
Abstract
Levels of loneliness are relatively stable across most of adult life, but correlates of loneliness show age differences. We review evidence of age differences in associations between loneliness and individual differences in health behaviors, stress exposure, physiological stress responses, appraisal and coping, and restorative processes. The effects of each of these pathways endow loneliness with the capacity to accelerate the rate of physiological decline with age. Additional research across the lifespan is required to understand the nature of accrued loneliness effects on health behavior and physiology in the short and long term.
Research over the past several decades has repeatedly shown that a lack of social ties increases risk for poor health (e.g., Seeman, 2001). In light of this research, sociodemographic changes in American society indicate a disturbing trend toward increased social isolation. General Social Survey respondents in 2004 were three times more likely than respondents in 1985 to report having no one with whom to discuss important matters (McPherson, Smith-Lovin, & Brashears, 2006). The modal respondent reported three confidants in 1985 and no confidants in 2004. As social isolation becomes more prevalent, so does loneliness (Wenger & Burholt, 2004). Older adults are disproportionately represented in the growing segment of socially isolated adults, and despite increased prevalence of loneliness in older adults, loneliness levels are relatively stable across the lifespan, at least until oldest old age (i.e., 85 years and older; e.g., Demakakos, Nunn, & Nazroo, 2006).
Age-related similarities in loneliness levels do not necessarily mean age-related similarities in the correlates or consequences of loneliness, however. Our theoretical model, illustrated in Figure 1, posits that loneliness contributes to, and accelerates, age-related decreases in physiological resilience through its influences on health behaviors, stress exposure, psychological and physiological stress responses, and restorative processes that replenish physiological reserves and fortify against future stress. This model extends prior work that examines some of these same pathways in the context of social integration and health (Seeman, 2001) by setting these processes in a life-span context. Social isolation increases risk for loneliness, but not all socially isolated people are lonely. We focus on the subjective experience of social isolation (i.e., loneliness) because in most normal circumstances perceived isolation is the proximate cause. Our working hypothesis is that loneliness hastens physiological decline through its association with one or more pre-disease pathways, and that the contributory pathways may differ in kind and potency across the lifespan. In addition, we expect that loneliness differences in physiological reserves will be evident primarily in precursors to disease in younger adults (e.g., alterations in physiological functioning that may indicate subclinical disease processes), whereas loneliness-related influences on slowly progressing physiological disease processes will eventually manifest as frank disease and dysregulation across multiple physiological systems in older adults.
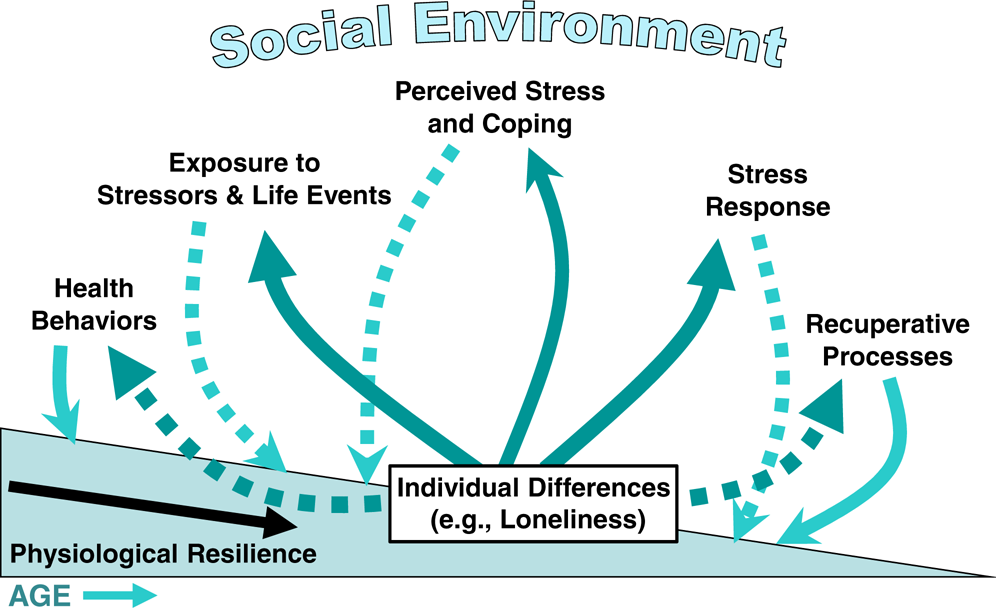
Loneliness and individual differences in the rate of age-related declines in physiological resilience. Loneliness may influence the rate at which physiological reserves decrease with age through its (a) adverse impact on health-promoting behaviors, (b) association with increased exposure to stressful events, (c) effects on appraisal and coping processes that increase the stressfulness of a given experience, (d) contribution to the quality and intensity of psychological and physiological stress responses, and (e) influence on the efficacy of restorative processes (e.g., sleep) that replenish physiological reserves and fortify against future stress. Solid lines denote enhanced influences and dashed lines denote diminished influences.
