significant risk factor for the development of cardiovascular disease and is associated with all-cause death (2–4). It is universally recommended that those who are overweight or obese should lose weight (5). Weight reduction in patients with metabolic syndrome is thought to be desirable because it helps to reduce plasma renin activity and improve glycemic control (6,7). Conventionally, the intentional loss of weight was shown to result in a reduced risk for the development of disorders associated with obesity (8–10). However, recent guidelines for the prevention of stroke suggested that despite the demonstrated beneficial effects of weight loss on cardiovascular risk factors, usefulness of weight loss among patients with a recent transient ischemic attack (TIA) or ischemic stroke is uncertain (11).
Furthermore, recent studies have documented a puzzling phenomenon, referred to as the ‘obesity paradox’, in which overweight and obese subjects have a better prognosis compared with normal-weight individuals (12–15). Obese patients might have more metabolic reserves in catabolic states, such as heart failure, chronic kidney disease, and stroke (16–19). Although this ‘obesity paradox’ has been reported in a number of clinical studies, little is known about the effect of weight loss on prognosis (13).
Controversy exists regarding the question of whether weight loss decreases or increases the risk of mortality. Several studies have demonstrated that weight gain or weight fluctuation resulted in a significantly higher mortality risk than the maintenance of a stable weight (20,21). By contrast, some reports have indicated that weight loss may be associated with an increased mortality risk (5,7,20,22,23). It is noteworthy that weight loss after stroke is a common observation, and no less than a quarter of patients who were in good physical condition before the onset of a stroke experienced weight loss in the short term as well as the long term following the stroke (24,25). Therefore, the aim of this study was to evaluate the prognostic importance of weight change for the short-term functional outcomes in patients with acute ischemic stroke.
Methods
Study population
We enrolled a consecutive series of patients with acute ischemic stroke or TIA who were admitted within seven-days of the onset of symptoms to our stroke center from March 2010 to May 2013 into our prospective stroke registry system. Initially, we included a total of 732 patients. All patients were followed through telephone interviews or medical records via outpatient care. From this population, we excluded patients with errors in their hospital charts (n = 13), lack of records regarding weight at discharge (n = 7), and follow-up loss (n = 28). Additionally, patients with the length of the hospital day over 30 days (n = 30) were also excluded. Because the aim of this study was to evaluate the impact of weight change during acute ischemic stroke on short-term functional outcomes, very long duration of hospital stay might affect the interpretation of the result. As a result, a total of 654 patients participated in this study (Fig. 1).
Flow diagram for weight-change group of the ischemic stroke. Patients were divided into five groups with regard to weight change: those with pronounced weight gain or loss (>0.1 kg/baseline BMI-unit), those with mild weight gain or loss (≥0.05-0.1 kg/baseline BMI-unit), and those with a stable weight (<0.05 kg/baseline BMI-unit). BMI, body mass index.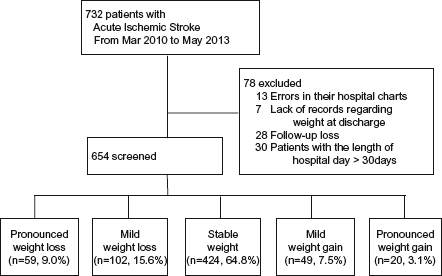
All patients received standard, optimal medical therapy during their hospitalization. The institutional review board of Seoul National University Hospital (1408-049-600) approved the study protocol, and written informed consent was obtained from all participants or from the next of kin when the patient's agreement was not possible.
Clinical information
All patients underwent diagnostic tests, including routine blood tests, neuroimaging, and cardiac studies. We collected baseline demographic and clinical information for all study participants, including age at onset, gender, hypertension (previous use of antihypertensive medication, systolic blood pressure >140 mmHg or diastolic blood pressure >90 mmHg at discharge), diabetes [previous use of anti-diabetic medication under the diagnosis of diabetes, fasting blood glucose >7.0 mmol/L (>126 mg/dL) at discharge], dyslipidemia [previous use of lipid-lowering medication, total cholesterol >6.0 mmol/L (>240 mg/dL), or low-density lipoprotein cholesterol >4.14 mmol/L (>160 mg/dL) at admission], smoking (ever- or never-smoking), history of stroke, and history of heart disease before the occurrence of stroke. The comorbid diseases included in this study were chronic renal failure, chronic obstructive pulmonary disease, liver cirrhosis, and cancer.
