
Abstract
Many studies in humans suggest that altered temporal lobe functioning, especially functioning in the right temporal lobe, is involved in mystical and religious experiences. We investigated temporal lobe functioning in individuals who reported having transcendental “near-death experiences” during life-threatening events. These individuals were found to have more temporal lobe epileptiform electroencephalographic activity than control subjects and also reported significantly more temporal lobe epileptic symptoms. Contrary to predictions, epileptiform activity was nearly completely lateralized to the left hemisphere. The near-death experience was not associated with dysfunctional stress reactions such as dissociation, posttraumatic stress disorder, and substance abuse, but rather was associated with positive coping styles. Additional analyses revealed that near-death experiencers had altered sleep patterns, specifically, a shorter duration of sleep and delayed REM sleep relative to the control group. These results suggest that altered temporal lobe functioning may be involved in the near-death experience and that individuals who have had such experiences are physiologically distinct from the general population.
Most individuals react to a life-threatening trauma with intense fear and anxiety that often lasts well after the threat has subsided. A number of trauma survivors go on to develop posttraumatic stress disorder (PTSD), which is characterized by flashbacks, nightmares, and significant distress. In contrast, a few people experience the trauma as a peaceful, joyful, and otherworldly event known as a “near-death experience”; this experience is often associated with long-term positive changes, notably, decreased fear and anxiety and increased positive affect (Greyson & Stevenson, 1980; Groth-Marnat & Summers, 1998). The typical near-death experience includes transcendence of space, time, and self; feelings of peace and euphoria; and an encounter with a bright light, religious figures, or deceased relatives (Greyson & Stevenson, 1980). This atypical response to life-threatening trauma and its positive aftereffects are in stark contrast to those seen in PTSD, but have received very little scientific attention.
The reason for this atypical reaction to trauma remains unknown. Nonetheless, the involvement of the temporal lobes is suggested by observations that electrical stimulation of the temporal lobe (Jasper & Rasmussen, 1958) and seizures in temporal lobe epileptics (Daly, 1975; Devinsky, Feldman, & Burrowes, 1989) can evoke similar mystical experiences. The acute stress or hypoxia during a life-threatening event may hypersensitize neurons and lower seizure thresholds, especially in the temporal lobe (Benveniste, Brejer, Achouseboe, & Diemer, 1984). Near-death experiencers and temporal lobe epileptics share the tendency to be transformed by their experiences and take on new spiritually oriented interests and values (Groth-Marnat & Summers, 1998; Waxman & Geschwind, 1975). Because of the similarities between temporal lobe epileptics and near-death experiencers, we hypothesized that compared with control subjects, near-death experiencers would show more signs of altered temporal lobe functioning, specifically, more interictal (between-seizure) epileptiform waveforms and temporal lobe epileptic symptoms. On the basis of previous theories (Morse, Venecia, & Milstein, 1989), we hypothesized that any brain abnormalities found in this population would be lateralized to the right side.
Because sleep increases the likelihood of epileptiform activity (Malow, 1996), we used an overnight polysomnographic (PSG) sleep study to screen for temporal lobe epileptic or paroxysmal discharges, and a questionnaire to assess temporal lobe epileptic symptoms. In addition, we used a number of other questionnaires to assess whether the near-death experience was associated with dysfunctional stress reactions like dissociation and other PTSD symptoms or with functional coping styles.
METHOD
Participants
A total of 43 participants (30 females, 13 males; 25–75 years old, mean age=52.75) gave written informed consent before participating in the study. Individuals who reported having had a near-death experience (n=23, mean age=53.04 years, range: 25–71) were recruited through a local support group (34.8%) and through local advertisements (65.2%). Inclusion into the near-death-experience (NDE) group required life-threatening physical distress as the result of an accident or other injury and a minimum score of 7 on the Near-Death Experience Scale (Greyson, 1983). Life-threatening events included accidents (43.5%), medical complications (17.4%), heart attacks (17.5%), allergic reactions (8.7%), and suicide attempts (8.7%). Head trauma was sustained in 21.7% of the accidents. Life-threatening situations before the age of 5 years were not included.
