
Abstract
Whether or not an individual develops dementia is powerfully influenced by genes. For Alzheimer's disease, the most common type of dementia, one susceptibility gene with major effects has been identified, but progress finding other susceptibility genes has stalled. Twin studies have revealed that nongenetic risk also plays an important role, as there are many monozygotic twin pairs in which only one individual has dementia. Scientists have argued that gene-by-environment interactions will be key to understanding vulnerability to Alzheimer's disease; but to date, few substantial gene-by-environment interactions have been replicated. Often, too, the nongenetic or lifestyle factor appears to have a protective effect only for those individuals not carrying the risky version of the gene, not for those individuals who are at genetic risk.
Whether one's future includes dementia is a concern for many middle-aged adults and, now, aging Baby Boomers. Ordinary memory lapses have assumed the status of “senior moments.” People play Sudoku as a form of mental exercise in the hopes that it will stave off decline. Jokes about memory are traded by e-mail:
Two elderly couples were enjoying friendly conversation when one of the men asked the other, “Fred, how was the memory clinic you went to last month?”
“Outstanding,” Fred replied. “They taught us all the latest psychological techniques: visualization, association, etc. It was great.”
“Sounds terrific! What was the name of the clinic?”
Fred went blank. He thought and thought, but couldn't remember.
Then a smile broke across his face and he asked, “What do you call that flower with the long stem and thorns?”
“You mean a rose?”
“Yes, that's it!”
He turned to his wife, “Rose, what was the name of that memory clinic?” (Helpguide, 2005)
A recent survey conducted by Harris Interactive for MetLife Foundation found that, among Americans aged 55 and older, Alzheimer's disease (AD) was the most feared on a list of diseases (chosen by 31% of respondents, compared to 27% choosing cancer and 20% choosing stroke; Harris Interactive, 2006). Fear for one's own cognitive future is especially strong among those who watch their own parents develop dementia.
Such a fear is not entirely misplaced. Among 65-year-olds, lifetime risk of developing any dementia has been estimated to be 11% for men and 19% for women (Seshadri et al., 1997). Rates of dementia increase exponentially with age. The consensus among expert scholars is that 30% of North Americans aged 85 and older are living with dementia (Ferri et al., 2005). Prevalence rates generally appear to be higher for African Americans than for Whites.
A number of investigators have addressed risk of AD in first-degree relatives of AD patients, with estimates ranging from 24% to 49%. In other words, lifetime risk of developing AD is 1.8 to 4.0 times higher for those with a family history of the disorder than for those without. Proportional increase in risk associated with being a first-degree relative of an AD patient is similar for African Americans and for Whites (Green et al., 2002). At the same time, only a quarter of those with late-onset AD have had a close relative with dementia (Bird, 2005).
TYPES OF DEMENTIA
Dementia refers to a group of diseases that have their onset in old age and in which there is progressive loss of cognitive functioning that eventually affects all aspects of self-care. Few dementias are reversible, although treatable factors that might contribute to cognitive decrements—for example, vitamin B12 deficiency, hypothyroidism, depression, or dehydration accompanying acute illnesses such as influenza—are important to assess and address.
The most common type of dementia is AD, accounting for up to two thirds of all cases of dementia. The cause of AD is not established, although how it originates can be described. A key feature is the formation in the brain of deposits of a protein called beta-amyloid (Aβ); these deposits are called amyloid plaques. It is hypothesized that these plaques cause oxidative injury (damage due to release of free radicals during cellular metabolism), inflammation, and alterations in neurotransmitters, eventually resulting in the death of neurons. AD is notable for its insidious onset. Clinically, impairment is typically observed in episodic memory—due to either problems with learning or failures of retention. There are also deficits in language, visuospatial abilities, and executive function—with judgment and problem solving often joining memory as the earliest reported symptoms.
Other major types of dementia include dementia with Lewy bodies (DLB), vascular dementia (VaD), and frontotemporal dementia. DLB is now considered the second most common form of dementia, accounting for 15 to 20% of all cases. The key feature is aggregations of a protein called alpha-synuclein in subcortical and cortical areas of the brain; these deposits are called Lewy bodies. Parkinsonism (e.g., slowness, muscular rigidity, tremor, and impaired motor control) is observed in people with this form of dementia, along with falls, visual hallucinations, poor response to antipsychotic medications, disturbed sleep, fluctuating attention, and executive dysfunction (e.g., impaired judgment and problem solving). Autopsy results suggest that Lewy-related pathology and AD-type pathology often occur together.
