
Abstract
Chronic stress is typically associated with suppression of the immune system, including impaired responses to infectious disease and delayed wound healing. Recent work suggests that stress and depression can enhance production of proinflammatory cytokines, substances that regulate the body's immune response to infection and injury. We provide a broad framework relating stress and depression to a range of diseases whose onset and course may be influenced by proinflammatory cytokines, particularly the cytokine interleukin-6 (IL-6). IL-6 has been linked to a spectrum of chronic diseases associated with aging. Production of proinflammatory cytokines that influence these and other conditions can be directly stimulated by chronic stress and depression. We suggest that a key pathway through which chronic stress and depression influence health outcomes involves proinflammatory cytokines. We discuss the evidence for relationships between psychosocial factors and proinflammatory cytokines, and important health implications of these findings.
A long-standing idea in the field of psychoneuroimmunology (the study of interactions between the nervous system and the immune system) is that chronic stress suppresses the immune system. A recent review of the past 30 years of research on stress and immunity concluded that “the most chronic stressors were associated with the most global immunosuppression” (Segerstrom & Miller, 2004, p. 618). Our own research has previously demonstrated that immune suppression related to chronic stress has clinical implications, including impaired immune responses to infectious disease and delayed wound healing.
Currently, researchers are changing their thinking about the relations among chronic stress, depression, and immunity. Recent research suggests that chronic stress and depression may actually enhance certain immune responses. One immune response in question is inflammation, a broad term that refers to immune processes triggered by damage to cells and tissues. Such damage occurs in a variety of ways, including infection and injury. The immune system initiates inflammatory responses that are critical to resolving infections and repairing the damaged tissue.
Focusing on the inflammation-enhancing role of chronic stress and depression marks an important shift in how researchers conceptualize the complex interactions between the brain, behavior, and the immune system. Rather than supporting the model in which chronic stress and depression results in global immune suppression, the evidence reviewed here suggests a more complex and clinically relevant model in which chronic stress and depression result more generally in immune dysregulation. The body normally orchestrates a balanced response when faced with immunological challenges, but in the new model, chronic stress and depression disrupt this balance, suppressing some immune responses and enhancing others. This can have significant costs to an individual's physical health, including prolonged cell and tissue damage, increased vulnerability to acute and chronic diseases, and even premature aging.
CYTOKINES AND IMMUNE REGULATION
The key substances involved in regulating inflammatory responses to infection and injury are cytokines. Released by a variety of cells, cytokines are proteins that serve as intercellular signals regulating immune responses. Much like hormones of the endocrine system, cytokines transmit messages by interacting with receptors on cell surfaces and communicate over long distances in the body. Cytokines can be differentiated into two broad classes on the basis of their effects on the immune response: proinflammatory (promoting inflammation) and anti-inflammatory (restraining inflammation).
Proinflammatory cytokines, including interleukin-1 (IL-1), IL-6, and tumor necrosis factor-α (TNF-α), are produced by cells at the site of infection or injury (see Fig. 1). Subsequently, proinflammatory cytokines attract other immune cells to the affected site and prime them to activate and respond. Anti-inflammatory cytokines such as IL-4, IL-5, IL-10, and IL-13 dampen this immune response, inhibiting immune-cell activities, such as replication, activation, and synthesis of other cytokines.
