
Abstract
The loss of a loved one carries serious consequences for the physical and emotional well-being of many of the bereaved. It is therefore not surprising that to mitigate the impact of loss and promote successful adaptation, various forms of grief therapy have been proposed. However, controversies about the effectiveness of bereavement interventions have arisen, in part because previous reviews have relied on small samples of studies, which makes drawing inferences about the evidence base for bereavement interventions precarious at best. Drawing on a recent comprehensive analysis of over 60 controlled studies, we attempt to offer a more definitive view, and we discuss moderators associated with more effective bereavement interventions. Finally, we conclude by considering several theoretically informed approaches that hold promise for the further refinement of evidence-based therapies for bereavement complications, and we suggest some future directions for grief research and intervention.
Bereavement may be distinguished among all major life-event stressors not only by its near inevitability but also by the high likelihood that we will experience it repeatedly across the course of a normal life span. Although most people respond to loss in a resilient fashion, experiencing only transitory distress, or follow an adaptive course of adjustment, beginning to recover baseline levels of functioning following several months, longitudinal research documents substantial and sustained bereavement-related difficulties for many people (Bonanno, Wortman, & Nesse, 2004). Most worrisome is recent evidence that 10 to 15% of the bereaved struggle to adapt to their loss over a period of many months or years. Mourners who experience such complicated or prolonged grief reactions are characterized by intense and persistent yearning for the deceased, intrusive and troubling thoughts regarding the death, a sense of inner emptiness and hopelessness about the future, trouble accepting the reality of the loss, and various other difficulties moving on with life (Lichtenthal, Cruess, & Prigerson, 2004). When left untreated, such symptoms have been shown to increase vulnerability to functional impairment, high blood pressure, cardiac events, substance abuse, and suicidal ideation over the long term (Prigerson et al., in press).
In view of the potentially profound and prolonged impact of bereavement, it is not surprising that helping professionals have stepped forward to assist grieving people. But how effective are these services? Are there features of the bereaved, or of the losses they suffer, that can inform us about who will most benefit from interventions? Are there certain symptoms and problems with which services are more effective? And are there aspects of grief therapy itself—in terms of its timing, duration, structure, or format—that that are likely to be more helpful for those to whom it is offered?
Here we will consider these questions in light of our recent comprehensive review of the literature on bereavement interventions (Currier, Neimeyer, & Berman, 2008) and then follow with a few thoughts on promising developments in grief therapy and associated research.
DOES GRIEF THERAPY WORK—YET?
Previous reviews using both narrative (Forte, Hill, Pazder, & Feudtner, 2004; Schut, Stroebe, van den Bout, & Terheggen, 2001) and quantitative procedures (Allumbaugh & Hoyt, 1999; Kato & Mann, 1999) have summarized what is known about the efficacy of bereavement interventions, reaching conclusions that range from skepticism to cautious endorsement. To provide a clearer and more comprehensive view of the state of the science, we conducted a meta-analysis of all available controlled outcome research on grief therapies (Currier et al., 2008), which involved using statistical procedures to convey the big picture about its effectiveness and to examine factors associated with greater or lesser benefit. The review was based on 61 outcome studies, which included 48 published peer-reviewed articles and 16 unpublished dissertations, making it the most comprehensive summary of the literature currently available. We used several criteria to select studies, the most basic of which was that the therapy tested aimed to improve bereavement adaptation and that the study included a group of bereaved persons who did not receive any formal help (that is, a no-intervention control group). Although most studies adhered to the gold standard of random assignment to treatment or control conditions, we also included 14 studies that did not do so, and we analyzed these separately to see if similar trends held in random and nonrandom studies.
