
Abstract
Research over the last decade has provided compelling evidence that the ability to engage with music is a fundamental human trait, yet the biological basis of music remains largely unknown. Recent findings indicate that a small number of individuals have severe musical problems that have neurogenetic underpinnings. Such deficiencies are termed congenital amusia, an umbrella term for lifelong musical disabilities that cannot be attributed to mental retardation, deafness, lack of exposure to music, or brain damage after birth. Congenital amusia constitutes a natural experiment, giving us a rare chance to examine the biological basis of music by tracing causal links among genes, environment, brain, and behavior.
Humans are born with the potential to both speak and make music. For the musically untrained majority, this fundamental human trait is expressed by avid listening and occasional dancing and singing. The propensity to engage in music ultimately gives rise to a sophisticated music processing system that is largely acquired implicitly by experience (Peretz, 2006). However, a minority of individuals never acquire this core musical system, either in part or in total. This condition affects 4% of the general population (Kalmus & Fry, 1980). It has been variously called note deafness, tone deafness, tune deafness, dysmelodia, and, more recently, congenital amusia (Peretz & Hyde, 2003). All of these terms refer to the same condition: A lifelong deficit in melody perception and production that cannot be explained by hearing loss, brain damage, intellectual deficiencies, or lack of music exposure. I coined the term congenital amusia to acknowledge the possibility that there may exist as many forms of congenital amusias as there are forms of acquired amusias, which arise as the consequences of accidental brain damage. The term congenital means simply “present from birth”; it defines a likely time period but not the etiology. Recent research has made major progress, however, regarding the etiology of this disorder. The goal of the present article is to summarize the current evidence.
The main reason for studying congenital amusia is that such disorders offer unique insight into the behavioral, neural, and genetic bases of cognitive functions in general and of music cognition in particular. The framework adopted here closely follows that of work conducted on language disorders (e.g., Bishop & Snowling, 2004). It makes a distinction between observed behavior, cognitive processes, neurobiology, and etiology. Like language, musical abilities result from genes and environmental factors that guide brain development and shape cognitive functions by affecting neural processes such as migration of neurons, cell death, and connectivity. An anomaly observed at the behavioral level can be traced back to cognitive processes, then to brain processes, and ultimately to genes and environment. As indicated in Figure 1, anomalous behavior may also influence the environment, such that the effect is somewhat circular. For example, an amusic person may avoid challenging musical situations and, consequently, live in a musically impoverished environment. It is also possible that amusic children seek music training to compensate for their difficulties, such that by adulthood they may no longer appear to have a severe problem. Both situations would have deep influences on brain and cognition. In short, the paths from etiology to cognition via neurobiology are not simple, but they are tractable, as illustrated here with congenital amusia.