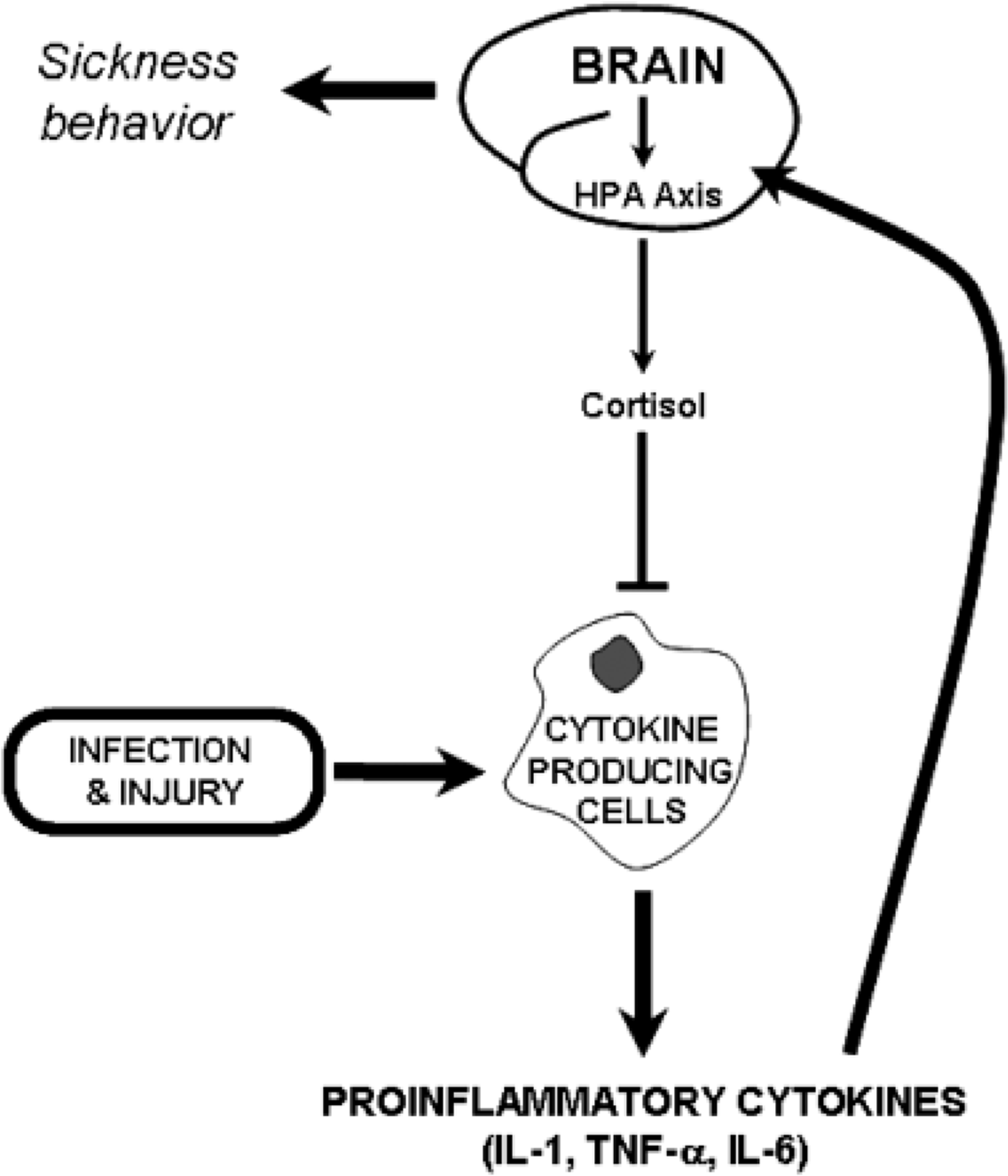
Proinflammatory cytokine responses to infection or injury under normal conditions. Lines terminating in arrowheads denote stimulatory pathways, and lines terminating in flat lines denote inhibitory pathways. Infection and injury stimulate cells to secrete proinflammatory cytokines, including interleukin-1 (IL-1), tumor necrosis factor-α (TNF-α), and IL-6. These cytokines attract other cells to the site and stimulate them to respond. In addition, proinflammatory cytokines travel to the brain and stimulate the hypothalamic-pituitary-adrenal (HPA) axis. This results in cortisol production, which helps to control inflammation and prevent the immune system from over-responding. Proinflammatory cytokines in the brain also induce sickness behavior, which helps the body maximize physical resources required to combat infection.