We measured the body weight and height at admission and then measured the body weight again at discharge. In cases that were referred to other departments, we measured the weight at the time of discharge from the Department of Neurology. Body weight was measured using a calibrated automatic height and weight scale (Model GL-150, G-Tech International, Uijeongbu-si, Gyeonggi-do, South Korea) by the skilled nurse, with hospital gown and shoes off. In cases of severe stroke, we measured the body weight using an under-bed scale, and the height was measured using a tapeline. The body mass index (BMI) was calculated as the weight (kg) divided by the square of the height (m). For the classification of BMI, we used the guidelines for an Asian-Pacific population. Weight change was predefined as weight gain or weight loss of >0.05 kg per baseline BMI-unit, as described in a previous study (23). We assumed that this definition was more reasonable for evaluating weight change than other methods that have been used, defining weight change as a gain or loss of more than 1∼2 kg/m2, a gain or loss of 4∼5% of the body weight, or a gain or loss of more than 3 kg (5,7,8,20,21,26–28). Consequently, for a patient with a BMI of 30 kg/m2, a change of ≥ ±1.5 kg was categorized as a weight change. Patients were divided into five groups with regard to weight change: those with pronounced weight gain or loss (>0.1 kg/baseline BMI-unit), those with mild weight gain or loss (≥0.05-0.1 kg/baseline BMI-unit), and those with a stable weight (<0.05 kg/baseline BMI-unit).
We measured the kilocalorie intake at three-days after stroke onset based on the doctor's diet prescriptions. Because some patients might be on a fasting status during initial one to two-days due to severe neurological deterioration or operability considerations. When patients had dysphagia at the time of admission, we provided sufficient calories through the Levin tube, as needed. A calorie surplus was defined as follows: Calorie surplus = Kilocalorie intake (Kcal) at three-days after stroke onset - Basal metabolic expenditure (BME) (29). The BME was calculated by the Harris-Benedict equation established in 1918.
Men: BME (Kcal) = 66 + (13.7) (weight, kg) + (5) (height, cm) − (6.8) (age, years).
Women: BME (Kcal) = 655 + (9.6) (weight, kg) + (1.7) (height, cm) − (4.7) (age, years).
The Harris-Benedict equation is a method used to estimate an individual's BME and daily kilocalorie requirements. The resulting number is the recommend daily kilocalorie intake to maintain current body weight (29,30). The type of meals at three-days was divided into three categories: general diet, tube feeding, and fasting.
The initial neurological severity (INS) was estimated using the National Institutes of Health Stroke Scale (NIHSS) score at admission. Because NIHSS scores were not normally distributed, we classified NIHSS scores into 0-7, 8-14, and ≥15 (31). We classified the stroke subtypes based on the method reported in the Trial of Org 10172 in Acute Stroke Treatment (TOAST). The short-term outcome was estimated using the modified Rankin Scale (mRS) at three-months after stroke onset. The three-month mRS was obtained via an outpatient visit or structured telephone interview. We evaluated the distribution of the weight changes after dichotomizing the mRS at three-months after stroke onset (favorable outcome: three-month mRS 0-2; unfavorable outcome: three-month mRS 3-6) (32).
As a compulsory social insurance, the Korean health insurance (National Health Insurance) covers the whole population living in the country. Therefore, ‘health insurance’ covers approximately 96-97% for the Korean population, and ‘Medicaid’ for the poor covers the remaining 3-4% of the population, with an annual assessment of the poverty status.
Statistical analysis
The distributions of demographic data, clinical features, laboratory findings, hospital duration, and stroke subtype data according to the weight change were analyzed using a χ2 test, Student's t-test, or one-way analysis of variance (ANOVA), as appropriate. The trend in the baseline data was also calculated using the χ2 test for trends in proportion. In the analysis, the associations between weight change and the short-term outcomes were estimated using binary logistic regression analysis. The stable weight (<0.05 kg/baseline BMI-unit) was used as a reference level. For the dependent variables, the patients with a favorable outcome (three-month mRS 0-2) were used as a reference group in the binary logistic regression analysis.
