
Abstract
People have long believed that adversity and stress contribute to emotional problems in general and to depression in particular. A considerable body of research has supported this intuition, documenting a consistent association between major stressful life events and the onset of clinical depression. However, most individuals under stress do not become depressed, sometimes depression develops without prior stress, and distinguishing psychological distress from major depression can be diagnostically challenging. In varying forms and degrees, life stress may play multiple roles in relation to major depression. In this article, we outline the opportunities and obstacles associated with conceptualizing depression from a life-stress perspective and discuss the implications for future research.
Keywords
However you are feeling at this moment—happy or sad, calm or anxious—is most likely related to what is happening in the immediate world around you. The daily ebb and flow of human emotions represent adaptive responses to life's ongoing demands, accomplishments, and disasters and are especially sensitive to changes in one's social environment. When our emotions are pushed to uncomfortable levels, we often describe ourselves as “stressed out,” “depressed,” or having an “emotional crisis,” and we blame our distress on the troublesome personal relationships, demanding careers, material losses, health issues, or other pressures and strains to which we may be exposed.
At their most extreme, significant shifts in mood, thought, and behavior cross over into the realm of psychopathology, where it remains appealing to invoke explanations involving the vicissitudes of life. Our understanding of a number of psychiatric and medical conditions—ranging from depression and anxiety disorders through coronary heart disease and the common cold—reflects the underlying premise that even a “normal” body or mind will eventually succumb to excessive life stress (Dohrenwend, 1999; Monroe, 2008). Yet ideas involving stress have also been invoked mistakenly to account for symptoms of psychopathology and disease in the absence of viable biological or psychological explanations. For example, prior to the discovery of the spirochete Treponema pallidum in 1913, the devastating and deadly condition of general paresis (or tertiary syphilis) was commonly ascribed to the “demands of civilization on physical and mental powers,” including “overwork,” “overstudy,” “competition,” and the “feverish pursuit of wealth and social position” (Kellogg, 1897). Although potentially useful, an overly flexible conceptualization of “stress” can opportunistically fill an explanatory vacuum and can serve as a self-contained, culturally legitimized account for almost any disorder or disease of unknown origins. People hunger for explanations, and poor explanations are often preferred to nothing at all. Consequently, ad hoc theories and research on stress in psychopathology and disease can lead to a proliferation of misleading ideas and practices (Monroe, 2008).
Current research on major depression still struggles with this question of when life stress is a useful explanatory construct as opposed to a misguided explanatory reflex (Monroe & Reid, 2008). When does the stress of life suggest a cause of depression, and when does it erroneously divert attention from other valid causal factors? By distinguishing the multiple roles life stress may play, and by addressing key research design and measurement issues, we believe that life stress will continue to yield useful information about the origins and nature of depression.
DEFINING AND DIAGNOSING THE PROBLEM: MAJOR DEPRESSION
Major Depressive Disorder (MDD; also called unipolar or clinical depression) is one of the most common and disabling psychiatric conditions. Current estimates suggest that approximately 16% of people in the United States suffer from MDD at some point during their lives, with women diagnosed with depression almost twice as often as men (Kessler et al., 2003). Also of great concern is the fact that depression is frequently recurrent and cyclical, or sometimes chronic. Depression is ranked as the fifth leading cause of disability among all diseases worldwide and is projected to become the second leading cause by the year 2020 (Michaud, Murray, & Bloom, 2001). Although highly prevalent in modern society, the disorder represents one of the most venerable of psychiatric conditions, with clear clinical descriptions dating back to ancient religious texts and medical writings (Jackson, 1986).