Proinflammatory cytokines initiate a variety of responses that regulate inflammation, in addition to stimulating production of other cytokines. Specifically, certain proinflammatory cytokines act on the brain, as shown in Figure 1, affecting the endocrine system and behavior. For instance, proinflammatory cytokines stimulate the hypothalamic-pituitary-adrenal (HPA) axis, a cascade of hormones from the hypothalamus and pituitary gland that results in production of the glucocorticoid hormone cortisol. Glucocorticoid hormones are steroid hormones produced by the adrenal cortex that can have anti-inflammatory effects by reducing the synthesis of proinflammatory cytokines, and thus complete a negative feedback loop that helps control inflammation. Proinflammatory cytokines also induce sickness behavior, a cluster of behaviors—including fever, decreased appetite, and reduced motor activity—that facilitate energy regulation (Maier & Watkins, 1998). By maximizing physical resources (energy, heat) required by the body to combat infection, sickness behavior is considered adaptive in helping the organism fight off infectious disease.
This review focuses on the proinflammatory cytokine IL-6, which has multiple effects on the immune, endocrine, and other tissue and organ systems, and thus serves as a good indicator of chronic inflammation. In addition, elevated IL-6 production is linked to key chronic diseases, such as cardiovascular disease and certain cancers, and to indices of physical health (Papanicolaou, Wilder, Manolagas, & Chrousos, 1998). Moreover, IL-6 production is related to psychosocial factors, including depression and chronic stress.
PSYCHOSOCIAL FACTORS AND PROINFLAMMATORY CYTOKINES
Several sociodemographic factors and health behaviors are related to elevated proinflammatory cytokines. Unlike other components of the immune system, which decline with age, IL-6 levels tend to increase with age (Papanicolaou et al., 1998). Men generally show higher levels of IL-6 than women, likely because of the effects of estrogen and androgens (Ershler & Keller, 2000). Higher IL-6 levels are associated with adverse health habits, including smoking, sedentary activity, and high body mass index; at the same time, elevated IL-6 levels are associated with higher rates of morbidity and mortality after controlling statistically for sociodemographic factors and health behaviors (Ferrucci et al., 1999).
As stated at the outset, the past 30 years of research on chronic stress and depression focused on immune suppression. Accordingly, one might expect that chronic stress and depression are related to suppressed production of proinflammatory cytokines. However, empirical evidence strongly suggests that major depression, depressive symptoms, and chronic stress enhance production of proinflammatory cytokines.
Major depression is related to enhanced proinflammatory cytokine levels, including IL-6, which can be reduced following successful treatment with antidepressant medications (Kenis & Maes, 2002). Elevated depressive symptoms also are related to elevated proinflammatory cytokine levels (e.g., Miller, Stetler, Carney, Freedland, & Banks, 2002). We recently found that higher levels of depressive symptoms were related to higher levels of IL-6 among older adults (Glaser, Robles, Sheridan, Malarkey, & Kiecolt-Glaser, 2003). More important, individuals reporting more depressive symptoms showed increased IL-6 levels 2 weeks after receiving a challenge to the immune system through an influenza virus vaccination, whereas there was little change in IL-6 among individuals reporting few or no depressive symptoms, as shown in Figure 2. In general, depressive symptoms were quite low in our sample of older adults, which suggests that even modest depressive symptoms may be sufficient in making the immune system hypersensitive to immunological challenges, resulting in amplified IL-6 production. Sensitization of inflammatory responses may have important health consequences, as amplified and prolonged inflammatory responses following infection and other immunological challenges could accelerate the progression of a range of age-related diseases. Overall, these data suggest that proinflammatory cytokines are a key mechanism whereby major depression and depressive symptoms may serve as a gateway to a broad array of health problems.
