
Abstract
The belief that people are in control of desired outcomes, including those associated with aging, is a hallmark of American culture. Nevertheless, older adults are less likely than the young to believe there are things that can be done to control aging-related declines in areas such as memory. Within age groups, individual differences in control beliefs are related to cognitive performance, health, and well-being. Mechanisms linking perceived control and positive outcomes include adaptive behaviors such as strategy use and physical activity. There is some evidence that control beliefs can be modified in later life, as illustrated in an intervention for fear of falling. Further work is needed to examine the antecedents of perceived control in later life and the implications of control beliefs in other aging-related domains.
More so than citizens of any other country, Americans believe that they are in control of outcomes in their lives. A 2002 Pew Center poll of 38,000 people in 44 countries presented a typical control-belief item: “Success in life is pretty much determined by forces outside our control” (Leland, 2004). In the United States, about 65% disagreed with the statement, as did 60% in Canada. In other countries, disagreement ranged from about 10% (Bangladesh) to 50% (Japan).
A majority of Americans believe they have control over many aspects of life, and aging is one such aspect. A survey conducted by Parade magazine and Research America (2006) asked, “Do you think there is anything you can do to stay healthy as you grow older, or do you think the way you age is basically outside your control?” The results revealed that 84% of Americans believe there are things they can do to control the aging process. The $40 billion-a-year anti-aging industry, which offers products and treatments designed to prevent, slow, reverse, or compensate for aging-related changes in the face, body, and mind, depends on this prevalent belief that there are things we can do to take control of aging-related changes.
Control over the aging process is heralded not only in popular culture but also in professional journals and books such as Successful Aging by Rowe and Kahn (1998). A key message conveyed is that although aging is influenced to some degree by genetic factors, there is a large component that is determined by lifestyle choices and behavioral factors—that is, the nature of aging is to some extent under one's own control.
AGE DIFFERENCES IN CONTROL BELIEFS
Although there is a widespread belief that we can control aspects of aging, there is also strong evidence, based on both cross-sectional and longitudinal studies, that the sense of control decreases, on average, with age (Krause & Shaw, 2003; Lachman & Firth, 2004; Mirowsky, 1995). In the 1995 John D. and Catherine T. MacArthur Foundation National Survey of Midlife in the United States (MIDUS), we administered an item similar to the one in the Pew Center Poll to a national probability sample of 4,242 Americans, aged 25 to 75 (Lachman & Firth, 2004). Respondents were asked to agree or disagree with the statement, “What happens in my life is often beyond my control.” Overall, we found results similar to the Pew results in that 70% disagreed with this statement. We also examined demographic factors (age, sex, education, income, religion, race, marital status) in relation to agreement or disagreement with this control item, and we found the largest variations by age. Almost 80% of the young (ages 25–39) said they are in control (i.e., disagreed with the statement), whereas it was 71% for the middle aged (40–59), and only 62% for the older adults (60–75). These age-group differences were not due to group variations in education, income, or health, although control beliefs were also related to socioeconomic status and health (Lachman & Firth, 2004).
Those who score higher in sense of control strongly believe there are things they can do to bring about desired outcomes. The primary focus of our research program is on perceptions of control especially in relation to declines associated with aging, including beliefs about prevention, remediation, and compensation. These expectancies for control, or lack thereof, have implications for affect and action whether or not they are veridical (Thompson, 1999).
Older adults seem to maintain their overall sense of mastery (beliefs about one's ability or self-efficacy), perhaps because they adjust the salient domains or the standards that they use to define their competence. With aging, we see mainly a loss of control associated with an increasing acknowledgment of the constraints and limitations due to uncontrollable factors or to reduced contingency between actions and outcomes (Lachman & Firth, 2004).
CONTROL AND WELL-BEING IN LATER LIFE
Although a majority in the United States may believe that the decrements associated with aging are preventable or modifiable, there are many, especially in later life, who believe declines are largely inevitable or irreversible. There is a great deal of evidence that such individual differences in control beliefs are associated with key aging outcomes (Rowe & Kahn, 1998). It is consistently found that a high sense of control is associated with being happy, healthy, wealthy, and wise. In the MIDUS sample, those with a higher sense of control had greater life satisfaction and a more optimistic view of adulthood; they reported that things were going well and expected them to either stay that way or even to get better in the future (see Lachman & Firth, 2004). We also have found that those with higher control are less depressed and have better self-rated health, fewer chronic conditions, and less-severe functional limitations.