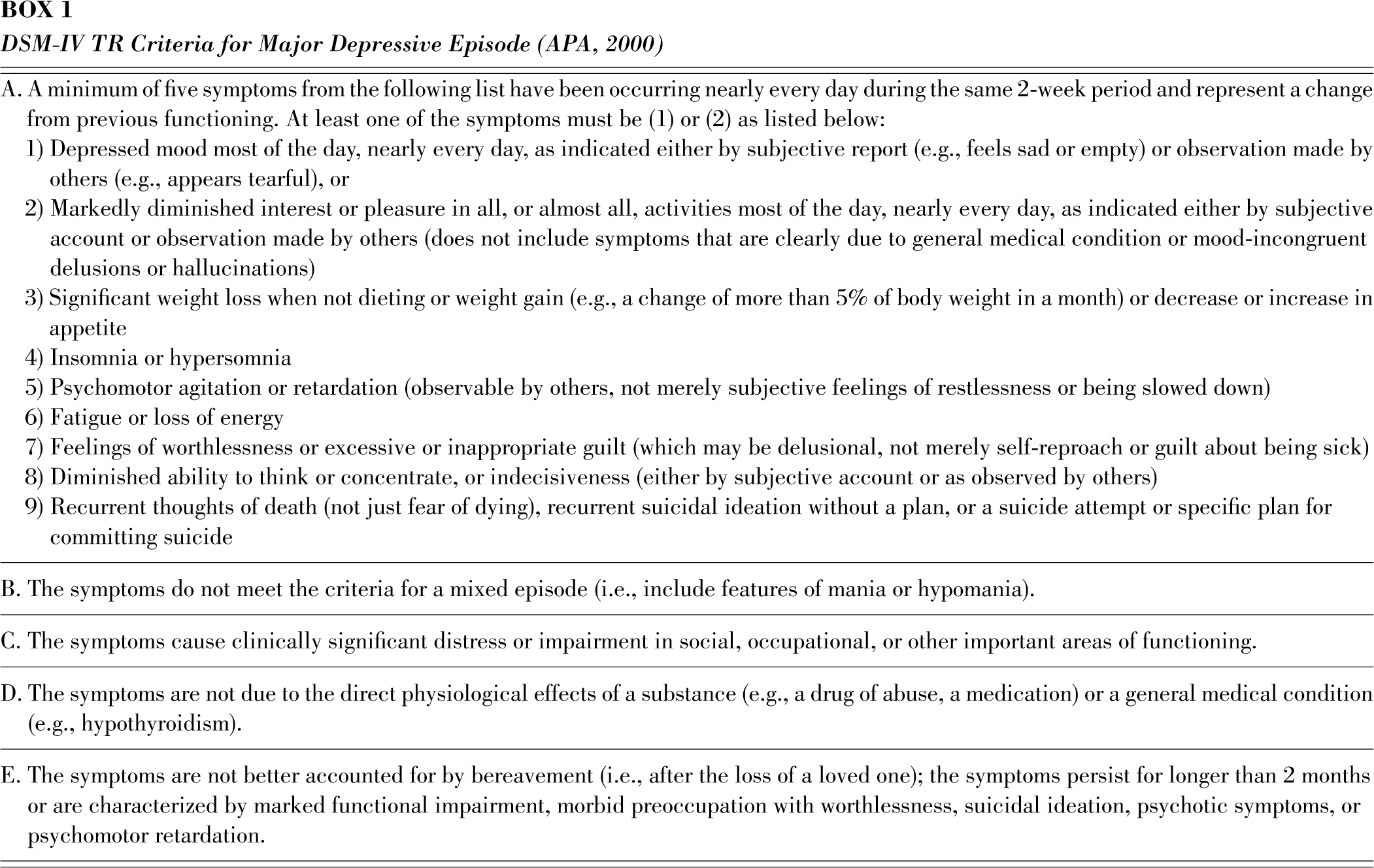
Currently, the diagnosis of MDD is based upon the fourth edition of the Diagnostic and Statistical Manual (DSM) of the American Psychiatric Association (APA, 2000) and requires clinical evaluation of the presence and duration of key signs and symptoms that constitute the defining features of the disorder (see Box 1). Over the past several years, there has been a dramatic increase in public awareness and acceptance of depression, spawned at first by public health initiatives in the 1980s and later by FDA approval of direct-to-consumer drug advertising for the pharmaceutical industry in 1997. At no other time in history has the general public been so well educated about depression, so aware of its defining features, and so informed of available treatments. “Being depressed,” clinically or subclinically, has become commonplace in our daily lives.
DSM-IV TR Criteria for Major Depressive Episode (APA, 2000)
LIFE STRESS AND MEASUREMENT MATTERS IN DEPRESSION RESEARCH
Major losses, setbacks in life, and other significant psychosocial events have long been thought of as precipitants of serious depressive conditions (Jackson, 1986). With the advent of modern stress theory and the development of life-event-checklist methodologies in the late 1960s, formal research examining life stress and depression proliferated (Monroe, 2008).
Critics soon contended that associations between stress and depression were attributable to poor research design or to faulty stress-measurement practices (Brown & Harris, 1978). For instance, early measures employing self-report life-event checklists commonly confounded life events with the actual symptoms of depression (e.g., major changes in eating or sleeping habits) or with the consequences of depression (e.g., occupational and relationship problems resulting from the depressed person's inability to function socially or professionally). Also, depression can have an insidious onset, with symptoms preceding and even contributing to the generation of subsequent life stress (Hammen, 2005).