VaD is characterized by cerebral infarcts (destruction of brain tissue due to blockage of blood supply) or other evidence of cerebrovascular disease. VaD often has an abrupt onset and progresses in a stepwise fashion. Most notably, VaD is found to impair executive functioning and psychomotor speed while leaving episodic memory relatively intact. Estimated prevalence of this type of dementia depends greatly on which diagnostic criteria are used. Autopsy studies suggest that prevalence of mixed AD with VaD is underestimated. With increased attention to vascular risk factors for AD, there is also recognition of common mechanisms in how these two forms of dementia originate.
Frontotemporal dementia entails loss of social awareness, disinhibition, changes in eating habits, and changes in speech output, but not a pronounced memory deficit. Neuropathologically, there may be aggregations in the brain of a protein called tau. This type of dementia typically emerges at a younger age than other dementias.
ESTIMATING GENETIC EFFECTS
Twin studies are a useful tool in estimating the importance of genetic factors in the emergence of dementia. Monozygotic (MZ) twin pairs (i.e., who come from a single egg) are regarded as being the same genetically. Dizygotic (DZ) twin pairs (i.e., from two eggs) share in principle half of their genetic makeup; effectively, they are siblings of the same age. The proportion of twin partners of affected twins who also have a disorder is called probandwise concordance. Probandwise concordance provides an indication of genetic risk. The magnitude of concordance rates for MZ twin pairs and the difference in concordance between MZ and DZ twin pairs both suggest the extent of genetic influence. And when MZ concordance is less than 100%, it indicates that environmental influences or chance processes play a role.
We recently reported concordance rates for all dementia and for AD in twins from the Swedish Twin Registry (Gatz et al., 2006). These results are shown in Figure 1. Probandwise concordance for all dementias in men was 44% for MZ pairs and 25% for DZ pairs, and in women it was 58% for MZ pairs and 45% for DZ pairs. However, concordance rates are influenced by length of life—and hence, opportunity to develop dementia. Thus, although rates are higher for women than for men, once the age of the women was taken into account in quantitative genetic models there was no significant difference in genetic influence by sex.