We had two distinct but interrelated aims for the review. Primarily, we were concerned with evaluating the overall effectiveness of grief therapies and exploring commonalities among the studies that generated better (and worse) outcomes. These features that potentially could moderate the outcomes achieved included the targeted population, timing of intervention, method of recruiting bereaved persons, a series of person- (e.g., age, sex) and loss-related factors (e.g., cause of death, relationship to the deceased), and features of the interventions themselves (e.g., number of sessions, group versus individual format). Secondarily, we assessed the amount of change over time among intervention recipients and participants in the control groups. This allowed us to address issues that we could not explore by simply relying on the standardized differences between intervention and control groups at a particular time point. For example, discouraging outcomes discussed in prior reviews might have been the result of either deterioration among intervention recipients or of improved adjustment among those who did not receive formal help. Clearly, these different patterns would carry quite different implications for interventionists in the trenches.
Our efforts to identify as many available studies as possible yielded a long line of research conducted over the past 3 decades. The age of the participants in the studies ranged from childhood through later life. As is consonant with trends in bereavement research in general, three out of four participants were female and Caucasian, and the same percentage had lost an immediate family member (i.e., spouse, parent, child, or sibling), with over a quarter of these losses occurring by homicide, suicide, or a fatal accident. On average, interventions were administered 14 months following the loved one's death. Most of the interventions used a group modality, although individual and family approaches were represented as well. The types of interventions included psychotherapy and counseling, professionally organized support groups, crisis intervention, social activities groups, writing therapy, a formal widowed-persons visiting service, and a helper training program. Although the therapies were based on several different theoretical models, their common focus on grief led many of them to focus on separation distress triggered by the loss and to provide support and problem solving for how to adapt to a changed life. The mean number of sessions for the interventions was eight, indicating the time-limited nature of most of the therapies tested to date.
WHAT WE FOUND