Control participants (n=20, mean age=52.5 years, range: 25–75) were age and gender matched to members of the trauma group and scored below 7 on the Near-Death Experience Scale. Control participants had no history of life-threatening illness or injury, combat experience, or the loss of a loved one in the last year. They were medically healthy, with no history of head injury or seizures or family history of epilepsy. In addition, control subjects had no current sleep problems and a sleep efficiency (total sleep time/total record time) of better than 60% during the study night. NDE participants and control subjects did not differ in age, level of education, or Mini-Mental Status exam score. The NDE group scored significantly higher (p<.001) on the Near-Death Experiences Questionnaire (M=20.16±5.52, range=12–32) than the control group (M=1.5±2.22, range=0–6).
Procedure
Participants who met the initial inclusion criteria were scheduled for a sleep study and given a packet of questionnaires to complete and return at the time of that study. Participants were asked to abstain from naps and substances that could interfere with sleep for 24 hr prior to arrival at the sleep lab.
Materials
Participants were asked to complete the Dissociative Experiences Scale (DES; Bernstein & Putnam, 1986), the Civilian Mississippi Scale for PTSD (Keane, Caddell, & Taylor, 1988), the Complex Partial Epileptic Signs (CPES) and Temporal Lobe Symptoms (TLS) subscales of the Personal Philosophy Inventory (Persinger, 1983), and the COPE Inventory (Carver, Scheier, & Weintraub, 1989).
PSG and Electroencephalogram (EEG)
EEG was recorded by scalp electrodes applied according to the International 10-20 System placements, as well as by mastoid and central reference electrodes. In addition, eye movements and electromyographic (EMG) activity were recorded by extraocular and submentalis electrodes. All physiological measurements were digitally recorded using a 32-channel Grass polysomnograph, Aurora model, and Twin 2.0 software (Grass Instrument Division, Astro-Med, Inc., Warwick, Rhode Island), with a sampling rate of 200 Hz, 20K amplification, and a bandpass of 0.1 to 70 Hz with a notch filter. After biological calibrations, subjects were allowed to sleep for 8 hr after sleep onset and were continuously monitored by video camera.
Sleep Parameters
Each study was scored (by the first author) in 30-s sections, or epochs, according to standard sleep-stage scoring guidelines (Rechtschaffen & Kales, 1968). In a randomly selected set of records, agreement of sleep-stage scoring between the first author and a registered PSG technician was found to be greater than 90%. Sleep onset was defined as the first epoch of any stage of sleep.
Detection of Paroxysmal EEG Activity
All records were scored visually (by the first author) and computer scored for any epileptiform patterns, noticeable asymmetries, rhythmic discharges, or other abnormalities. All potential abnormalities were then independently evaluated by a registered EEG technician at the Epilepsy Monitoring Unit at the University of Arizona Health Sciences Center. The visually scored records were viewed at 30 mm/s on an anterior-posterior bipolar montage and scored according to the guidelines of the Terminology Commission of the International Federation of Societies for Clinical Neurophysiology (Chatrian, 1974). These guidelines identify a spike as activity that (a) is one third higher than the activity during the preceding 5 s, (b) has a duration of less than 200 ms, and (c) is accompanied by a field, as defined by the (phase-reversed) involvement of a second adjacent electrode.
RESULTS
No clinically significant seizure activity (EEG or tonic-clonic posturing) was observed in either group, and therefore we use “epileptiform EEG” to refer to interictal activity. Interictal temporal lobe paroxysmal EEG activity was found in 5 (21.7%) near-death experiencers and 1 (5%) control subject during the overnight sleep studies. The hypothesis that abnormal EEG activity would be found in the right cerebral hemisphere was not supported: All subjects in the NDE group had paroxysmal activity in the left hemisphere, and 1 had bilateral paroxysmal activity. The control subject's paroxysms arose solely from the right hemisphere. All of the paroxysmal EEG activity in the NDE group showed mid temporal spike activity (see Fig. 1 for examples), whereas the control subject showed an anterior temporal (F8) low-amplitude rhythmic transient. A between-groups difference in lateralized epileptiform activity was found (Fisher's Exact test, p=.051, two-tailed).
In addition to having a higher prevalence of epileptiform EEG than the control group, the NDE group reported significantly more temporal lobe symptoms (p<.005) and scored significantly higher on the CPES scale (p<.001; see Fig. 2). Temporal lobe symptoms include experiences that are common among temporal lobe epileptics, such as frequent anomalous experiences, sleepwalking, olfactory hypersensitivity, and hypergraphia. The CPES items refer specifically to the ictal experiences of temporal lobe epileptics (i.e., during seizures), or experiences that are evoked by direct electrical stimulation of the temporal lobe. These items cover a wide range of experiences, including feelings of intense personal significance and unusual olfactory, auditory, or visual perceptual experiences.