Control beliefs moderate the well-known relationship between socioeconomic status (SES) and health. Those with lower incomes typically have a lower sense of control and poorer health. This likely reflects, at least in part, the reality of conditions tied to economic circumstances. Differences by countries in control beliefs such as those found in the Pew Center study cited above may mirror economic circumstances and public health conditions, or religious and cultural ideologies. In the United States, we found that although, on average, lower-income groups reported less control, there were individual differences within groups and the distribution of control beliefs overlapped across SES groups. Those with lower incomes who managed to develop and maintain a high sense of control had health similar to that of the higher-income groups (Lachman & Weaver, 1998). Thus, control beliefs buffer the negative health consequences of lower SES.
In the cognitive domain, the sense of control is tied to better memory and greater intellectual functioning, especially among older adults. Although much of the work has been cross-sectional and correlational, there is longitudinal evidence that those who have higher control beliefs improve more on cognitive tests with practice and also are less likely to show aging-related declines in cognitive functioning over time (Caplan & Schooler, 2003).
HOW ARE CONTROL BELIEFS ADAPTIVE?
Although relationships between control beliefs and positive outcomes such as good memory, health, and well-being are fairly well established, there is little work examining the processes linking control beliefs with outcomes in these domains. To guide our work, we have used a conceptual model of the role of adaptive beliefs (e.g., control) and behaviors (e.g., strategy use, physical activity) in relation to aging-related changes, derived from cognitive-behavioral theory (Bandura, 1997). This model (see Fig. 1) shows a multidirectional process in which control beliefs are influenced by prior performance outcomes and beliefs about control also have an influence on subsequent performance and outcomes through their