Consistent with the majority of smaller-scale reviews, our tests of overall effectiveness failed to yield an overly encouraging picture of grief therapies (see Fig. 1). Of the overall analyses, grief therapies did outperform no-intervention control conditions immediately following the intervention in the randomized and nonrandom studies, although these effects were only weak to moderate. However, analyses for follow-up outcomes at an average of 8 months later failed to yield intervention effects significantly greater than zero. These results contrast with meta-analyses of general psychotherapy for other forms of distress, which typically yield large effects by the end of treatment and show enduring improvement (Wampold, 2001). However, beyond this general conclusion, other analyses revealed that some treatments showed little benefit or even negative effects, whereas other therapies enjoyed impressive effectiveness. This highlighted the need to subdivide the studies on the basis of clinically relevant factors that could account for different results.
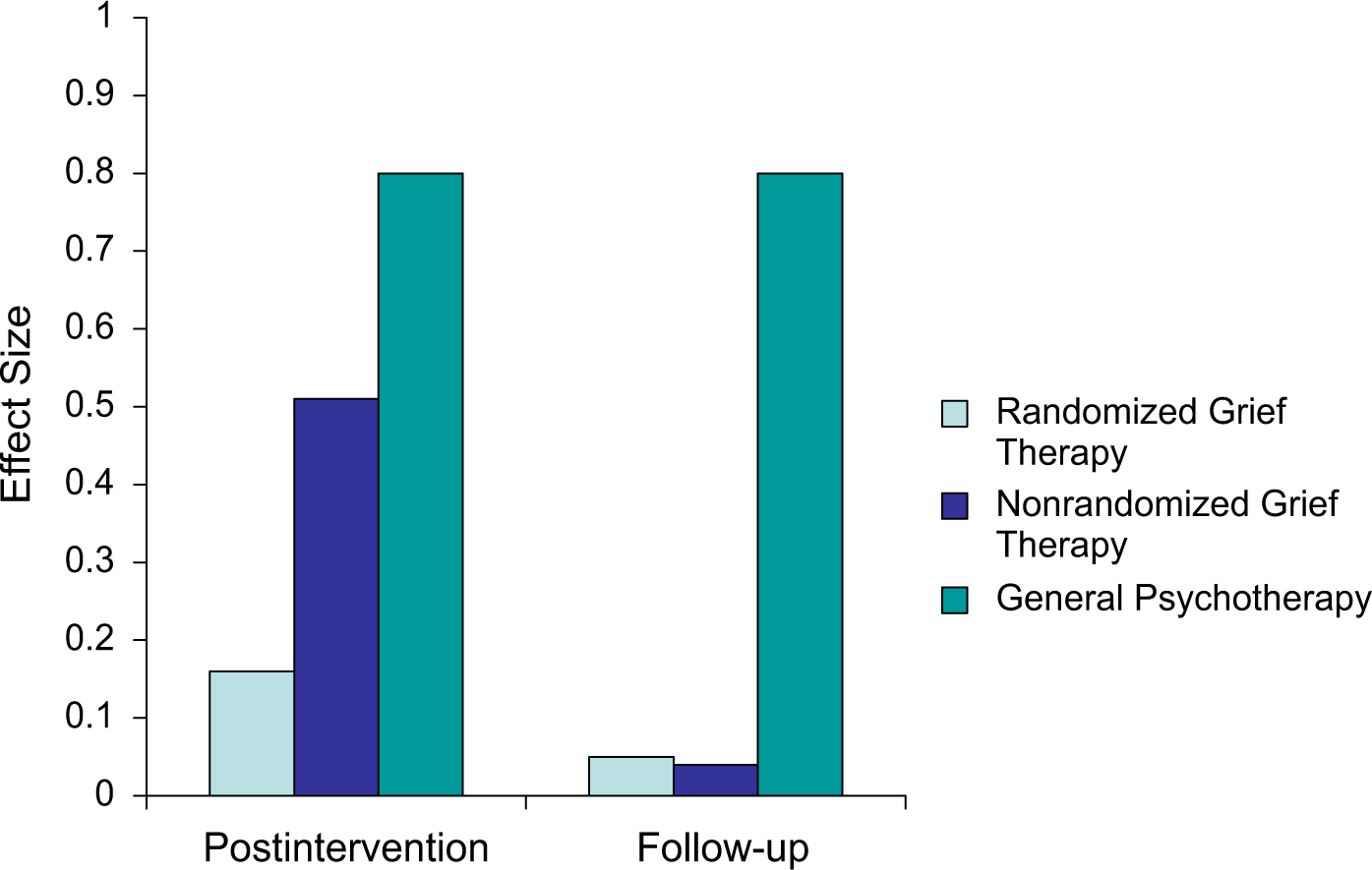
Overall effectiveness of grief therapies compared to general psychotherapy. Bars represent effect sizes for different classes of interventions relative to untreated controls, with taller bars indicating more effective treatments. Compared to general psychotherapy for other problems (see Wampold, 2001), the effects of grief therapy are unimpressive; the apparently more substantial effects for nonrandom studies of grief therapy likely reflect confounding factors, such as the assignment of more motivated clients to the active treatment condition.
WHO DO WE HELP? THE SEARCH FOR MODERATORS
Of the many potential moderators we explored, the targeted population emerged as especially critical for researchers and clinicians to consider in their work (see Fig. 2). Using contemporary Institute of Medicine nomenclature, we compared universal applications targeting anyone who suffered a loss, selective interventions with subsets of higher-risk grievers (such as parents who lost children to violent death), and indicated interventions that took the further step to assess for difficulties adapting to loss as a requirement for treatment (as in evaluating the presence of complicated grief )—broadly paralleling the distinctions between primary, secondary, and tertiary prevention used by previous reviewers (Schut et al., 2001). Like these reviewers, we found that universal interventions failed to produce better outcomes than would be expected by the passage of time. By comparison, although selective interventions showed a small benefit at posttreatment, these benefits were not significant at follow-up. In contrast, outcomes of indicated interventions were clearly favorable and showed enduring improvement for survivors, a factor that could not be attributed to regression to the mean in those with severe symptoms because they showed more substantial change than control-group respondents, who did not receive the intervention, over the same period of time. In other words, for treating those struggling with intense symptomatology over a protracted period, grief therapy is an evidence-based practice that enjoys growing support.