The NDE group exhibited different objectively measured sleep patterns during the PSG study than the control group. Analysis of total sleep time revealed that the NDE group slept about an hour less than the age- and gender-matched control group (355.6 min±85.3 vs. 404 min±63.3, p<.05). REM sleep latency was longer for the near-death experiencers than control subjects (109.1 min±53.0 vs. 77.3 min±27.9, p<.05), and the NDE group also had fewer REM sleep periods than control subjects (p<.05). No difference in the amount of REM sleep was found between groups, as measured by total minutes of REM sleep and REM sleep as a percentage of total sleep time.
To identify the predictors of the differences in REM sleep latency, we entered total sleep time (Step 1), DES score (Step 2), NDE Scale score (Step 3), Civilian Mississippi Scale for PTSD score (Step 4), temporal lobe symptoms (Step 5), and group (Step 6) into a hierarchical regression with REM latency as the dependent variable. Total sleep time accounted for 36.5% of the variance, p<.0005. Decreased total sleep time was related to delayed REM sleep onset. However, even after total sleep time was partialed out, NDE Scale scores were significantly associated with REM sleep latency, accounting for 12% of the variance, p<.05, so that the higher the score on this scale, the more delayed the REM sleep onset. The regression analysis indicates that REM sleep latency, although partially related to decreased sleep time, is related to NDE Scale scores, but unrelated to PTSD symptoms.
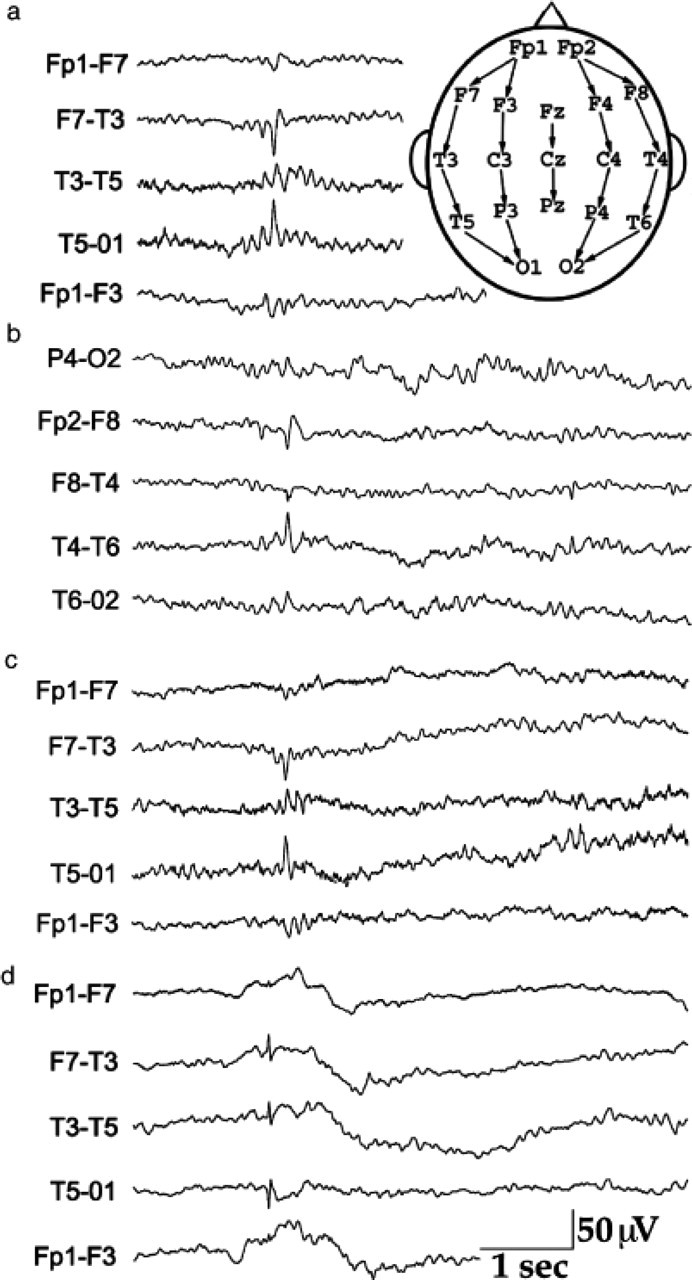
Examples of interictal epileptiform discharges in the temporal lobe of near-death experiencers in the current study. These examples come from Stage 2 (a–c) and REM (d) sleep. The illustration of the head shows the placement of the electrodes in the 10-20 system with an anterior-posterior bipolar reference scheme. Each tracing shows the localized brain activity from the area of the two electrodes indicated.