LONELINESS, AGING, AND PHYSIOLOGICAL RESILIENCE
The accrual of loneliness effects with age is well illustrated in a recent longitudinal study (Caspi, Harrington, Moffitt, Milne, & Poulton, 2006). In this study, social isolation in childhood and feelings of loneliness in adolescence and young adulthood predicted how many cardiovascular risk factors (e.g., body mass index, waist circumference, blood pressure, cholesterol) were elevated in young adulthood (mean age = 26 years). Moreover, the number of developmental occasions (i.e., childhood, adolescence, young adulthood) at which participants were lonely predicted the number of elevated risk factors in young adulthood. These data suggest that the effects of loneliness accrue in a dose-response fashion to accelerate the rate of physiological decline.
If loneliness effects accrue across the lifespan, then we might see age differences in the relative importance and/or potency of causal pathways through which loneliness acts to diminish resilience. Here, we review evidence for age differences in associations between loneliness and (a) health behaviors, (b) stress exposure, (c) stress appraisals and coping, (d) physiologic stress responses, and (e) recuperative processes across the adult life span from young adulthood to old age (i.e., 18–84 years). We draw primarily upon our prior research on loneliness in a sample of 135 young-adult undergraduate students (18–25 years old, with a mean age of 19) whom we recruited from more than 2,500 students at the Ohio State University (OSU) and studied extensively, and a population-based sample of 229 middle- and older-aged Caucasian, Black, and Hispanic men and women (50–68 years old, with a mean age of 57.4) in the Chicago Health, Aging, and Social Relations Study (CHASRS) whom we have followed for 5 years. We discuss other relevant research to the extent it exists, but with few exceptions, most of the research to date has dealt only with age differences in loneliness, not age differences in associations between loneliness and the causal pathways we consider here. Research in the latter area is much needed.
Health Behaviors
Poor health behaviors are appealing mechanistic candidates for associations between loneliness and health. High-calorie, high-fat diets and sedentary lifestyles, for example, contribute to being overweight or obese, major risk factors for disease in Western society. In our survey of over 2,500 OSU undergraduates (mean age = 19.1 years), loneliness was associated with a slightly greater body mass index (BMI). In our CHASRS sample, loneliness showed no association with BMI, but in a large cross-sectional survey of 1,289 adults 18 years and older (mean age, 46.3 years), the lonely group had a higher mean BMI and a greater proportion of overweight/obese individuals than the nonlonely group did (Lauder, Mummery, Jones, & Caperchione, 2006). Regarding sedentary lifestyles, however, neither our OSU study of young adults nor the wide age-range sample surveyed by Lauder et al. (2006) revealed loneliness differences in physical activity. On the other hand, in Lauder et al.'s (2006) sample, smoking was more prevalent in the lonely group than it was in the nonlonely group.
Stress Exposure
Stress is inevitable, and age brings with it a growing history of stressful experiences. In our OSU sample of young adults, the number of major life events failed to distinguish lonely from nonlonely individuals. In addition, their daily diaries showed no loneliness-related differences in reports of types of activities, behaviors, and experiences that might indicate differential exposure to stress (Hawkley, Burleson, Berntson, & Cacioppo, 2003). In our CHASRS sample of middle- and older-age adults, major life events were not more prevalent in lonely individuals than in nonlonely ones, but lonely individuals reported a greater number of chronic stressors (e.g., financial, work, marital, social, residential, caregiving, and general difficulties in daily life) than did nonlonely individuals (6.0 vs. 4.8; Hawkley, Hughes, Waite, Masi, & Cacioppo, 2007). In addition, lonely adults in the CHASRS sample recalled a greater number of childhood adversities (e.g., childhood hospitalization, parental divorce, physical abuse) than their nonlonely counterparts did (1.6 vs. 1.2 events), and the present-day negative effects of those events were perceived as more potent by lonely participants than by nonlonely participants (Hawkley et al., 2007).