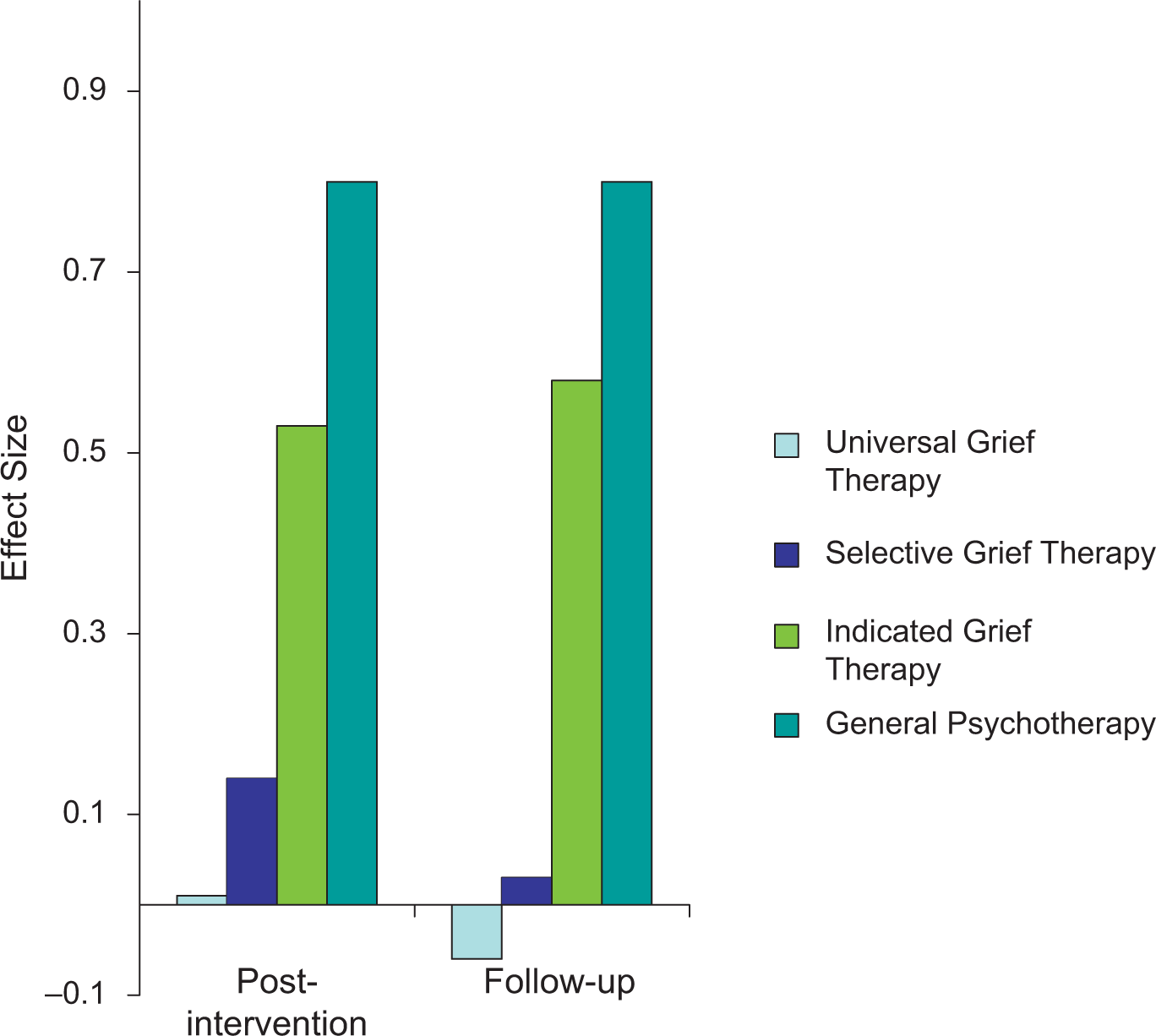
Effect sizes of grief therapies for targeted populations. At both posttreatment and follow-up, bereavement interventions for “indicated” groups of mourners suffering from clinically elevated symptoms outperform interventions for “selective” groups of “at risk” mourners (e.g., bereaved parents) and “universal” interventions for all bereaved people, regardless of risk or demonstrated distress. Effects for general psychotherapy for other problems (see Wampold, 2001) are included for comparison.