The values for the continuous variables were expressed as the means ± standard deviation (SD). The odds ratios (ORs) and 95% confidence intervals (CIs) are presented in the results and were used to calculate the probability values. A probability value of ≤0.05 was considered statistically significant. Analyses were performed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA).
Results
Among the 654 subjects, the mean age was 66.7 ± 13.0 years, and 38.5% of the participants were women. The mean duration of the hospital stay was 9.4 ± 5.2 days. The baseline demographic and clinical characteristics are shown in Table 1. A total of 230 patients (35.2%) were included in the weight-change group. Approximately a quarter of patients (24.6%) had weight losses (Fig. 2). Patients with pronounced weight loss had higher BMI at admission, smaller calorie surplus at three-days after stroke onset, and more likely to have feeding diet and atrial fibrillation. On the contrary, patients with stable weight had the mildest neurological severity at admission and the shortest length of hospital stay (Table 1). Of the 654 subjects, 171 (26.1%) patients had poor functional outcomes. Figure 3 shows the distribution of the three-month mRS according to the weight change levels. Patients with weight loss had poorer functional outcomes at three-months after stroke onset compared with the patients with stable weight (P for difference <0.001; Fig. 3).
(a) The number of patients according to the weight-change groups in acute ischemic stroke during admission. (b) The proportions of patients according to the weight-change groups in acute ischemic stroke during admission. Distribution of groups of weight-change after dichotomizing modified Rankin scales (mRS) at three-months after stroke onset. Patients were divided into four groups with regard to weight change: those with pronounced weight loss (>0.1 kg/baseline BMI-unit), those with mild weight loss (≥0.05-0.1 kg/baseline BMI-unit), those with weight gain (≥0.05 kg/baseline BMI-unit), and those with a stable weight (<0.05 kg/baseline BMI-unit). BMI, body mass index.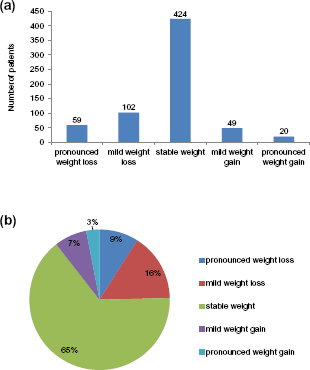

Baseline characteristics grouped by weight change
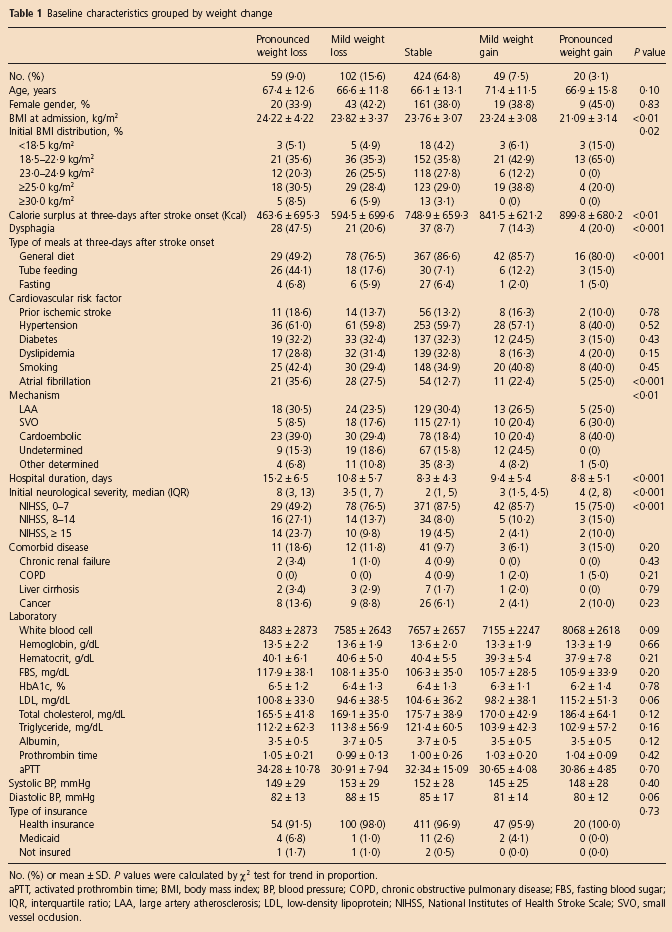
No. (%) or mean ± SD. P values were calculated by χ2 test for trend in proportion.
aPTT, activated prothrombin time; BMI, body mass index; BP, blood pressure; COPD, chronic obstructive pulmonary disease; FBS, fasting blood sugar; IQR, interquartile ratio; LAA, large artery atherosclerosis; LDL, low-density lipoprotein; NIHSS, National Institutes of Health Stroke Scale; SVO, small vessel occlusion.