impact on behavior, motivation, and affect. For example, older adults who experience memory lapses or declines in physical strength may respond with a lowered sense of control in these domains, especially if these changes are attributed to uncontrollable factors. Such beliefs in low control can be detrimental if they are associated with distress, anxiety, inactivity, and giving up without expending the effort or using the strategies needed to support optimal outcomes.
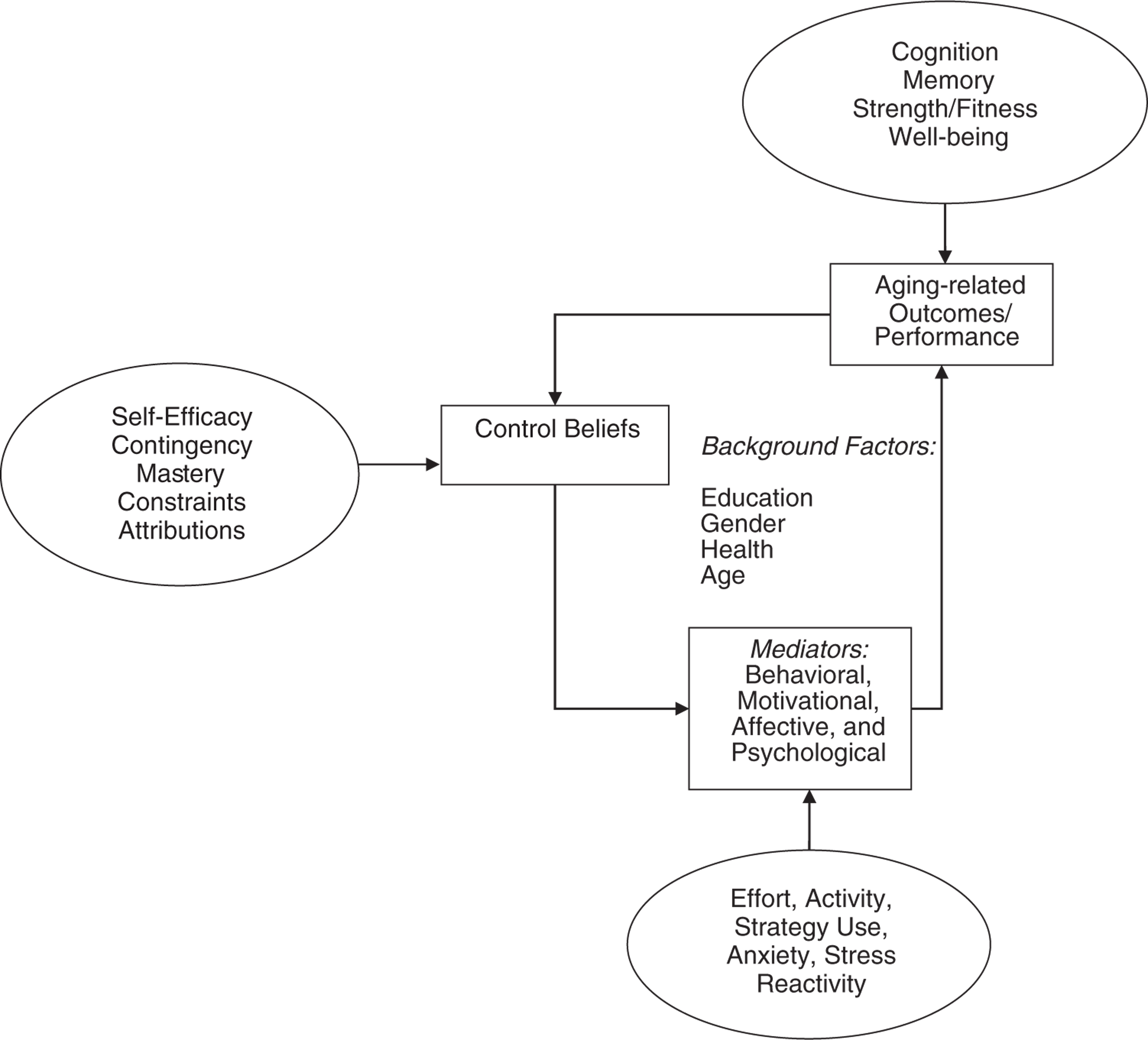
Conceptual model of the relationship between control beliefs and aging-related performance outcomes with postulated mediators, based on cognitive-behavioral theory.
We have examined possible affective, behavioral, motivational, and physiological mechanisms, including anxiety, effort, compensatory strategies, and physical activity, that link control beliefs and outcomes. In the health domain, for example, we found that those who have a higher sense of control are more likely to exercise regularly and also to have better health (Lachman & Firth, 2004).
We also have investigated mechanisms linking control beliefs to memory, a domain that typically shows age-related declines. In a study of 335 adults aged 20 to 85, we asked participants to recall a list of 30 categorizable words such as types of fruit and flowers (Lachman & Andreoletti, 2006). We found that control beliefs were positively related to effective strategy use and to recall performance for middle-aged and older adults, but not for young adults. These age differences in the pattern of correlations for beliefs with effective strategy use and memory are shown in Figure 2. Moreover, the relationship between control beliefs and recall was mediated by strategy use for the middle aged and partially mediated for older adults. Those who had a higher sense of control were more likely to use an effective strategy, in this case categorizing the words, and they in turn had better recall. Although the directional relationship can not be confirmed given the correlational design, we tested alternative directional models and this mediational model provided the best fit.