Somewhat to our surprise, however, none of the remaining potential moderators reliably accounted for differences in outcome: Similar results were found for men and women, children and adults, and regardless of the relationship one had to the deceased. We also found that the timing of the intervention had little relation to outcome, overturning conclusions of earlier reviews that had suggested early intervention was important. Similarly, the source of referral made a difference only at post-treatment, at which time studies intervening with referred clients generated better outcomes than those strictly relying on aggressive outreach procedures. This advantage faded in the coming months, however—again qualifying the conclusions of earlier reviewers (Schut et al., 2001).
Examining patterns of change in control groups over time, we discovered no evidence that the average untreated survivor deteriorated. Instead, on average, all of the groups displayed positive change at posttreatment and follow-up, so that favorable intervention effects, when these were observed, resulted from greater reductions in distress in intervention recipients than in those who went without formal help. Viewed affirmatively, these results suggest that grief therapy can be helpful to a range of people contending with a range of losses, ameliorating many forms of distress in the near and long-term aftermath of bereavement, regardless of how they enter therapy, if they are assessed as contending with substantial clinical distress to begin with. Others with less oppressive and sustained symptoms tend to respond resiliently, even in the absence of intervention, suggesting that grief therapists might adopt an attitude of humble appreciation for what many of the bereaved can achieve without professional assistance.
THE FUTURE HORIZON
Taken together, the findings of our review reinforce the need for more research to establish and extend the efficacy of carefully crafted therapies for the subset of the bereaved who struggle to move forward with their lives after loss. Fortunately, such theory-guided research is now being undertaken. For example, one controlled study of a specially tailored complicated grief treatment (CGT) was guided by the dual-process model of bereavement (Stroebe & Schut, 1999), which posits that adaptation after the death of a loved one entails oscillating between orientation to the loss (as through expressing and exploring the grief and reconnecting with the memory of the loved one) and restoration of contact with a changed world (as through re-engaging relationships and work and experimenting with new life roles). Accordingly, CGT involves a series of specific procedures for accomplishing these tasks, ranging from revisiting the story of the loss in its most painful aspects to holding facilitated conversations with the image of the loved one, to creating opportunities to reorganize future goals. Impressively, such therapy produces substantial change across 16 weeks of treatment for over half of those with debilitating grief—roughly twice the rate of improvement for similar patients randomly assigned to a more general form of psychotherapy (Shear, Frank, Houch, & Reynolds, 2005). Other effective therapies use written (Wagner, Knaevelsrud, & Maercker, 2006) or oral procedures (Boelen, de Keijser, van den Hout, & van den Bout, 2007) to promote adaptation to the story of loss and to promote more constructive thinking about it, both of which have outperformed control conditions. Common components of such evidence-based interventions include (a) the selection of grievers who display intense and prolonged separation distress and related complications in the aftermath of loss; (b) repeated and experientially intense “retelling” of the circumstances of the death with associated feelings and reactions, often coupled with prompts for the client to take perspective on it in a healing way; (c) some form of guided encounter with the memory of the loved one, as in a symbolic monologue or dialogue with the deceased or through drafting letters to them; and (d) attempts to promote “restoration oriented” coping such as attending to current relationships and responsibilities and projecting new goals that better fit with the new post-loss reality.