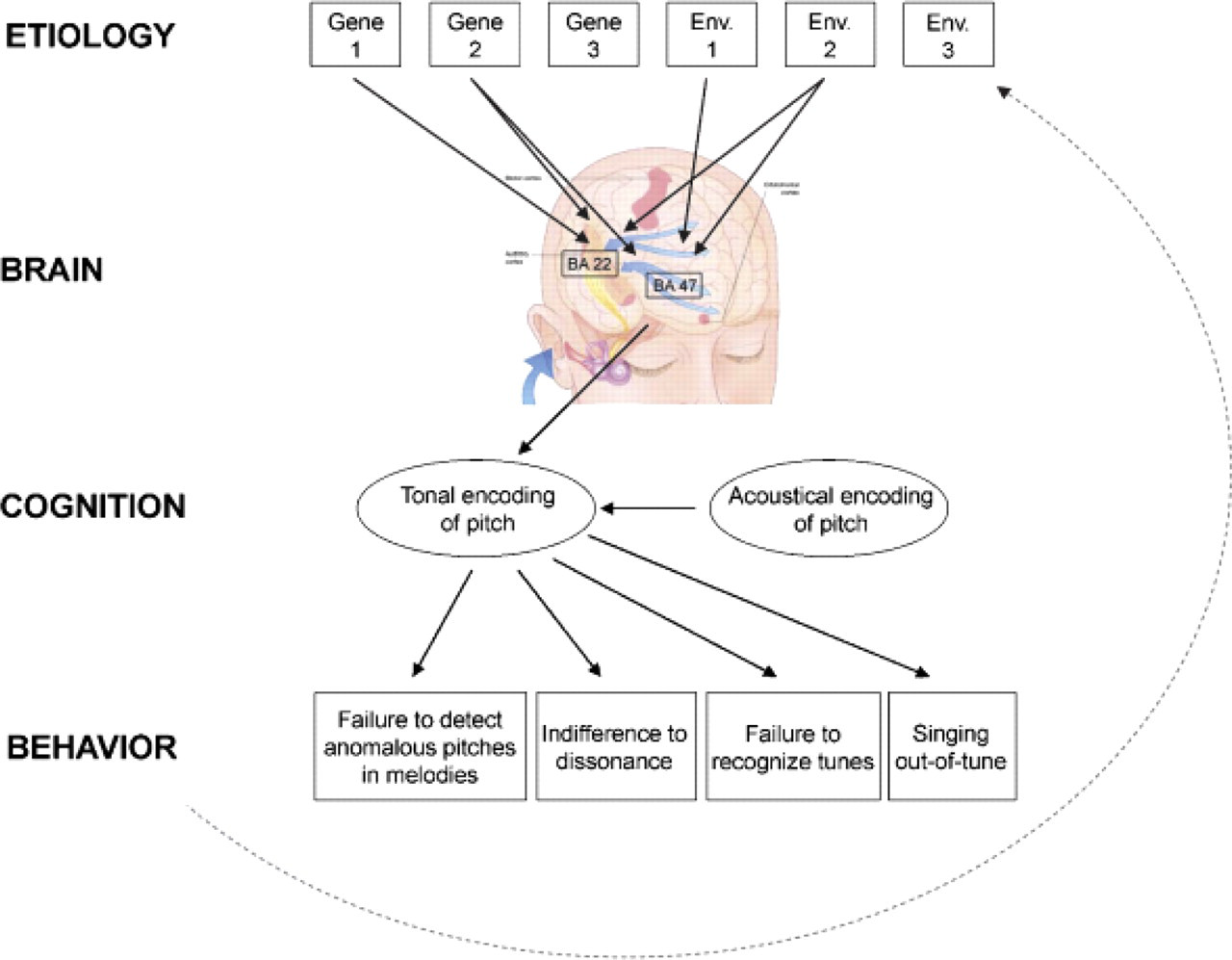
Levels of causation for the perceptual form of congenital amusia. The musical deficits observed at the behavioral level (bottom) can be related to a difficulty interpreting melodic pitches in terms of musical tonal rules. This impairment at the cognitive level (tonal encoding of pitch) may arise partly from a subtle problem in acoustical encoding of pitch. The musical-pitch disorder probably results from an anomalous connectivity between the auditory associative cortex (BA 22) and the inferior frontal gyrus (BA 47). The brain anomalies should be ultimately traced back to genes (etiology, top row) since congenital amusia is hereditary. Genetic predispositions will be modulated by environmental factors (e.g., musical rehabilitation during childhood). The dashed line emphasizes that behavior can affect the environment (e.g., avoidance of musical activities).
BEHAVIOR
At the level of observed behavior, congenital amusia appears to be domain-specific (Peretz & Hyde, 2003). As first noted by Allen (1878; see Peretz & Hyde, 2003, for a review) more than a century ago, amusic individuals enjoy a normal life. They may even excel in certain domains, as illustrated by well-known figures such as Che Gevara (who studied medicine), Sigmund Freud (who lived in a musical capital), and Milton Friedman (who was awarded a Nobel Prize for economics). Nevertheless, these individuals exhibited severe problems with music perception. What distinguishes amusic individuals from ordinary people is their inability to recognize a familiar tune without the aid of the lyrics, their inability to detect when they sing out of tune, and their difficulty judging whether two melodies are the same or different, especially on the pitch dimension. They also show little sensitivity to the presence of obvious pitch violations in melodies and of dissonant chords in classical music (Ayotte, Peretz, & Hyde, 2002). The associated rhythm deficit that is observed in about half of such individuals seems to result from the presence of pitch variations in melodies. When presented with rhythmic sequences from which pitch variations are removed, amusic subjects discriminate them as well as control subjects do (Foxton, Nandy, & Griffiths, 2006). In sum, the core deficit concerns the processing of pitch in a musical context.
In speech, the processing of pitch information (intonation) is relatively spared, at least in the vast majority of the amusic subjects tested so far in nontonal languages (e.g., Patel, Wong, Foxton, Lochy, & Peretz, 2008). This might be related to the fact that pitch variations in nontonal languages are very coarse as compared to those used in music. Meaningful pitch changes are in the order of 5 to 12 semitones in both English and French. In contrast, Western melodies have steps between consecutive notes of 1 or 2 semitones (a semitone corresponds to the smallest pitch distance used in Western music; Peretz & Hyde, 2003). Thus, a pitch-perception difficulty is more likely to manifest itself in music than in speech.
