
Abstract
A massive literature documents the inverse association between poverty or low socioeconomic status and health, but little is known about the mechanisms underlying this robust relation. We examined longitudinal relations between duration of poverty exposure since birth, cumulative risk exposure, and physiological stress in two hundred seven 13-year-olds. Chronic stress was assessed by basal blood pressure and overnight cortisol levels; stress regulation was assessed by cardiovascular reactivity to a standard acute stressor and recovery after exposure to this stressor. Cumulative risk exposure was measured by multiple physical (e.g., substandard housing) and social (e.g., family turmoil) risk factors. The greater the number of years spent living in poverty, the more elevated was overnight cortisol and the more dysregulated was the cardiovascular response (i.e., muted reactivity). Cardiovascular recovery was not affected by duration of poverty exposure. Unlike the duration of poverty exposure, concurrent poverty (i.e., during adolescence) did not affect these physiological stress outcomes. The effects of childhood poverty on stress dysregulation are largely explained by cumulative risk exposure accompanying childhood poverty.
Poverty during early childhood is associated with increased morbidity and decreased life span in adulthood (Blane, Bartley, & Davey-Smith, 1997; Lawlor, Ronalds, Macintyre, Clark, & Leon, 2006). This association occurs irrespective of adults' social status (Kuh, Hardy, Langenberg, Richards, & Wadsworth, 2002; Poulton et al., 2002). Something in the early life experiences of low-income individuals sets them on a life trajectory of impaired health. Our focus in this article is on why this occurs. We suggest that poverty in early childhood harms health because stress regulatory mechanisms are damaged by excessive exposure to cumulative environmental risks during childhood. We tested this hypothesis by examining neuroendocrine and cardiovascular markers of stress regulation and cumulative physical and social risk exposure in a longitudinal sample of low- and middle-income adolescents.
Poverty and low socioeconomic status (SES) are associated with elevated basal measures of blood pressure in children under the age of 13 (Chen, Matthews, & Boyce, 2002). This link between poverty and blood pressure vanishes by adolescence, although it reappears in adulthood (Chen et al., 2002). Two cross-sectional studies also have revealed elevated hypothalamic-pituitary-adrenocortical (HPA) axis activity among low-income, elementary-school-age children (Evans & English, 2002; Lupien, King, Meaney, & McEwen, 2000).
These findings leave open a critical question: Why does poverty in early childhood lead to stress dysregulation? One plausible explanation is that risk exposure may be heightened among poor children relative to more affluent children. Low-income children confront significantly more physical and social risk factors than their wealthier counterparts (Taylor, Repetti, & Seeman, 1997). Income-related physical risks include substandard housing, low neighborhood quality, toxins, ambient pollutants, noise, and crowding (Evans, 2004). Also, the families of poor children tend to have heightened levels of conflict, greater risk of dissolution, and harsher and more unresponsive parenting (Repetti, Taylor, & Seeman, 2002). Research has also shown that several of these physical and social environmental risk factors potentiate physiological stress. Both noise and crowding increase blood pressure and activate the HPA in children (Evans, 2006). Early exposure to family instability, turmoil, and harsh, unresponsive parenting is linked to similar physiological outcomes (Repetti et al., 2002).
Although elevated resting levels of blood pressure and HPA activity are associated with morbidity, recent physiological stress research implicates damage to stress regulation as the principle mechanism underlying disease etiology (McEwen, 1998; 2000). Thus, we hypothesized that the effect of childhood poverty on subsequent health is due to elevated HPA activity plus reduced efficiency of the cardiovascular response to stress. We examined the efficiency of stress regulation by assessing blood pressure reactivity and recovery after exposure to an acute stressor. Given the epidemiological literature, however, we expected no effects of poverty on sympathetic activation in young adolescents (Chen et al., 2002). Moreover, we expected the adverse effects of childhood poverty on stress regulatory mechanisms to be mediated by elevated cumulative risk exposure.
METHOD
Participants
Two hundred seven young adolescents (M = 13.4 years; 52% male) who had complete physiological data in the second wave of a longitudinal study (M = 9.2 years at Wave 1) were included in the sample. At initial recruitment, 53% of the sample lived at or below the federal poverty line. The sample was Caucasian, and all the children resided in rural areas of upstate New York. (See Evans, 2003, for further details on the sample and the procedures for data collection.)
Each youth and his or her mother were tested independently by two trained interviewers in the home. A standard protocol was used to collect sociodemographic information, data on risk exposure, a host of questionnaire and behavioral indices of socioemotional development, and physiological stress indicators.
Measures
Poverty
The duration of lifetime exposure to poverty was defined as the proportion of years each adolescent had lived in poverty since birth. Poverty was operationalized as an income-to-needs ratio of less than or equal to 1.0. This ratio is an annually adjusted, per capita index of income that the U.S. Census Bureau calculates using a standardized formula.
Physiological Stress
Twelve-hour, overnight urinary free cortisol was calculated by a radioimmune assay at both Wave 1 and Wave 2 (Contreras, Hane, & Tyrrell, 1986). Creatinine was also measured to control for differences in body size and incomplete voiding (Tietz, 1976). We also assayed overnight urinary catecholamines; we do not discuss these data here, however, because urinary catecholamines are indices of sympathetic activation, which does not show effects of poverty in adolescents.