Stress Appraisals and Coping Styles
Stress appraisals and threat perceptions are associated with patterns of physiological activity that work to the detriment of physiological resilience and health and may therefore contribute to accelerated physiological decline with age in lonely individuals. Lonely and nonlonely young adults in our OSU study did not differ in the frequency or diversity of their everyday activities, but lonely students rated those same activities as more stressful and themselves as less capable of meeting the challenges of daily activities than did nonlonely students (Hawkley et al., 2003). Similarly, in our CHASRS sample, feelings of helplessness and threat were greater among lonely individuals than among nonlonely individuals (Hawkley et al., 2007).
Lonely individuals also employ different coping strategies than nonlonely individuals do. In the OSU sample, loneliness was inversely associated with active coping, seeking emotional support, and seeking instrumental support, and was positively associated with behavioral withdrawal (i.e., the tendency to “give up” or “quit trying” to deal with a stressor; Cacioppo et al., 2000). In the CHASRS sample, lonely individuals again were found to be less likely to seek emotional support and more likely to report behavioral withdrawal (Hawkley et al., 2007)—coping styles that tend to perpetuate stress.
In addition, lonely individuals may employ qualitatively different behavioral coping strategies with increasing age. In our CHASRS sample, loneliness was associated with a higher probability of membership in a religious group among those over but not under the median age of 57 years (43% of lonely vs. 35% of nonlonely individuals over 57 years old; Hawkley et al., 2007). To what extent religious affiliation is an effective coping strategy for lonely individuals in older age remains to be determined.
Stress Physiology
Age differences in the manifestations of loneliness are most apparent in physiology. In young adults, homeostatic processes are generally effective in regulating physiological endpoints within a normal range, but persistent situational demands, real or perceived (e.g., acute or chronic stress, feelings of loneliness), can result in resetting of homeostatic regulatory mechanisms to new operating levels (Sterling & Eyer, 1981). These changes in physiology signal risk for disease and can be evident early in life (Caspi et al., 2006).
Cardiovascular Physiology
Blood pressure is a physiologically regulated endpoint that is determined by total peripheral resistance (TPR), a measure of resistance to blood flow resulting from the constriction of small arteries in the vascular system, and cardiac output, the amount of blood the heart ejects each minute. Lonely young adults exhibit higher levels of TPR than nonlonely individuals do, but levels of systolic blood pressure (SBP) do not differ as a function of loneliness (Cacioppo, Hawkley, Crawford, et al., 2002; Hawkley et al., 2003). Maintenance of equivalent blood pressure in the face of elevated TPR speaks to the physiological resilience of young adults. However, over time, increased TPR contributes to a degradation of homeostatic mechanisms and a gradual increase in SBP, at least until approximately 55 years of age, after which arterial stiffening plays an increasingly important role (Franklin et al., 1997). In our CHASRS sample of 50- to 68-year-olds, lonely adults did, in fact, have significantly higher SBP than their nonlonely counterparts did, and this effect was independent of depressed affect, perceived stress, social support, and hostility (Hawkley, Masi, Berry, & Cacioppo, 2006). Moreover, a significant loneliness-by-age interaction showed that the older the participant, the stronger the association between loneliness and SBP.
Neuroendocrine Physiology
Physical and psychological stressors activate the sympathetic adrenomedullary system and the hypothalamic-pituitary-adrenocortical (HPA) axis, physiological pathways that may contribute to loneliness differences in resilience. In young adults, loneliness was not associated with plasma levels of either epinephrine or norepinephrine, stress hormones released upon activation of the sympathetic adrenomedullary system (Cacioppo, Hawkley, Crawford, et al., 2002). However, in middle-aged and older adults, loneliness was associated with significantly greater urinary epinephrine excretion in an overnight urine sample (Hawkley et al., 2006). Higher levels of overnight urinary epinephrine reflect higher blood levels of circulating epinephrine and indicate greater activation of the sympathetic adrenomedullary system in lonely than nonlonely adults, consistent with greater loneliness-related wear and tear of this physiological system with age.