Clearly, the behavioral signature of amusia, or its phenotype, depends on how the disorder is defined. Fortunately, all current research on amusia is using the same tool to establish whether an individual is amusic or not. The current tool is the Montreal Battery of Amusia Evaluation (Peretz, Champod, & Hyde, 2003). It involves six tests (180 stimuli) that assess the different components that are known to be involved in melody processing of Western tonal music: pitch contour, musical scales, pitch intervals, rhythm, meter, and memory. Self-declared amusic individuals whose global score (averaged across the six tests) lies two standard deviations below the mean of normal controls are typically considered as confirmed cases. In many laboratories, including our own, the test that is most diagnostic of amusia requires participants to detect out-of-key notes in conventional but unfamiliar melodies. A behavioral failure on this test is diagnostic because there is no overlap between the distributions of the scores of amusics and controls (e.g., Ayotte, Peretz, & Hyde, 2002). This musical-pitch disorder represents a clear-cut phenotype that can serve to identify the associated neurogenetic factors, as I will summarize.
PERCEPTUAL ORIGIN
What amusics seem to be lacking is a pitch-processing component that is normally and automatically acquired by ordinary listeners early in life, and that is essential for processing music but not speech. The problem may occur at an acoustical stage of processing. Indeed, amusic individuals are impaired in detecting pitch directions (Foxton, Dean, Gee, Peretz, & Griffiths, 2004) and pitch deviations that are smaller than two semitones in tone sequences (Hyde & Peretz, 2004), as well as in tone pairs. Given that amusic individuals are probably born with such an elemental deficit (normal infants' pitch acuity is in the order of half a semitone), they have probably never assimilated the structure of musical scales nor acquired the sophisticated knowledge that every normally developing individual implicitly builds on that structure. Thus, a perceptual system that is unable to detect small pitch changes is bound to miss an essential part of music (Peretz & Hyde, 2003).
We refer to this essential processing component as “tonal encoding of pitch” (Peretz, 2006). By tonal, we mean that pitch is encoded in terms of the tonal system that characterizes one's musical environment. That is, in the Western music system, pitches are organized around a central tone called the tonic. Usually, a musical piece starts and ends on the tonic. Among the other tones of the key, there is a hierarchy of importance or stability. The out-of-key tones are the least related and often sound anomalous. Normal detection of an out-of-key note in the melody is one of the behavioral manifestations of implicit tonal knowledge. Lacking this knowledge has numerous cognitive consequences. The tonal hierarchical organization of pitch is central to music because it facilitates perception, memory, and performance by creating expectancies about future auditory events (Tillmann, Bharucha, & Bigand, 2000). Thus, a perceptual system that is unable to acquire this tonal knowledge and procedures will miss an essential component of music, as seen in congenital amusia.
BRAIN ANOMALIES
On gross inspection, amusic brains do not have any detectable neurological abnormality. Neural anomalies are detected only when series of amusic brains are considered in fine-grained automated analyses of magnetic resonance images. My colleagues and I highlighted the fact that amusic brains, compared to controls, have less white matter in the right inferior frontal cortex (BA 47), while they have thicker cortex in the same right inferior frontal area and the right auditory area (BA 22; Hyde, Lerch, Zatorre, Griffiths, Evans, & Peretz, 2007). Decreases in grey matter in the same two regions on the left side of the brain have been uncovered in another amusic sample (Mandell, Schulze, & Schlaug, 2007).
These anomalies that point to abnormal neuronal migration or proliferation in the auditory cortex and inferior frontal gyrus are consistent with anomalies during cortical development (Ramus, 2006). The findings are also consistent with the functional neuroimaging literature, which demonstrates that BA 22 and 47 are important in musical-pitch processing in the normal brain. These regions have been implicated in the active retention of pitch in melodies (Zatorre, Evans, & Meyer, 1994) and in the processing of tonality in the detection of unexpected chords (in the adjacent areas of BA 44/45; e.g., Tillmann et al., 2006). The involvement of the frontal areas is also consistent with measurements of electrical activity in the amusic brain that show abnormalities in relatively late brain potentials along the right auditory temporo-frontal pathway (Peretz, Brattico, & Tervaniemi, 2005). Thus, congenital amusia appears to be a neurodevelopmental disorder that can be explained by an impoverished communication in a right, or perhaps bilateral, temporo-frontal neural network.