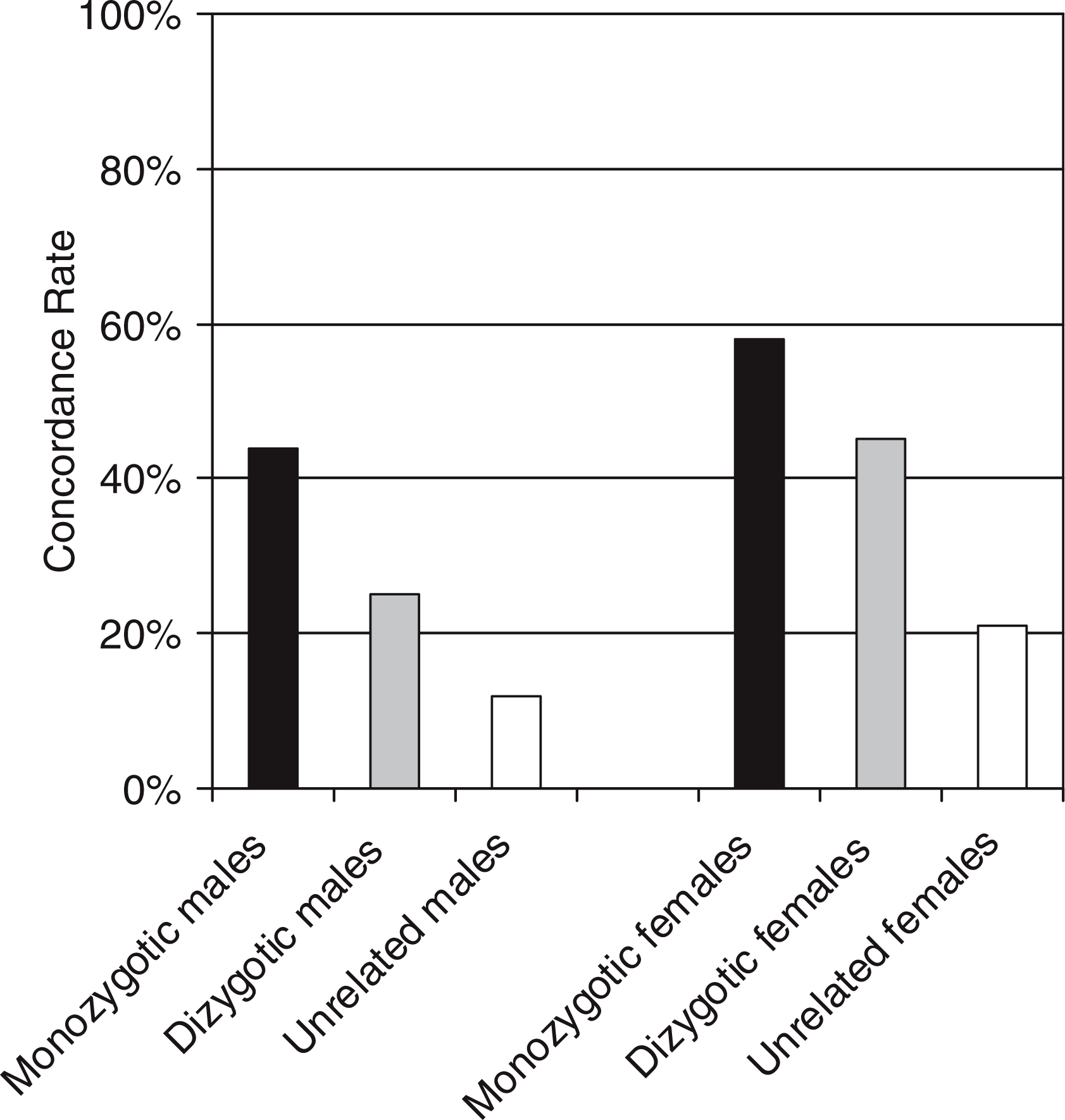
Probandwise concordance rates for dementia (i.e., likelihood of the partner being affected if one member of a pair has a disease), for monozygotic twin pairs, dizygotic twin pairs, and unrelated pairs sharing the same year of birth, by sex. The number of pairs represented by the columns are 428, 679, 1547, 655, 1009, and 1569, respectively.
Because dementia is age related, there is some chance that any two older adults of equivalent age can both be expected to be affected, independent of any shared genetic influences. From the same data, we created artificial pairs in which each individual was randomly coupled with an unrelated individual born in the same year. Converging results from thirty repetitions of this procedure are shown in Figure 1. Concordance was 12% and 21% respectively for male and female unrelated pairs matched by birth year. The comparison of concordance rates for MZ twins, DZ twins, and unrelated individuals highlights the influence of genetic factors for dementia vulnerability.
SPECIFIC GENES
A great deal of research attention has been devoted to identifying the genes underlying dementia (summarized by Tsuang & Bird, 2002). There are two kinds of genes—causative genes that follow an autosomal dominant pattern of inheritance, and susceptibility genes. Autosomal dominant means that the risk to each child of an affected parent is 50% and that inheriting one copy of the mutation is sufficient to develop the disease. Susceptibility genes alter an individual's chances of developing a disease or the age at onset of a disease but are not in themselves sufficient to cause the disease. Late-onset complex diseases such as AD are rarely due to a single causative gene, and susceptibility genes account for more of the genetic risk than do causative genes.
Three genes have been identified (see Table 1) in which particular mutations cause AD following an autosomal dominant pattern of inheritance, typically with an early age of onset. Mutations in these genes explain up to half of what is often called familial AD. However, because familial AD is so rare, these three established gene mutations account for under 2% of all cases of AD.