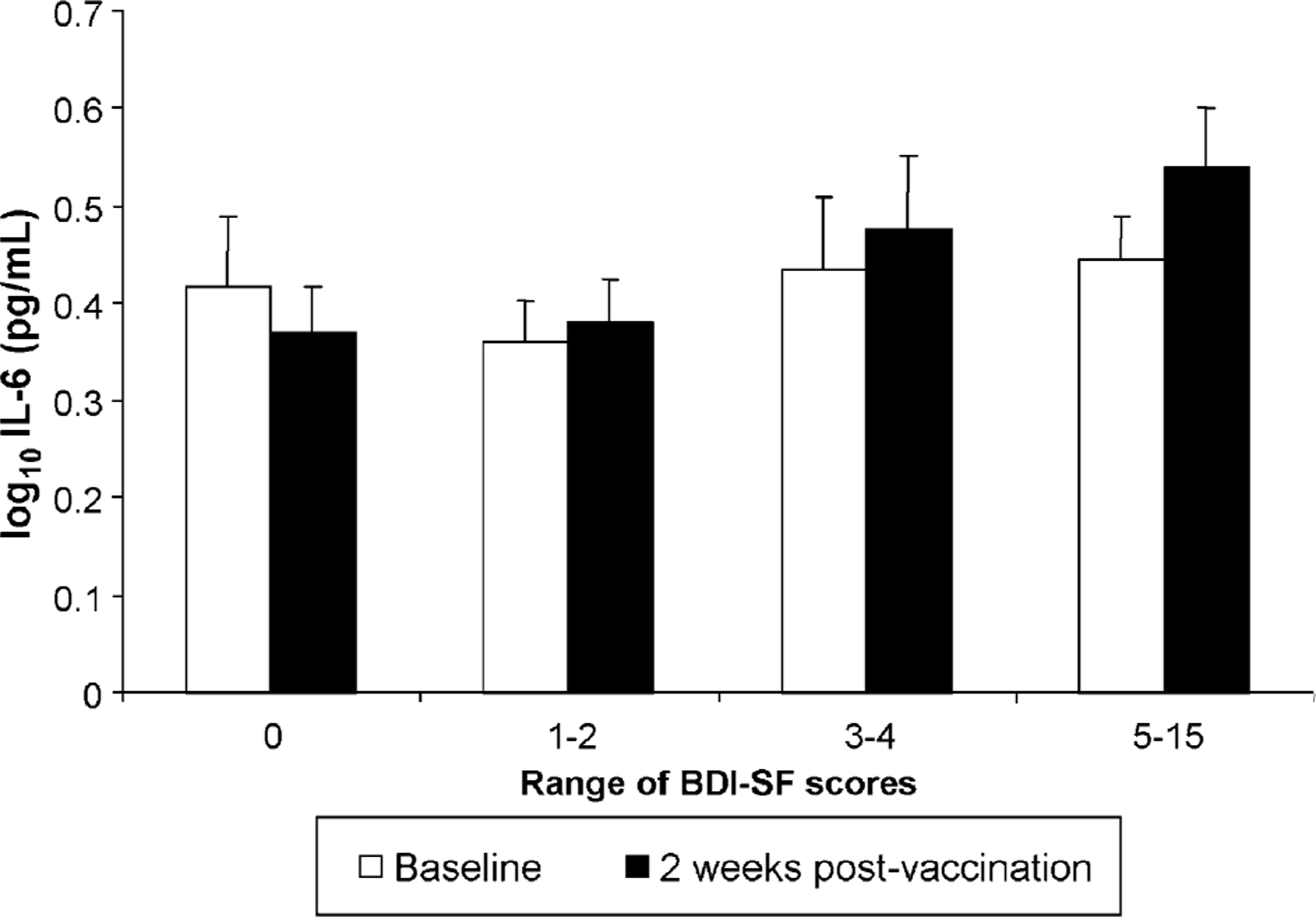
Levels of interleukin-6 (IL-6) as a function of depressive symptoms in a sample of 119 older adults. IL-6 levels were measured before participants received an influenza virus vaccination (baseline, represented by the white bars) and 2 weeks after they were vaccinated (dark bars). Depression symptoms were measured using the short form of the Beck Depression Inventory (BDI-SF). Individuals reporting depressive symptoms showed an increase in IL-6 2 weeks following vaccination compared to individuals reporting few or no depressive symptoms. Error bars denote standard error of the mean. Redrawn after Glaser, R., Robles, T.F., Sheridan, J., Malarkey, W.B., & Kiecolt-Glaser, J.K. (2003).