A recent quantitative review of therapies that incorporate these and similar cognitive-behavioral procedures documents their efficacy relative to no treatment but calls into question their differential effectiveness relative to supportive therapies once investigator allegiance is taken into account (Currier, Holland, & Neimeyer, in press). Such findings provide encouragement that focusing not only on emotion regulation but also on dealing with traumatic imagery associated with the loss, countering fatalistic thinking and hopelessness, and addressing practical readjustments in life can all play a role in promoting adaptation, but they leave room for exploration of factors that could contribute to the further refinement of grief theory and therapy.
Several recent theories in addition to the dual-process model (Stroebe & Schut, 1999) mentioned above could provide guidance in this project. One is the cognitive-behavioral formulation of complicated grief, which argues that bereaved people who struggle with accommodating the loss face specific problems in integrating the death of their loved one into their autobiographical memory, as well as in contending with unrealistically negative and self-blaming patterns of thinking in its aftermath (Boelen, van den Hout, & van den Bout, 2006). Research on an intervention drawing on this rationale suggests that the former emphasis on coming to terms with the loss may be a primary consideration, with challenging distorted patterns of thinking playing a secondary role in most cases (Boelen et al., 2007). A second promising framework is the two-track model of bereavement, which posits that adaptation to loss proceeds along two avenues simultaneously: a biopsychosocial track reflecting the bereaved person's overt symptomatology (e.g., grief, depression, anxiety, social and occupational disruption) and a relational track reflecting his or her pre- and post-death relationship with the deceased (e.g., how the loved one is held in memory, idealized, and incorporated into the bereaved person's ongoing life). Research on this model and the modification of these factors in therapy is likely to benefit from the recent development of a valid measure of its central constructs (Rubin, Malkinson, Koren, & Michaeli, in press).
Finally, a constructivist theory of bereavement posits that grieving entails an active effort to reaffirm or reconstruct a world of meaning that has been challenged by loss (Neimeyer, 2006). In this perspective, people are viewed as meaning makers, drawing on personal and cultural resources to construct a system of beliefs that permit them to anticipate and respond to the essential events of their lives. The death of a loved one, however, can challenge this framework, sometimes calling into question the coherence of a person's worldview and self-narrative, or life story, across time. Such a perspective accords well with a growing body of research that points to the anguished search for meaning into which bereaved parents (Keesee, Currier, & Neimeyer, 2008) and survivors of the violent death of a loved one (Currier, Holland, & Neimeyer, 2006) are frequently cast, and the tendency for enhanced sense making in the wake of such tragic losses to be associated with more favorable bereavement outcomes. As more evidence accrues regarding the role of these cognitive, attachment-oriented, and meaning-making processes in adjustment to bereavement, we are hopeful that such theory-based models will contribute to an expanded toolbox of effective methods for grief therapists.
Footnotes
Recommended Reading
Boelen, P.A., de Keijser, J., van den Hout, M., & van den Bout, J. (2007). (See ![]() ). A representative controlled study of grief therapy supporting its effectiveness.
). A representative controlled study of grief therapy supporting its effectiveness.
Calhoun, L., & Tedeschi, R.G. (Eds.). (2006). Handbook of posttraumatic growth. Mahwah, NJ: Erlbaum. A volume containing several readable and empirically informed contributions to research on the development of strength and resilience in the face of tragic and challenging life circumstances.
Center for the Advancement of Health. (2004). Report on bereavement and grief research. Death Studies, 28, 489–575. Summarizes recent developments in bereavement theory and research, with an emphasis on health impacts.
Neimeyer, R.A. (Ed.). (2001). Meaning reconstruction and the experience of loss. Washington, DC: American Psychological Association. Presents a multifaceted exploration of meaning-oriented research, theory and practice on bereavement and grief therapy.
Stroebe, M., Hansson, R., Schut, H., & Stroebe, W. (Eds.). (2007). Handbook of bereavement research and practice. Washington, DC: American Psychological Association. Offers a multifaceted survey of contemporary research on grief, with a focus on major theories and research programs concerning bereavement-related coping, social support, neurobiological dimensions, and more.