Further, it is now recognized that respondents often interpret and respond to self-report checklist items idiosyncratically (Dohrenwend, 2006). Life events endorsed by subjects with self-report checklists match the nature of the event as intended by the investigator less than 50% of the time (Monroe, 2008). When compared with interview-based procedures, respondents commonly provide discordant information on these self-report measures, highlighting the advantage of more careful assessment and operationalization of life stress (McQuaid, Monroe, Roberts, Kupfer, & Frank, 2000). By utilizing these rigorous interview-based methods, research has not only supported the idea that stress causally precedes depression but also demonstrated the causal relevance of independent life events that are beyond an individual's control (Hammen, 2005; Mazure, 1998).
Based on these state-of-the-art life-stress measurement practices and sound research designs, it is now generally accepted that most people who develop major depression do so following major (but not minor) life stress (Hammen, 2005). It has been estimated that approximately 50 to 80% of depressed persons report a recent severely stressful life event prior to onset (Brown & Harris, 1989; Mazure, 1998). At a minimum, such events are among the strongest available markers of the likelihood of depression's impending onset. To what extent life stress is an actual maker of depression—a central etiological element—remains more debatable (Monroe, Slavich, & Georgiades, 2009).
WHY DOESN'T DEPRESSION ALWAYS FOLLOW AFTER MAJOR LIFE STRESS?
Although major stress commonly precedes depression's onset, the majority of people exposed to life stress do not break down. It is estimated that approximately one in five of those exposed to severe life events subsequently develop depression (although the proportion can be higher, depending upon the nature of the life event and other circumstances; Brown & Harris, 1989; Kendler, Hettema, Butera, Gardner, & Prescott, 2003). This indicates that other factors influence the depressogenic potential of life stress (Brown & Harris, 1978). For example, childhood abuse and early trauma have been associated with heightened risk for depression later in life, perhaps sensitizing individuals to the depressogenic effects of later stressors (Hammen, 2005). Social support, too, has been found to buffer individuals with high stress with respect to onset of depression. Genetic predisposition, biological susceptibility, and personality characteristics are all believed to influence the likelihood of developing depression after experiencing life stress (Brown & Harris, 1978; van Praag, de Kloet, & van Os, 2004).
Research examining genetic moderation of stress impact provides a promising explanation of why only some stressed individuals develop depression. A wealth of data suggests that genetically predisposed persons are especially sensitive to the adverse effects of major life stress. In a recent study, Caspi et al. (2003) found that individuals with one or two copies of the short allele in the serotonin-transporter-gene–linked polymorphic region (5-HTTLPR) were especially prone to develop depression following stressful life events. More than a dozen replications and meta-analytic reviews have underscored that genetic effects predict depression only in the context of heightened life stress (i.e., gene–environment interaction). However, the vast majority of studies examining this interaction suffer from serious life-stress-measurement and research-design limitations similar to those that plagued early life-stress research, again raising critical questions about ersatz or conflicting findings and misleading stress explanations (Monroe & Reid, 2008).
WHY DOES DEPRESSION SOMETIMES OCCUR IN THE ABSENCE OF MAJOR LIFE STRESS?
Kraepelin (1921), the great systematizer of modern psychopathology, maintained that some forms of depression “may be to an astonishing degree largely independent of external influences” (p. 181, italics in the original). For centuries, “sadness without cause” and “groundless sadness” have described those serious cases of depression without readily identifiable external precipitants (Jackson, 1986, p. 315). Efforts to establish subtypes of depression have often included a category of “endogenous” or “autonomous” depression, characterized by the absence of life stress. Debates about stress-related forms of depression (e.g., reactive depression) and stress-unrelated forms of depression (e.g., endogenous depression) have been numerous over many decades, producing extensive and often contentious debate (Hammen, 2005; Monroe et al., 2009). To date, there has been no resolution of the issue. Consequently, current diagnostic practices for MDD do not systematically evaluate the presence or absence of major life stress (e.g., APA, 2000).
For advancing research on depression, confirming the absence of significant life stress prior to depression's onset could be as vital as confirming its presence. Rigorous life-stress measurement practices may be instrumental for isolating a classic autonomous form of the disorder, in which depression occurs in persons whose lives appear relatively stress-free if not even advantaged and enviable. This hypothetical subtype of depression, characterized by “sadness without cause,” may easily be overlooked due to ubiquitous and superficial stress explanations or obscured by confounded stress measures and faulty research designs. These explanatory problems and measurement biases are minimized when rigorous stress-assessment procedures, which include precise definitions, operational criteria, and accurate dating of events and onset, are used (Monroe & Reid, 2008).