Chronic stressors are also related to elevated production of IL-6. A study found that women who were caring for a relative with Alzheimer's disease had higher levels of IL-6 than either women who were anticipating a housing relocation or women from the same community who experienced neither of these stressors (Lutgendorf et al., 1999). This finding was particularly noteworthy because the caregivers were 6 to 9 years younger, on average, than women in the other two groups. Given that IL-6 levels generally increase with age, what might be the impact of chronic stress on age-related increases in IL-6?
We addressed this question by following older adults undergoing a chronic stressor for 6 years and assessing age-related change in their IL-6 levels during that period (Kiecolt-Glaser et al., 2003). Older adults experiencing the chronic stress of caring for a spouse with Alzheimer's disease showed an average rate of annual IL-6 increase that was about 4 times as large as that of noncaregivers. There were no systematic group differences in chronic health problems, medications, or health-relevant behaviors that might have accounted for the faster increase in IL-6 in caregivers. Moreover, the mean annual changes in IL-6 among former caregivers did not differ from that of current caregivers even several years after the death of the impaired spouse. Based on these findings, we suggest that chronic stressors may be capable of substantially augmenting normal age-related increases in proinflammatory cytokine production. Put simply, chronic stress may contribute to premature aging of the immune system.
PSYCHOSOCIAL FACTORS AND MECHANISTIC PATHWAYS
Apart from influencing health-related behaviors, how might psychosocial factors contribute to elevated production of proinflammatory cytokines? Figure 3 depicts four potential pathways. Several pathways (i.e., A, C, and D) involve dysregulation of signals coming from the endocrine system, specifically the HPA axis. Stress-related HPA activity results in elevated levels of glucocorticoid hormones, including cortisol. As previously mentioned, glucocorticoid hormones reduce the synthesis of proinflammatory cytokines and thereby help prevent the immune system from overshooting, or mounting an overreactive immune response that could cause damage to cells and tissues, such as the damage observed in autoimmune diseases like multiple sclerosis or rheumatoid arthritis.
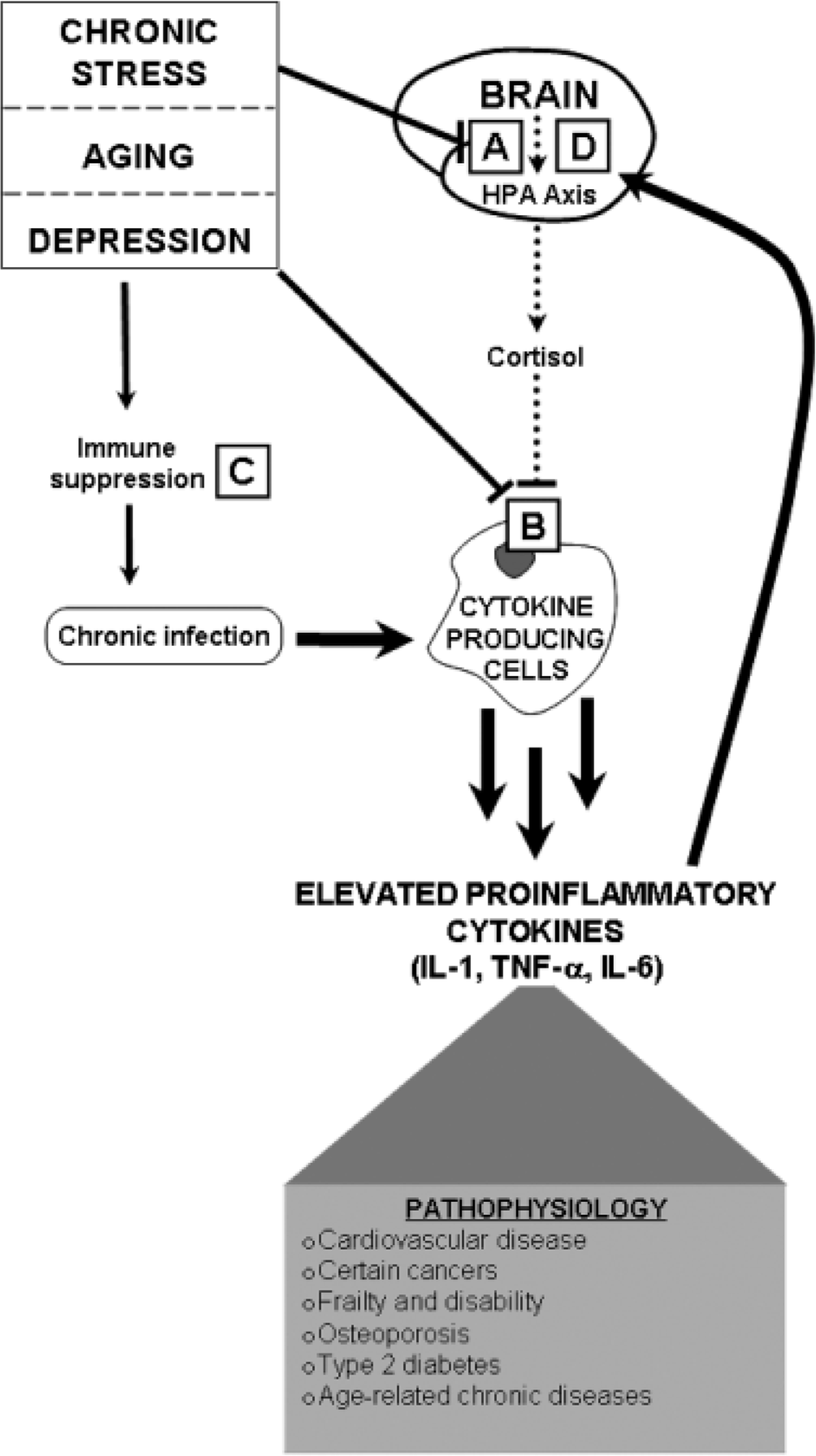