Loneliness differences in the activity of the HPA axis have been observed in young and older adults. In a diary study of young adults, loneliness ratings over a period of 1 week were associated with higher morning and night-time levels of salivary cortisol, indicative of greater activation of the HPA axis in lonely than nonlonely individuals (Pressman et al., 2005). In a healthy sample of middle-aged adults (47 to 59 years), loneliness was associated with a greater cortisol response to awakening (Steptoe, Owen, Kunz-Ebrecht, & Brydon, 2004), and in our sample of 50- to 68-year-olds, loneliness feelings reported in two end-of-day diaries predicted a higher cortisol response to awakening each subsequent day (Adam, Hawkley, Kudielka, & Cacioppo, 2006). Given the importance of the HPA axis in controlling inflammatory processes and maintaining immune function, it is worth noting that lonely young adults also exhibited poorer response to a vaccine than their nonlonely counterparts did (Pressman et al., 2005). Impairments in HPA regulation across the adult years could play a particularly important role in the development of glucocorticoid insensitivity (a compromising of the normal feedback mechanism in which increasing levels of cortisol turn off the release of yet more cortisol) and impairments in the regulation of inflammatory processes, thereby accelerating the rate of decline in physiological resilience among lonely individuals.
Recuperation
Counteracting the forces that drain physiological reserves are forces that shore up the organism against physiological assault. Among these restorative anabolic forces is sleep. In young adults who wore a “Nightcap” that enabled us to distinguish between wake, REM, and non-REM states, loneliness was associated with poorer sleep as defined by more micro-awakenings (Cacioppo, Hawkley, Berntson, et al., 2002). Lonely young adults also reported longer sleep latency and greater daytime dysfunction, even though Nightcap estimates of actual sleep hours did not differ between lonely and nonlonely individuals (Cacioppo, Hawkley, Berntson, et al., 2002; Cacioppo, Hawkley, Crawford, et al., 2002). Similar findings were evident in our pilot study of elderly adults (mean age, 65 years; Cacioppo, Hawkley, Crawford, et al., 2002). Moreover, among 70-year-old adults in the Jerusalem Cohort Study, loneliness at study onset proved to be a significant risk factor for sleep dissatisfaction 7 years later (Jacobs, Cohen, Hammerman-Rozenberg, & Stessman, 2006). With increasing age and the accrual of more stress, sleep benefits may be even more limited, thereby further hastening the decline of physiological reserves in lonely individuals.
FUTURE DIRECTIONS
Despite the absence of age differences in loneliness across most of the adult lifespan, associations between loneliness and health-relevant psychological and physiological processes show some age differences in type and/or strength. Research on age-related changes or differences in associations between loneliness and health-related processes is limited, however. For instance, a search of Medline (January, 1996, to January, 2007) that crossed the terms loneliness (subject or keyword) and aging (subject or keyword) or age differences (keyword) produced 87 articles, and only 11 of these were relevant to the mechanistic pathways to diminished resilience that we outlined in our model. A similar search in PsycInfo (January, 1985, to January, 2007) generated 210 journal articles, but fewer than a dozen were relevant to this focus. According to our model, the rate of age-related declines in physiological regulation and resilience can be modulated by perceived social connection or isolation. This postulate is supported by our research showing that loneliness is associated with elevated vascular resistance in young adults and higher blood pressure in older adults. Long-term longitudinal research is needed to determine whether the diminution in the regulation of blood pressure is attributable to the influence of chronic loneliness.
Future research is also needed to determine the extent to which chronic loneliness may have deleterious effects on other physiological regulatory systems (e.g., metabolic, neuroendocrine) as individuals age, and to determine whether such adverse effects accrue also in the domains of social and behavioral regulation. Given the aging of the population, the increases in the prevalence of social isolation, and the rising costs of health care, it is imperative that we gain a better understanding of the means by which loneliness influences health and well-being.
Footnotes
Acknowledgements
Funding was provided by the National Institute of Aging Grant No. PO1 AG18911 and the John Templeton Foundation.