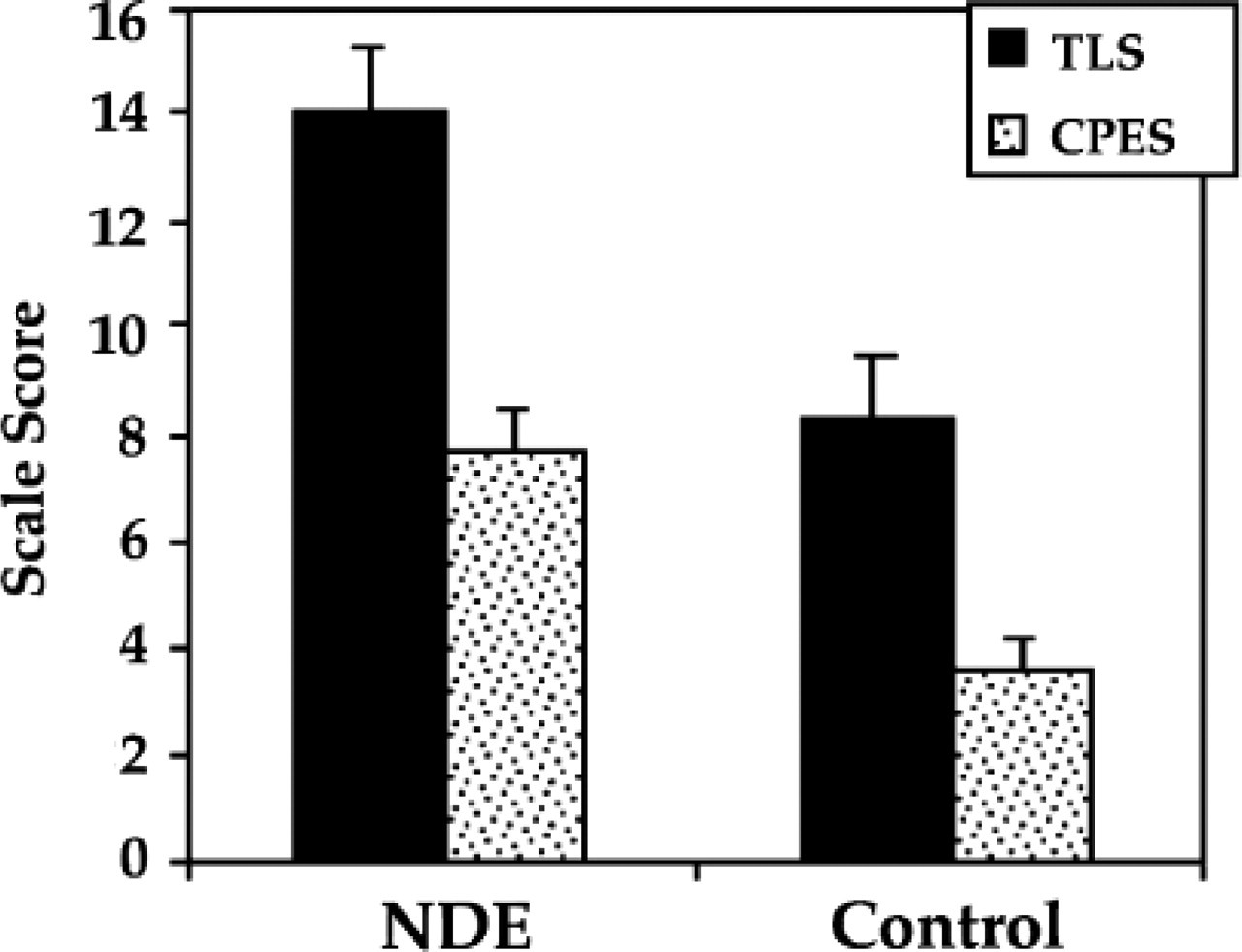
Scores on the Temporal Lobe Symptoms (TLS) and Complex Partial Epileptic Signs (CPES) subscales in near-death experiencers (NDE) and the control group.