We evaluated the distribution of the weight change groups after dichotomizing the patients based on the mRS at three-months after stroke onset (favorable outcome: three-month mRS 0-2; unfavorable outcome: three-month mRS 3-6). When compared with the stable-weight group, the pronounced weight-loss group had a higher risk of having unfavorable outcomes after adjusting for age, gender, hypertension, diabetes, dyslipidemia, smoking, atrial fibrillation, caloric surplus at three-days after stroke onset, type of meals at three-days after stroke onset, stroke subtype, hospital days, comorbid diseases, BMI at admission, and INS (OR 2.43; 95% CI 1.12-5.25). As the weight changed from pronounced weight loss to weight gain, the risk of having an unfavorable outcome decreased (mild weight-loss group: OR, 1.31; 95% CI, 0.71-2.40; weight-gain group: OR, 0.57; 95% CI, 0.25-1.31) (Table 2).
Effect of weight changes on short-term outcomes (compared with favorable three-month mRS)
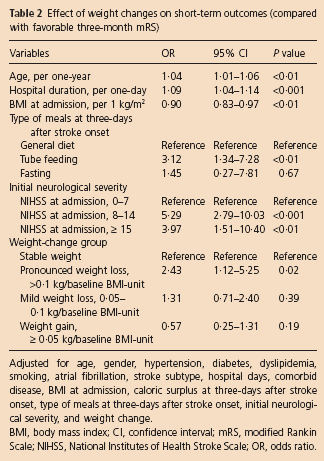
Adjusted for age, gender, hypertension, diabetes, dyslipidemia, smoking, atrial fibrillation, stroke subtype, hospital days, comorbid disease, BMI at admission, caloric surplus at three-days after stroke onset, type of meals at three-days after stroke onset, initial neurological severity, and weight change.
BMI, body mass index; CI, confidence interval; mRS, modified Rankin Scale; NIHSS, National Institutes of Health Stroke Scale; OR, odds ratio.
Additionally, to clarify the associations between the effects of weight change and the functional outcomes, we evaluated further analyses using other definitions of weight change, such as a gain or loss of more than 1 kg or 0.5 kg/m2 BMI-unit. The pattern of significance remained in this analysis (see Table S1).
Discussion
In summary, we found that patients with pronounced weight loss during acute ischemic stroke had poor functional outcomes compared with patients with stable weight. Furthermore, approximately 25% of the participants experienced weight loss during the relatively short average hospital stay of nine-days in our stroke registry. Therefore, we suggest that it is important to monitor weight change during the acute stroke period in terms of treating catabolic imbalance.
It is noteworthy that weight loss after stroke occurred more frequently than we expected, and we had not previously taken the weight loss during admission fully into account. In a population-based study examining weight loss after stroke, weight loss >3 kg was observed in 24% of patients after four-months and in 26% one-year later (24). Similarly, among 4360 patients with coronary artery disease, 24.93% presented weight loss at three-months (23). In our study, it should be noted that weight loss during acute ischemic stroke was not an intentional but an observational result. Unlike the intentional weight loss, observational weight loss seems to be related to poor outcomes (10).