Mutations and Susceptibility Genes Associated With Dementia, Their Locations, and Possible Pathways by Which Susceptibility Genes Might Influence Risk of Alzheimer's Disease (AD)
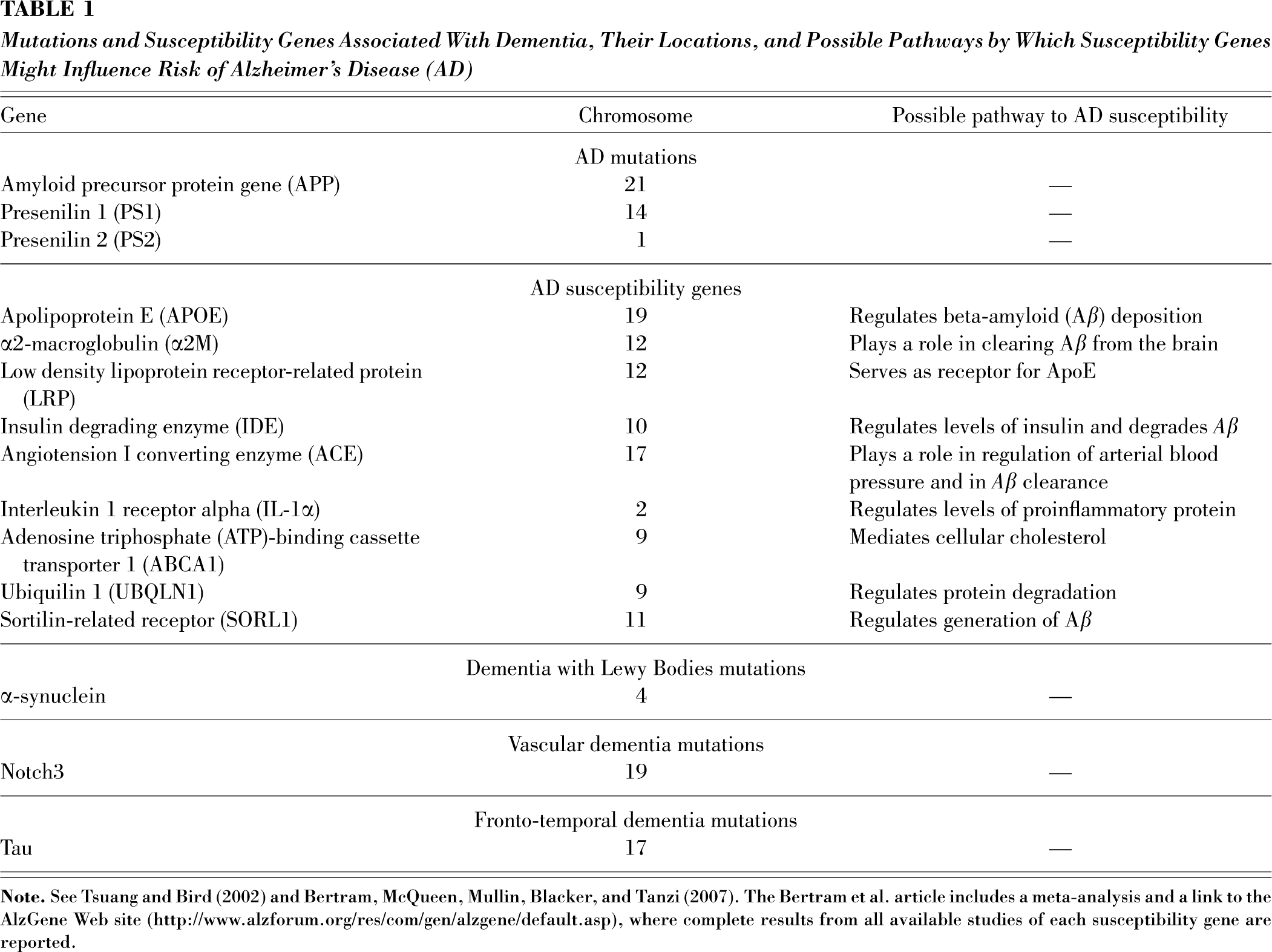
Genetic influences on AD are believed largely to stem from predisposing rather than causative genes. The major susceptibility gene identified to date is the apolipoprotein E gene (APOE). The ApoE protein is involved in the transport of cholesterol during neuronal growth and after injury and in the deposition of Aβ. The APOE gene has three versions or alleles—ε2, ε3, and ε4. Those who inherit an ε4 allele from one parent have greater risk of developing AD. There is a dose effect, with two ε4 alleles being more unfavorable than one. Some studies find that the ε2 allele is protective.
There is a higher occurrence of the ε4 allele in African Americans than in Whites. However, surprisingly, most reports find that APOE ε4 is not a significant genetic risk factor for African Americans.
Even including APOE, identified genes at best explain half of AD cases. It is estimated that there may be six or more additional susceptibility genes with major effects on risk of disease occurrence and age at onset (Bird, 2005). Susceptibility genes may each add quantitatively to an individual's personal risk. The more promising of these susceptibility genes are shown in Table 1. All of them relate to some aspect of how AD originates, as described earlier in this paper, lending plausibility to how each might contribute to increasing disease risk. A number of these genes have been investigated with Swedish twin data—including, for example, the gene for insulin-degrading enzyme (Prince et al., 2003). Research to date, however, is characterized by many failures to replicate findings across studies.