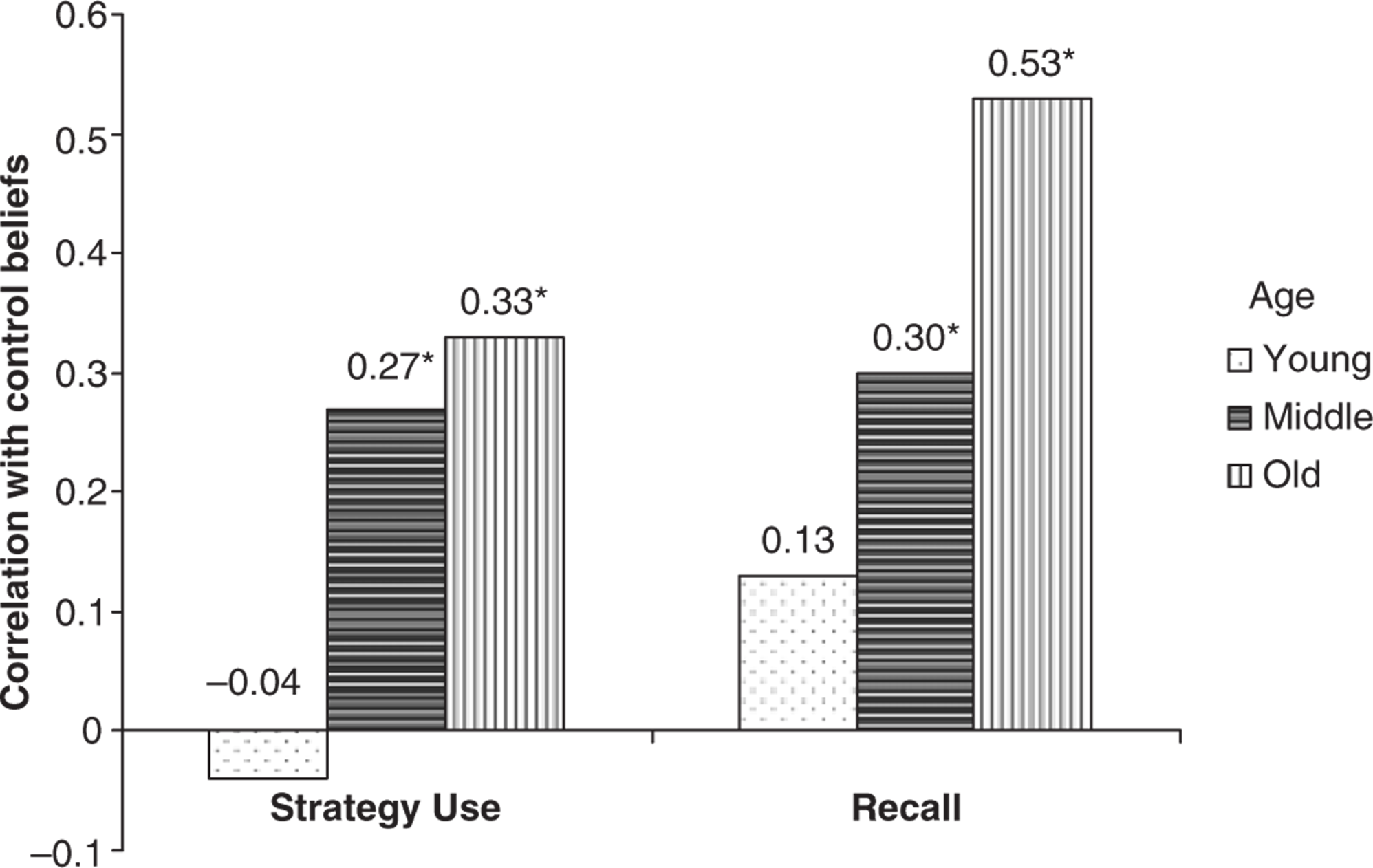
Age differences in correlations between control beliefs, strategy use, and recall, based on data from Lachman & Andreoletti (2006).
CONTROL INTERVENTIONS
Given the apparent benefits of control beliefs and the likelihood of declines in sense of control in later life, we were interested in whether we could modify control beliefs among older adults and if this would affect outcomes in a given domain. Many older adults assume they are too old to improve performance or functioning or to make up for losses in areas such as memory or physical ability. Using the model in Figure 1 as a guide, we have conducted interventions that all have in common a joint focus on modifying control beliefs and behaviors (Lachman, 2000). We assumed that enduring behavior change is unlikely without first instilling confidence that aging-related declines can be controlled.
A fear of falling is relatively common among older adults. This is typically manifested as a low sense of efficacy for engaging in activities without falling and a sense that falling is uncontrollable (Tennstedt et al., 1998). Consistent with our cognitive-behavioral conceptual model, the best predictor of self-efficacy and control with respect to falling is previous fall status, and low falls self-efficacy is subsequently associated with maladaptive behavioral changes such as activity restriction, which can lead to increased risk of falling through muscle atrophy and deconditioning.