At both waves, basal blood pressure was monitored (Dinamap Pro 100, Tampa, FL) every 2 min over a 14-min period while the youth sat quietly and read. The mean of the second through seventh readings was used as the index of basal blood pressure (Kamarck et al., 1992), which was not expected to be related to exposure to poverty. Cardiovascular reactivity and recovery were measured at Wave 2 only. Immediately following the seventh reading, the youth was told without warning that he or she would now take a math test. The task was to mentally subtract a two-digit number from a series of four-digit numbers without writing down any calculations. Every 4 min, the two-digit number was changed. This reactivity phase lasted for 12 min, with blood pressure monitored every 2 min. Thirty seconds after the test was completed, the first of five additional readings (at 2-min intervals) was taken while the youth again sat quietly and read for a period of 10 min. This constituted the recovery phase of the protocol. At the end of the test, the participant was assured that no more tests would be given, and that he or she could relax and read while the blood pressure monitoring continued. Mental arithmetic is a standard stress-induction protocol used in reactivity studies with children and adults (Gump & Matthews, 1999; Matthews, Gump, Block, & Allen, 1997).
Cumulative Risk Exposure
Cumulative risk was calculated from birth to the initial wave of data collection and for the time interval between Wave 1 and Wave 2. The six risk factors included three physical risks, crowding (people/room), noise (average decibel level in the home over a 2-hr period), and substandard housing (assessed using a standardized, rater-based instrument; Evans, Wells, Chan, & Saltzman, 2000), and three social risks, family turmoil, child's separation from parents, and exposure to violence. At Wave 1, exposure to social risks was determined from mothers' reports on the Life Events and Circumstances (LEC) checklist (Work, Cowen, Parker, & Wyman, 1990); at Wave 2, youths' self-reports on the Adolescent Perceived Events Scale (Compas, 1997) were also included (an event was counted a single time if it was reported by the youth, the mother, or both). Multiple items (yes/no) made up each social risk factor. Exposure to physical risks was calculated identically at each wave of data collection.
For each of the six individual risk domains, risk was coded dichotomously at each wave. A score of 1 was given if the youth's exposure at a given wave was more than 1 standard deviation above the mean for the entire sample's distribution of continuous exposure at that wave, and a score of 0 was given in all other cases. Cumulative risk exposure (0–6) was then calculated for each wave of data collection by summing across the six singular risk factors.
RESULTS
Data-Analytic Strategy
Ordinary least squares regression was employed to analyze how the duration of lifetime exposure to poverty was related to cortisol levels, baseline blood pressure, and cardiovascular reactivity assessed in early adolescence in Wave 2 of this longitudinal study. Cardiovascular reactivity was operationalized by subtracting the mean of the six baseline readings from the mean of the six readings during the acute stressor. Recovery was analyzed with multilevel, hierarchical linear modeling (Singer & Willett, 2003). For overnight cortisol, prior cortisol levels, assessed at age 8, were included in the model. For the reactivity and recovery indices, no prior physiological data were available; thus, these analyses are cross-sectional. To examine the hypothesized mediational role of cumulative risk exposure, we repeated each of the regression equations with two additional terms in the model, Wave 1 and Wave 2 cumulative risk. The change in the b weight for poverty between the first regression model (cumulative risk not included) and the second regression model (cumulative risk included) was the prime indicator of mediation.
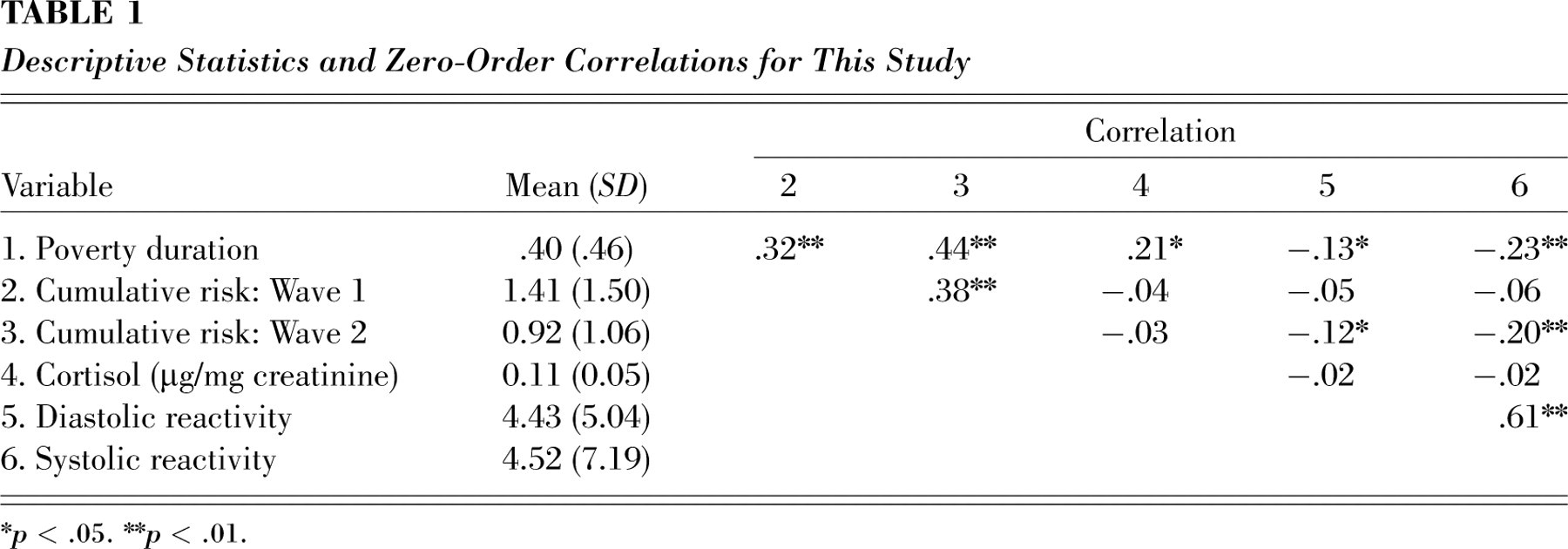
Table 1 displays descriptive information and the zero-order correlation matrix for duration of poverty exposure, cumulative risk, and the physiological stress measures.