For other types of dementia, some specific mutations, also shown in Table 1, have been implicated, but only in rare forms of these conditions. As for AD, there are familial cases not explained by genetic discoveries to date.
The question of genetic testing for dementia sometimes arises. Genetic testing along with genetic counseling would be recommended in families in which one of the specific mutations is suspected. But at present, potential misuses of testing for susceptibility genes may outweigh the information gained.
GENE-BY-GENE AND GENE-BY-ENVIRONMENT INTERACTIONS
Most scholars believe that dementia results from a combination of several genes acting together (gene-by-gene interactions) and interactions between genes and multiple environmental factors (gene-by-environment interactions). In testing for gene-by-environment interactions, the environment term encompasses anything to which an individual is exposed—hypertension or education, for example—that might affect risk of dementia, although clearly these factors might themselves be influenced by other genes.
Gene-by-gene interactions have most often been examined by testing APOE ε4 carrier status in concert with some other susceptibility gene Findings have generally not shown consistent evidence of interaction. The ability to find reliable results and to test complex interactions among multiple genes should become possible with larger databases and more sophisticated analytic approaches (Bertram, McQueen, Mullin, Blacker, & Tanzi, 2007).
Finding gene-by-environment interactions has proved elusive. Where there have been significant results, they have not always been intuitive. In African American participants from the Indianapolis-Ibadan Dementia Project, for example, lower total serum cholesterol was related to reduced risk of AD only in those who carried no ε4 alleles (Evans et al., 2000). In Cardiovascular Health Study participants, it was found that estrogen replacement therapy (ERT) was related to lower risk of becoming cognitively impaired, but only among women who carried no ε4 alleles (Yaffe, Haan, Byers, Tangen, & Kuller, 2000), and that physical exercise was significantly associated with reduced risk of subsequently developing dementia, but, again, only among ε4 noncarriers (Podewils et al., 2005). In analyses of MZ twins from Sweden, intrapair differences in depressive symptoms were associated with intrapair differences in cognitive decline. However, for both estrogen receptor alpha (ESR1) and APOE, the association between depressive symptoms and cognitive decline was found only for noncarriers of the risk alleles (Reynolds, Gatz, Berg, & Pedersen, in press).
Thus, although individuals who have a positive family history for AD are particularly interested in what steps they might be able to take to reduce their chances of developing dementia, the preponderance of findings suggests that lifestyle factors—such as diet, ERT, physical exercise, and exposure to depression-evoking contexts—may be more important for those who are not at genetic risk than for those who are. People with a positive family history or who know that they are ε4 carriers are still left with remarkably little reliable guidance about what might be protective.
For vascular dementia, health habits related to preventing stroke—e.g., avoiding smoking, obesity, and hypertension—are relevant to prevention. Further advances in understanding genetic risk and potential gene-by-environment interactions are likely to arise from identifying genes that make brain tissue more or less susceptible to vascular injury.
CONCLUSIONS AND FUTURE DIRECTIONS
Taken together, twin studies and molecular-genetic studies indicate that genetic factors are clearly important in dementia, especially AD. A major new effort called the AD Genetics Initiative, funded by the National Institute on Aging, is being undertaken to identify these genes. Yet, equally evident is that genetic factors are only part of the picture, and finding the causes of dementia must entail more than a search for genes.
Clinical trials and experimental studies, including animal studies and neuroimaging work, will be useful complements to epidemiological studies in obtaining evidence about the gene-by-environment interactions. Future research might also build on twin studies—for example, focusing on MZ pairs who share particular susceptibility genes but in which only one of the pair has dementia.
Finally, epigenetic phenomena may play a key role in explaining dementia. Epigenetic differences refer to changes in genetic material that arise during development. These could be seen as chance events during DNA replication that do not alter the DNA sequence but change whether a particular gene is active or not. Twin studies are an important tool because identical twins can accumulate differences between them due to epigenetic modifications (Wong, Gottesman, & Petronis, 2005). Discordance for dementia among monozygotic twin pairs could be explained by epigenetic differences arising by chance, differences in environmental influences, or environmental factors that have a long-term influence on epigenetic modifications.
Footnotes
Acknowledgements
Research described in this article was supported in part by National Institute on Aging Grant R01AG08724. I am grateful for comments by Malcolm Klein, Chandra Reynolds, and Martha Storandt.