Our multifaceted intervention targeted beliefs about control over falls with 434 older adults who reported fear of falling and were randomly assigned to an intervention or a contact control condition (Tennstedt et al., 1998). We used cognitive-restructuring strategies to reframe control beliefs. This entailed analysis and challenge of maladaptive beliefs (e.g., I can't do this; I am too old; it won't do any good; I will get hurt) and information that efforts (e.g., using fall-prevention strategies; engaging in strength and balance exercises, which were also taught to participants) can make a difference for outcomes. The contact control group was given information about risk factors for falls and saw a video about ways to minimize the risk of falls. Those who completed the treatment increased their falls self-efficacy, sense of control over falls, level of intended activity, and physical mobility functioning significantly more than the control group did. Although the fear-of-falling intervention did not target falls reduction directly, greater mobility and increased activity should lead to a decrease in falls due to better physical conditioning. However, if intervention participants increased their activity levels as indicated by their intentions, they might also have inadvertently increased their risk of falls due to greater exposure. There were no significant differences between intervention and control subjects in the number of falls for up to 12 months (Tennstedt et al., 1998), which suggests, at least, that the intervention did not have unintended side effects.
IS A SENSE OF CONTROL ALWAYS ADAPTIVE?
Most of the work exploring a sense of control in relation to age-related well-being has focused on types of performance and situations that are to some extent controllable. There is some evidence that in uncontrollable situations, those with lower control beliefs do better, at least over the short run. For example, Bisconti, Bergeman, and Boker (2006) found recent widows with greater levels of perceived control over their social support had poorer overall adjustment across the first 4 months of widowhood. Longitudinal studies over longer periods are needed to investigate whether a high sense of control may be more beneficial for resilience and coping over the long run. Those who have a strong sense of control would be expected to be better at finding ways to cope with uncontrollable events or unattainable goals or outcomes by using secondary (change the self) rather than primary (change the situation) control strategies (Wrosch, Heckhausen, & Lachman, 2006).
CONCLUSIONS AND FUTURE DIRECTIONS
Adults with a low sense of control over aging-related declines may be vulnerable to memory problems and physical disabilities in later life, in part, because they are not likely to use compensatory strategies or adopt preventative or remedial behaviors. There is the potential to reduce declines in cognition and physical functioning by instilling more adaptive beliefs about controllability over aspects of the aging process in conjunction with training in adaptive behaviors.
Although to some extent people may be able to prevent, postpone, or compensate for aging-related declines, it is rare to be able to influence diseases, illnesses, injuries, loss of loved ones, and ultimately when and how one's own aging process comes to an end. Thus, to some extent a belief in control over aging has an illusory quality (Thompson, 1999). Nevertheless, for domains in which efforts do make a difference, there is consistent evidence that those who believe they can control aging-related outcomes do better.
We found some evidence for the mediational role of strategy use and activity, and we are currently exploring anxiety and stress reactivity as potential mediators of the relationship between control beliefs and memory. With regard to areas with aging-related declines, we find that control beliefs make more of a difference for middle-aged and older adults even though on average their control beliefs are lower (Lachman & Andreoletti, 2006). More work is needed to examine whether control beliefs play similar roles for change outcomes at younger ages and in other domains as well as in other cultures. We have focused mainly on the domains of memory and physical health, and we are now looking at control in relation to hearing loss.
Previous research has looked primarily at the consequences of control beliefs. In future work we will explore the sources of control beliefs and address issues of causal direction. We have just completed collecting 10-year longitudinal data with the MIDUS sample, which will enable us to examine biopsychosocial antecedents of changes in control beliefs. We will examine the impact of changes in health and disability and identify those who are most vulnerable to losses in the sense of control.
Footnotes
Acknowledgements
This article is dedicated to Paul B. Baltes, my extraordinary mentor and wonderful friend, who passed away on November 7, 2006. I would like to express my appreciation for financial support for this research from the John D. and Catherine T. MacArthur Foundation Research Network on Successful Midlife Development and the National Institute on Aging: Grants R01 AG 17920, AG11669, and PO1 AG 20166. In addition, I would like to acknowledge the many contributions from my collaborators: Carrie Andreoletti, Kimberly Firth, Jonathan Howland, Alan Jette, Shevaun Neupert, Ann Pearman, Ron Spiro, Sharon Tennstedt, Suzanne Weaver, and Stacey Whitbourne.