Although severe life events have commonly been found to precede the onset of a first lifetime episode of depression, severe life events are less often found to precede recurrences of the disorder (Monroe & Harkness, 2005). In other words, major life events may initiate one's first depressive episode, but “sadness without cause” may characterize subsequent recurrences. Current psychobiological theory posits that MDD is a dynamic process, in which liability to future episodes accrues over time as a result of prior stress and depressive experiences. Conceptually, this escalating tendency toward recurrence may involve one or more of three processes: (a) progressively less severe forms of life stress become capable of triggering recurrences (i.e., sensitization to life stress); (b) recurrences become more “spontaneous” and independent of life stress (i.e., non-stress-related biological factors predominate); or (c) highly susceptible individuals are inclined from the outset to incur many episodes of depression, regardless of life stress. Research evaluating these alternative viewpoints indicates the crucial distinction between a first lifetime episode and a first recurrence, and holds promise for predicting and managing the lifetime cycle of recurrences for this subset of people afflicted by the disorder. If the liability to recurrences accrues over time as one experiences more depressive episodes, the topics of early detection and potential prevention of depression become even more salient clinically (Monroe & Harkness, 2005).
THE FUTURE OF LIFE-STRESS RESEARCH IN DEPRESSION
We began this article by considering how people habitually interpret uncomfortable emotions in the context of their present life and social circumstances. But how are we to distinguish between understandable psychological distress and apparently inexplicable psychopathology? In an important sense, the psychology of adversity—the so-called expectable range of emotions and behaviors in response to life's ongoing challenges and upheavals—provides the foundation upon which psychiatric classification and diagnoses rest. With little firm knowledge about what constitutes the normal range of reaction to adversity, structural flaws likely exist in the definitional underpinnings of psychopathology in general and of MDD in particular (Monroe et al., 2009). Distinguishing between psychological distress as an expectable response to adversity and distress that is a manifestation of clinical depression represents a significant challenge for depression research. It is a challenge, too, that points to new roles life stress may play in improving our understanding of the disorder.
Prior to the 1980s and the development of our currently accepted diagnostic systems (e.g., DSM-IV-TR; APA, 2000), clinical depression was diagnosed when the severity of the syndrome was disproportionate (in intensity or duration) to the degree of stress evident in the person's life (Horwitz & Wakefield, 2007). To enhance diagnostic inter-rater reliability, etiological presumptions were discarded and focus shifted toward documenting the presence or absence of key signs and symptoms of depression (see Box 1). While this decision removed unwanted variability in clinical diagnoses, it inadvertently may have introduced unnecessary variability into the category of MDD.
Today, investigators of diverse backgrounds and theoretical persuasions recognize that the emergent category of MDD represents a heterogeneous assortment of conditions and syndromes (e.g., van Praag et al., 2004). One major source of heterogeneity concerns diagnostic challenges in distinguishing between situational crises, short-term adjustment disorders, and long-term clinical depression. Recently, it has been proposed that normal distress responses to acute life stress and adjustment disorders have commonly resulted in improper diagnoses of MDD in clinical populations (i.e., the “false positive” problem with diagnoses of major depression; Horwitz & Wakefield, 2007). Moreover, since mental health researchers have begun to evaluate depression in nonclinical and community samples, concerns about possible false-positive diagnoses of MDD may be especially relevant for accurately estimating the prevalence of MDD and evaluating treatment needs.
To address these recently voiced diagnostic concerns, the signs and symptoms of depression will have to be examined within the context of the individual's life in future research and practice. Without a proper assessment of life stress, one cannot determine whether or not the presenting condition represents an understandable response to adversity, an adjustment disorder, or a clinical syndrome indicative of a true psychological disorder (Horwitz & Wakefield, 2007). In the coming years, life-stress research not only will continue to elucidate depression's origins but also may assist in delineating depression's boundaries relative to nonpathological mood states and conditions.
Overall, the theoretical and empirical mandate to consider life stress in research on major depression is becoming more diversified and complex. Evaluating how life's demands and disasters are capable of provoking a range of psychological responses, including severe psychopathology, will necessitate a more careful consideration and assessment of life stress. In its absence, presence, and gradations in between, life stress represents an essential topic and instrument for investigating the mysteries of major depression.