The reasons for the pronounced weight loss during the short-term as well as the long-term periods following a stroke remain to be determined. The body weight change after stroke might impact patients differently than it does healthy subjects. Multifactorial mechanisms, including fluid intake, reduced physical activity, sympathetic activation, and systemic inflammation, may contribute to metabolic imbalances. Because this study was not intended for patients in an intensive care unit (ICU), it was not possible to collect exact information about the fluid balance intake. However, according to the previous reports, the recorded fluid balances were considered unreliable (33,34). Calculated fluid balances are not predictive of actual weight changes in critically ill patients because other factors leading to unintentional weight loss have been found to be important, such as fever, parenteral nutrition, and tracheal intubation (34,35). The net effect of catabolic over-activation is an acceleration of tissue degradation, resulting in muscle loss and overall weight loss (25). Prior studies supporting an ‘obesity paradox’ have demonstrated that obese individuals might have an energy reservoir under catabolic conditions, and therefore, obesity might be correlated with better outcomes (14,36). Despite the fact that BMI was commonly used, it has received a lot of critique in terms of its accuracy to define obesity. Because BMI is an aggregate of lean mass and body fat, estimating body composition is important (37). In one retrospective study, higher lean mass index was clearly protective. Because lean mass has been associated with muscle strength and cardiorespiratory fitness, ‘lean mass index’ might perform an important role for ‘obesity paradox’ (38). However, little is known about the patho-physiological changes that occur in skeletal muscle after a stroke. Numerous data suggest that inflammatory cytokines, such as tumor necrosis factor, may induce tissue degradation and promote weight loss (39,40).
Energy malnutrition in elderly and critically ill patients is an important independent indicator of high morbidity and mortality (41). Current international guidelines suggesting a calorie and protein intake closer to the recommended amounts during the early phase of stay in an ICU are associated with a more favorable outcome (42). In addition, although there is limited evidence that nutritional intervention may improve short-term outcomes, recent guideline recommended that it is reasonable to conduct a nutritional assessment for patients with ischemic stroke (11). In our study, short-term weight loss after stroke is determined by complex mechanisms such as nutritional deficiency, eating difficulties, hemodynamic status, stroke severity, and underlying diseases. Therefore, the loss of weight did not indicate malnutrition per se. However, there is no ‘gold standard’ for determining nutritional status because there is no universally accepted definition of malnutrition (43). Thus, the general loss of body weight is considered to be a gross indicator of a nutritional deficit (30).
The strength of this study is that it is the first report to review the importance of weight loss in patients with acute ischemic stroke. Weight change during the recovery from an acute stroke has been relatively overlooked despite its significance. Our results indicate that many patients with acute ischemic stroke experienced weight loss, even during a brief hospital stay, and weight change should be considered during the follow-up after a stroke to detect unintentional weight loss related to possible malnutrition. However, there are some caveats to this study. First, because this is a retrospective observational study, and unknown factors might have confounded our results. Second, in cases of changing neurological status, modalities to measure weight and height might be different. However, except for some cases, because body weight was measured using a calibrated scale with same protocol, the modalities to measure weight would be matched in the same patients. Third, patients with pronounced weight loss were more likely to have dysphagia. However, even if the patients had dysphagia at the time of admission, we provided sufficient calories through the Levin tube, as needed. Fourth, we did not obtain fluid intake and biochemical parameters such as serum albumin and serum total cholesterol that can be considered as indicators of nutritional status. However, according to the previous reports, the recorded fluid balances were considered unreliable and the serum albumin and total cholesterol levels have limited value because they fluctuated depending on acute phase reactants and statin use. Serum albumin, as a possible marker of malnutrition, is considered to be a poor indicator of nutritional status due to a compensatory decrease in its production by the liver in response to systemic stress of critical illness and an increase in the production of acute phase reactants (24,30). Fifth, preexisting disease may significantly affect the outcome. However, there were no statistically significant differences related to comorbid diseases among the weight-change groups. Furthermore, although preexisting diseases might influence the mortality, they may have fewer impacts on the short-term outcomes compared with the long-term outcomes. Finally, because of short duration of admission, we predefined weight change more strictly than previous reports. Considering the short length of the hospital stay, even mild weight change might be significant in this analysis. To overcome the limitations of our method, we also conducted analyses using other methods and found that the pattern of significance still remained.
Collectively, weight loss during acute ischemic stroke is common and appears to be associated with unfavorable functional outcomes. We suggest that clinical nutrition should be considered as a component of medical treatment, and weight loss should be monitored as an indicator of malnutrition.
Author contributions
B-W. Yoon devised the original study concept and design. C. K. Kim and S. Jung participated in the acquisition of data. Y. Kim and C. K. Kim performed statistical analyses. S-H. Lee and S-B. Ko made intellectual contribution. Y. Kim and B-W. Yoon interpreted the results and wrote the manuscript. All authors read and approved the final manuscript.
Supporting information
Additional Supporting Information may be found in the online version of this article at the publisher's web-site:
Footnotes
Conflict of interest: None declared.