Analysis of the COPE Inventory data showed significant differences between groups in positive coping (see Table 1), but not in measures of dysfunctional stress responses. The NDE group scored significantly higher than control subjects on measures of functional coping, such as active coping, planning, and positive reinterpretation and growth (p<.05). The NDE group also scored marginally higher on measures of religious coping (p<.10). No differences were found between groups on measures of maladaptive coping, such as denial, mental or behavioral disengagement, or substance abuse.
No significant differences were found between groups on any measure of PTSD, including the Mississippi Scale combined total or score on the Arousal subscale, Avoidance subscale, or Guilt subscale. Trauma survivors scored marginally higher than control subjects on the Intrusion subscale (p<.10).
The NDE group scored marginally higher than the control group on the combined total of the DES (see Fig. 3) and a number of subscales with items endorsed by clinical and nonclinical populations (p<.10). The NDE group scored significantly higher than the control group on the nonclinical Amnestic subscale, which includes items that are commonly endorsed by nonclinical populations (e.g., arriving at a destination and not remembering the drive). Near-death experiencers scored an average of 11 on the DES. In contrast, individuals with PTSD typically score above 30, and those with dissociative disorders, above 35 (Carlson & Putnam, 1993; Stewart & Bartucci, 1986). These findings indicate that although dissociation in the NDE group was elevated, it was within the normal range and did not approach pathological or clinically significant levels.
Because the NDE group was compared with nontrauma control subjects rather than non-NDE trauma survivors, the sleep and EEG differences in this study may represent a neurophysiological difference between traumatized and nontraumatized individuals rather than something unique to those who have had near-death experiences. Temporal lobe epilepsy is a common sequela of trauma (Stewart & Bartucci, 1986), especially if traumatic brain injury occurs (Annegers & Coan, 2000). If the temporal lobe epileptiform activity in the NDE sample is simply a result of generalized trauma, then epileptiform EEGs might be expected to be associated with trauma-related factors to a similar degree. However, in a simultaneous regression analysis, paroxysmal activity in the left temporal lobe was more highly related to NDE Scale scores than other trauma-related factors, such as PTSD, dissociation, or history of head trauma, and accounted for 18.2% of the variance of NDE Scale scores (β=.44, p<.05).