A theoretical model depicting how psychosocial factors and aging contribute to immune dysregulation. Lines terminating in arrowheads denote stimulatory pathways, and lines terminating in flat lines denote inhibitory pathways. Dotted lines denote disrupted signaling pathways. In this model, chronic stress, depression, and aging contribute to elevated proinflammatory cytokines—interleukin-1 (IL-1), tumor necrosis factor-α (TNF-α), and IL-6—in four ways: (A) Psychosocial factors may disrupt the functioning of glucocorticoid hormones (such as cortisol) in the brain by reducing the number of glucocorticoid receptors in certain brain regions or disrupting receptor functioning, which may result in dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis; (B) psychosocial factors may disrupt the functioning of glucocorticoid receptors on cytokine-producing cells, rendering those cells less sensitive to the anti-inflammatory effects of cortisol; (C) psychosocial factors may result in immune suppression, which inhibits the body's ability to fight off infection and injury, leading to chronic infections; and (D) proinflammatory cytokines may reduce the number of glucocorticoid receptors in the brain or disrupt the functioning of those receptors. All four mechanisms may eventually lead to elevated production of proinflammatory cytokines and, over time, contribute to chronic disease and pathophysiology.
If glucocorticoid signals are disrupted, the result may be reduced restraint on the immune system and overproduction of proinflammatory cytokines. Figure 3, Path A depicts that chronic stressors and depression disrupt glucocorticoid signaling in the brain by altering the function of glucocorticoid receptors (Raison & Miller, 2003). Figure 3, Path B depicts that chronic stressors and depression may decrease the responsiveness of target tissues to cortisol. For instance, chronic stress is related to decreased sensitivity of immune cells to the anti-inflammatory effects of glucocorticoids (e.g., Miller, Cohen, & Ritchey, 2002).
Another pathway through which psychosocial factors may contribute to enhanced production of proinflammatory cytokines involves stress-related immune suppression (Fig. 3, Path C). Chronic stress impedes the immune response to infection, increasing risks for catching contagious diseases and having prolonged illness episodes, delaying wound healing, and increasing the risk for wound infection after injury. Thus, immune suppression may contribute to repeated, chronic, or slow-resolving infections or wounds, which subsequently enhance secretion of proinflammatory cytokines, a process that can serve to further inhibit certain aspects of immune responses. Finally, elevated proinflammatory cytokines may themselves impair cortisol signaling, and thus HPA axis regulation, by altering the functioning of glucocorticoid receptors in the brain (Fig. 3, Path D). As a result, elevated proinflammatory cytokines impair the ability of the HPA axis to regulate inflammatory processes, further enhancing proinflammatory cytokine production.