The abnormal temporo-frontal connectivity that would characterize congenital amusia differs from the brain anomalies identified in other neurodevelopmental disorders such as language disorders and face-recognition disorders (congenital prosopagnosia). For example, abnormally high levels of grey matter, but in another portion of the superior temporal gyrus, have also been highlighted in speech and language disorders, while reductions have been found in various motor-related systems (Vargha-Khadem, Gadian, Copp, & Mishkin, 2005). In congenital prosopagnosia, a significant reduction is observed in the anterior fusiform gyrus, which is related to the face-recognition deficit (Behrmann, Avidan, Gao, & Black, 2007). Although similar cortical malformations (in grey matter for instance) have been noted across neurodevelopmental disorders, the cortical anomalies do not appear to occur in the same brain areas. Given that the disorders are both cognitively distinct and hereditary, the identification of different anatomical bases for the disorders suggests different genetic alterations.
GENETIC FACTORS
Cortical anomalies provide a crucial link in the understanding of the chain of events through which a genetic mutation may result in a disorder. If amusia is indeed a disorder of neural connectivity, we can narrow down the search for the genes that encode fronto-temporal fiber tracks. To estimate if congenital amusia can be genetically transmitted, its prevalence was quantified by auditory testing in 71 members of 9 large unrelated families of amusic individuals, as well as in 75 members of 10 control families. The results confirm that congenital amusia is expressed by a deficit in processing musical pitch but not musical time, and also show that the pitch disorder has a hereditary component. In amusic families, 39% of first-degree relatives have the same cognitive disorder, whereas only 3% have it in the control families. The identification of multigeneration families with a high relative risk for experiencing a musical-pitch deficit enables the mapping of genetic loci for hereditary amusia (Peretz, Cummings, & Dubé, 2007).
The finding of a genetic component to the disorder in terms of musical-pitch processing is consistent with the results obtained in a twin study. In a test requiring the detection of pitch violations in melodies, monozygotic (i.e., identical) twins obtained more similar scores than did dizygotic (i.e., fraternal) twins. Genetic model-fitting indicated that the influence of shared genes was more important than that of shared environments, with a heritability of 70 to 80% (Drayna, Manichaikul, de Lange, Snieder, & Spector, 2001).
What is currently unknown is the impact of environmental factors on this genetic vulnerability. One question for future research is to describe the specific mechanisms that explain how genes interact with the environment to produce congenital amusia.
CONCLUSIONS AND A QUESTION FOR FUTURE RESEARCH
As illustrated here, congenital amusia can offer special insight into the behavioral, neural, and genetic bases of music cognition. In this perspective, music disorders are as interesting as language disorders because both types of disorder provide unique and complementary answers to fundamental questions of innateness and modularity (Patel, 2008). Such questions can only be answered by studying the full complexity of the relations among cognition, the brain, and genes.
One promising avenue is to study congenital amusia in relation to tone languages. Tone languages, such as Cantonese and Mandarin Chinese, use relatively subtle pitch differences to indicate word meaning. Thus, one might predict that (Western) amusic individuals might have difficulties learning a tone language due to their generally poor pitch abilities. Conversely, the prevalence of congenital amusia might be extremely rare in tone-language speakers. Early exposure to a tone language may compensate for the pitch disorder. Such an environmental influence may turn out to be difficult to distinguish from genetic factors. Indeed, a connection between the type of language (tone language) a population speaks and brain-growth related genes has been recently highlighted (Dediu & Ladd, 2007). It would be interesting to examine whether these genetic variations contribute to variations in both the acquisition of a tone language and the prevalence of congenital amusia.
Thus, the study of congenital amusia may modify the ways the processes of music acquisition and language acquisition are studied. Furthermore, if the development of music competence emerges, at least in part, from the integrity of a mechanism that mediates fine-grained specification of pitch, then early training at the acoustic level should affect music processes. Gaining insight into every aspect of congenital amusia should not only enrich current brain theories of normal and abnormal music development but may someday lead to therapies for afflicted individuals. Amusic individuals are often reluctant to acknowledge their deficit because they see it as a social handicap and, even worse, as a lack of a sensitivity that is basic to humankind. The study of the environmental factors that contribute to the emergence of amusia, or that may counteract its full expression, should be the goal of future studies. These findings will guide the development of possible interventions.
Footnotes
Acknowledgements
This work was supported by funding from the Canadian Institutes of Health Research and from a Canada Research Chair. I thank Lola Cuddy, Aniruddh Patel, Glenn Schellenberg, and Lauren Stewart for insightful comments.