Summary of Self-Report Measures
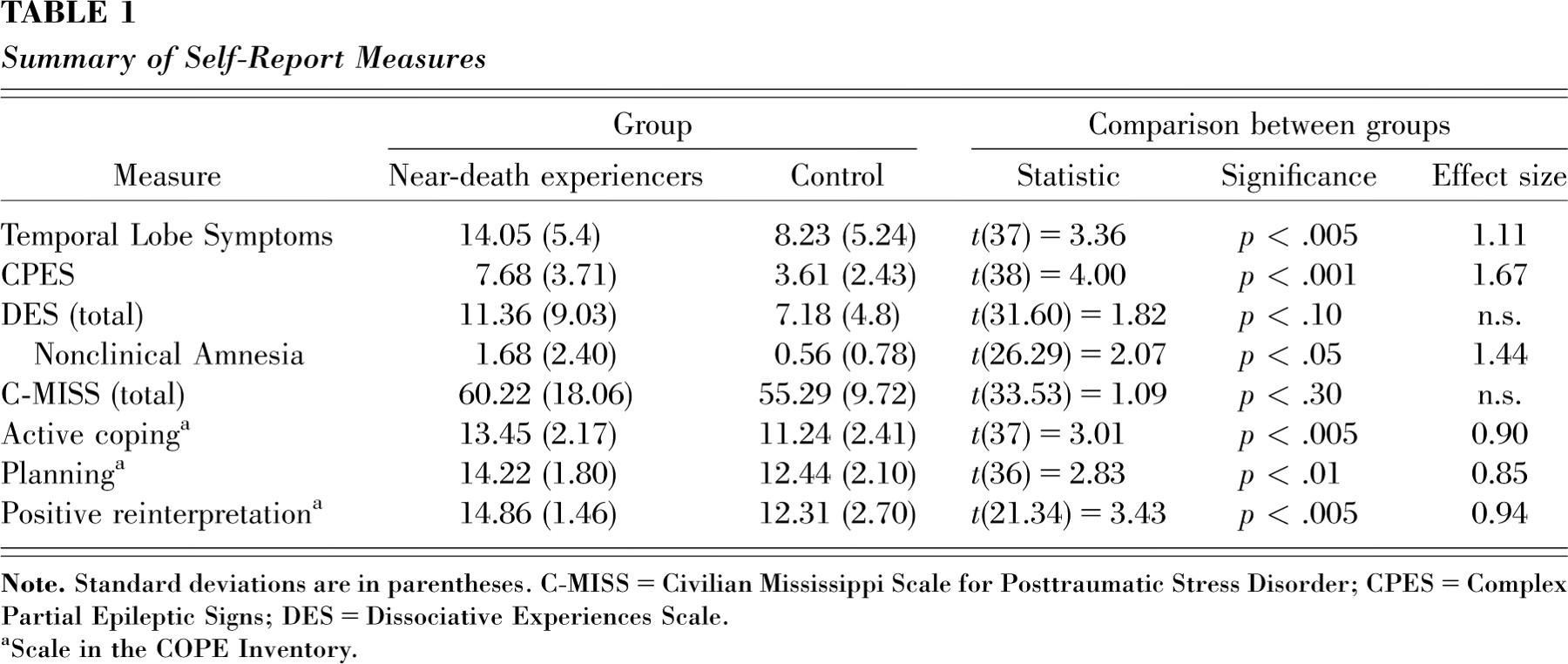
aScale in the COPE Inventory.
DISCUSSION
In this study, individuals who had had near-death experiences had a higher prevalence of interictal temporal lobe epileptiform EEG activity and reported more temporal lobe epileptic symptoms than nontraumatized control subjects. A few considerations suggest that the amount of epileptiform activity was probably underestimated, however. First, although sleep increases the likelihood of paroxysmal discharges, accuracy of prevalence estimates would be improved by multiple overnight studies (Salinsky, Kanter, & Dasheiff, 1987) and by using additional electrodes at nasopharyngeal or sphenoidal sites, especially if the epileptic focus is in the mesial basal temporal lobe (Sperling, Mendius, & Engel, 1986). Second, 25% of the trauma survivors with abnormal EEGs had paroxysmal activity during REM sleep. Usually, paroxysms are more frequent in non-REM sleep and occur in REM sleep only when the overall frequency of paroxysmal activity is high (Malow, Lin, Kushwaha, & Aldrich, 1998). In any case, the 22% incidence of epileptiform activity found in the current NDE sample exceeds the incidence rate found in normal, nonclinical populations (4 per 1,000) and in nonepileptic clinical populations (2–3%; Binnie & Stefan, 1999).
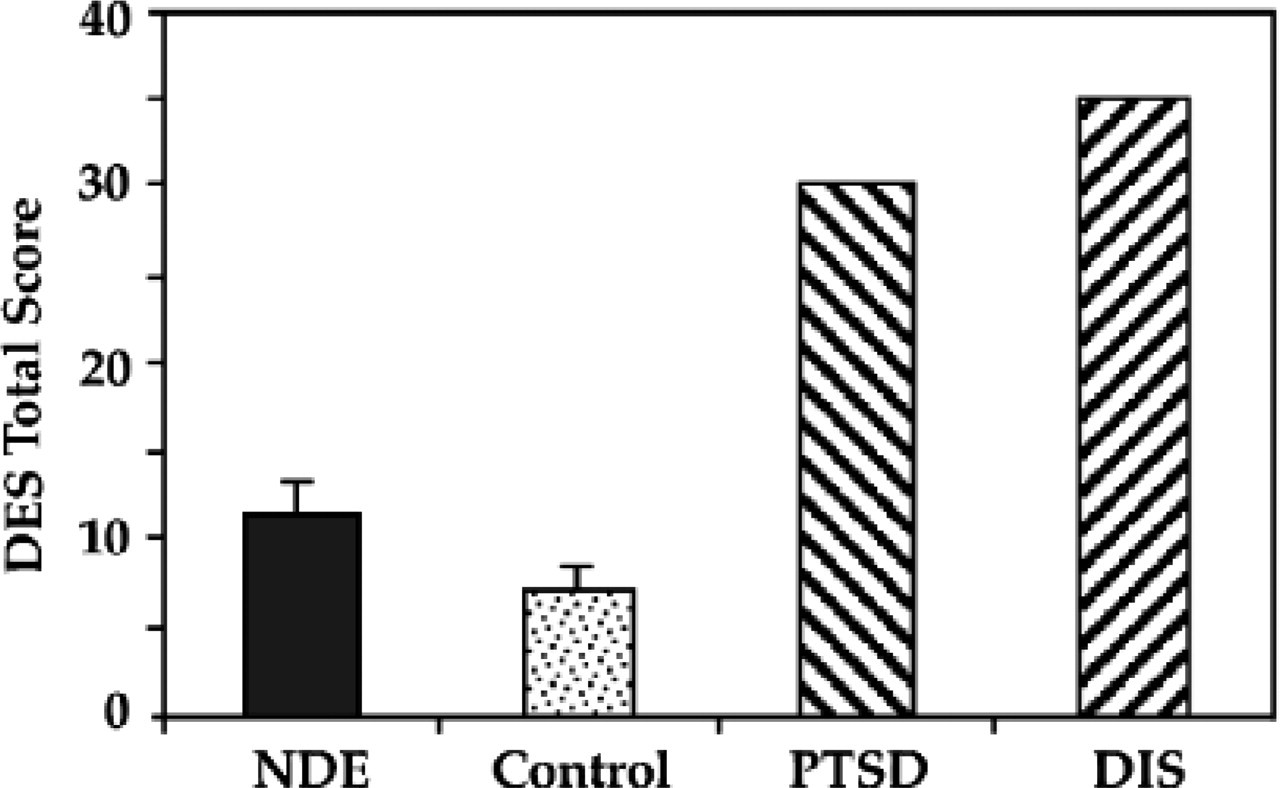
Self-reported dissociative experiences: average Dissociative Experiences Scale (DES) score for near-death experiencers (NDE) and control subjects in the present study, and for individuals with posttraumatic stress disorder (PTSD) and dissociative disorders (DIS) as described by Carlson and Putnam (1993).
The NDE group also showed differences from the nontraumatized control group in objectively measured sleep patterns, which suggests a psychophysiological difference. Alterations in REM sleep, in particular, may be related to differences in the regulation of affect. Previous studies have found decreased REM latencies and increased early REM in depressed individuals (Benca, Obermeyer, Thisted, & Gillin, 1992; Cartwright & Lloyd, 1994; Kupfer, 1976). The longer REM latency in the NDE sample contrasts with the shorter REM latencies seen in depression and may be associated with the atypical positive affect in response to acute stress. It is important to note that sleep data in both groups were collected without an adaptation night, and therefore the differences found may to some extent reflect differential responses to a novel sleeping environment.