HEALTH IMPLICATIONS
Under normal conditions, elevated levels of proinflammatory cytokines are critical to resolving damage from infection and injury. However, chronic infections can result in persistent stimulation of immune and proinflammatory cytokine responses, leading to pathological effects (Hamerman, Berman, Albers, Brown, & Silver, 1999). For example, low levels of persistent inflammation may result when chronic infections such as periodontal disease, urinary tract infections, chronic pulmonary disease, and chronic renal disease continuously stimulate the immune system. In turn, chronic elevations in proinflammatory cytokines including IL-6 have substantially deleterious health implications, including links to a spectrum of conditions associated with aging. These conditions include cardiovascular disease, osteoporosis, arthritis, type 2 diabetes, certain cancers (including multiple myeloma, non-Hodgkin's lymphoma, and chronic lymphocytic leukemia), Alzheimer's disease, and periodontal disease (Ershler & Keller, 2000).
The association between cardiovascular disease and IL-6 has received increased attention in the past decade, in part because of the central role that IL-6 plays in promoting the production of C-reactive protein (CRP), recently recognized as an important risk factor for myocardial infarction (Papanicolaou et al., 1998). Elevations in both IL-6 and CRP levels are related to risk of future cardiovascular disease, myocardial infarction, and mortality, even in apparently healthy adults (Taubes, 2002).
More globally, chronic elevations in proinflammatory cytokines may be one key biological mechanism that fuels declines in physical function leading to frailty, disability, and, ultimately, death. Indeed, statistical analyses show that even after controlling for risk factors such as cholesterol levels, hypertension, and obesity, chronic IL-6 production continues to be an important indicator of physical decline among the very old (Ferrucci et al., 1999).
For these reasons, the role of chronic stress and depression in promoting IL-6 production should also have clinical relevance. Moreover, stress-related increases in proinflammatory cytokines may be particularly harmful for older adults. For instance, in our study of chronic-stress-related increases in IL-6, the average caregiver reached IL-6 levels that doubled his or her mortality risk by the age of 75; the average control participant in the study did not reach similar levels until the age of 90 (Kiecolt-Glaser et al., 2003).
CONCLUSION
Research has identified a key mechanism whereby chronic stress and depression may promote the development of chronic disease and speed aging of the immune system: elevated proinflammatory cytokine levels. This work demonstrates the shift in the field of psychoneuroimmunology away from focusing solely on chronic stress and immune suppression, toward integrating chronic stress and immune dysregulation in a model that emphasizes the balance between two important and adaptive mechanisms: inflammatory and anti-inflammatory responses.
Depression and chronic stress, by disrupting bidirectional communication between the brain and immune system, effectively damages the “brakes” that help restrain inflammatory responses, paving the way for increased production of proinflammatory cytokines through several distinct mechanisms. Depressive symptoms may increase production of proinflammatory cytokines following an infection or injury. Furthermore, chronic stress and depression accelerate age-related increases in production of proinflammatory cytokines, making these psychosocial stressors uniquely problematic for older adults.
Current work continues to establish relationships among chronic stress, depression, and proinflammatory cytokines. Future research must firmly establish proinflammatory cytokines as a key mediator between psychosocial factors and chronic disease. This requires longitudinal follow-up studies that not only track chronic stress, depression, and inflammation over time, but also include assessments of clinical indicators of chronic disease, such as coronary artery calcification in atherosclerosis. Ultimately, intervention studies will be needed to determine if treating chronic stress and depression can eventually restore immunological balance and affect health.
Footnotes
Acknowledgements
Work on this article was supported by National Institutes of Health Grants P50 DE13749, P01 AG16321, AT002122, M01 RR034, and CA16058, and by a National Science Foundation Graduate Research Fellowship to the first author.