It is possible that the temporal lobe and sleep findings in the NDE group are a generalized result of trauma rather than specific to the near-death experience itself. However, a number of factors indicate otherwise. First, both REM latency and epileptiform EEG were highly correlated with NDE Scale scores but unrelated to other trauma variables. Second, posttraumatic epilepsy has incidence rates from 1 to 5% in civilian populations (Jennet, 1975; Penfield & Shaver, 1945), with higher rates (18%) occurring only in cases of severe head trauma (Annegers & Coan, 2000). However, the majority of near-death experiencers in this sample (78%) did not sustain head trauma, and according to a regression analysis, the few cases of head trauma were not associated with epileptiform EEG activity. Therefore, the most appropriate comparison group are trauma survivors who experienced a loss of consciousness without head trauma. The incidence of epileptiform EEG in this trauma group has been found to be 5.7% (Shintani, Tsuruka, & Shiigai, 2001). Therefore, the incidence rate of epileptiform EEG found in near-death experiencers (22%) is higher than expected in an appropriate trauma comparison group. Furthermore, the complete left-sided lateralization of epileptiform discharges is atypical (Holmes, Dodrill, Kutsy, Ojemann, & Miller, 2001) and could represent a neurophysiological condition unique to this population. In contrast to what is found in typical trauma survivors, the physiological differences in near-death experiencers were not associated with negative stress reactions such as PTSD or dissociative disorders, but were associated instead with positive coping styles. Taken together, the temporal lobe, sleep, and psychological findings are not consistent with posttraumatic symptomatology. However, they may be indicative of a preexisting condition that predisposes individuals to unusual reactions to acute stress. These data are the first objective evidence of neurophysiological differences in near-death experiencers. Further research is needed to clarify the precise role of these differences in this unusual response to trauma.
Footnotes
Acknowledgments
We thank Keith Fridel, Ron Hutzler, and Kevin Martinez for their assistance in this research.