Descriptive Statistics and Zero-Order Correlations for This Study
∗ p < .05.
∗∗ p < .01.
Chronic Physiological Stress
Overnight urinary free cortisol (controlling for Wave 1 cortisol) was significantly elevated by longer duration of exposure to poverty in childhood, b = 0.02 (SE = 0.01), p < .01, p rep = .97, f 2 = .05. As expected, adolescents' basal blood pressure, controlling for Wave 1 levels, was unaffected by exposure to poverty. To examine whether the effects of poverty duration on chronic physiological stress were mediated by cumulative risk exposure, we initially examined whether duration of poverty was related to the hypothetical mediator, cumulative risk exposure. Duration of poverty was significantly related to cumulative risk exposure at Wave 1, b = 0.80 (SE = 0.16), p < .001, p rep = 1.00, f 2 = .11, and at Wave 2, b = 1.05 (SE = 0.14), p < .001, p rep = 1.00, f 2 = .25. We next examined whether the significant relation between poverty duration and overnight cortisol was attenuated when cumulative risk was included in the equation. Contrary to our hypothesis, the covariance between poverty duration and elevated cortisol was not affected by the inclusion of the mediator, cumulative risk, in the regression model, b = 0.02.
Stress Regulation
The greater the duration of exposure to poverty, the less robust was the response to the acute stressor. Both diastolic and systolic blood pressure reactivity were significantly lower for children who had spent a greater proportion of their lives in poverty, b = −1.62 (SE = 0.77), p < .03, p rep = .90, f 2= .02, and b = −3.62 (SE = 1.05), p < .01, p rep = .99, f 2 = .06, respectively. The effects of duration of poverty exposure on diastolic and systolic blood pressure recovery were not significant. The significant relations between duration of poverty and cardiovascular reactivity became nonsignificant when the effects of cumulative risk were partialed out of each equation, b diastolic = −1.06, b systolic = −2.75.
Timing of Poverty Exposure
Because of the longitudinal nature of our research design, we could also examine whether the chronic effects of poverty duration on stress dysregulation were largely due to exposure to poverty at the time of Wave 2 assessment. They were not. Poverty at Wave 2 had no significant effects on any of the measures of stress dysregulation. Moreover, the significant impacts of poverty duration on cortisol and cardiovascular reactivity all remained statistically significant when poverty at Wave 2 was added to the equation.
DISCUSSION
In this sample of young adolescents, the greater the proportion of their lives they had spent living in poverty, the higher their levels of chronic HPA activity. These are the only prospective, longitudinal data on poverty and physiological stress, and they replicate two prior cross-sectional studies of childhood poverty and HPA activity (Evans & English, 2002; Lupien et al., 2000). Also, for the first time, we have shown that poverty during childhood is linked to a dysregulated stress response to an acute stressor. The more time 13-year-old children have spent living in poverty since birth, the more muted their cardiovascular reactivity to a standard acute-stressor protocol. Although we had also expected to see a less efficient (i.e., slower) pattern of cardiovascular recovery among chronically poorer children following cessation of the acute stressor, we did not. One reason for this result might be the significantly lower level of reactivity in the children with greater exposure to poverty. Another possibility is that chronically impoverished children have an elevated degree of variability during the recovery period. The pattern of chronically elevated cortisol coupled with muted reactivity to an acute stressor is indicative of damage to stress regulatory mechanisms that portends long-term morbidity (McEwen, 1998; 2000). The finding that these results are due to chronic poverty exposure rather than concurrent poverty exposure during adolescence is important as well. Many epidemiological studies have uncovered little or no relation between poverty and blood pressure among adolescents (Chen et al., 2002).
Our results also provide longitudinal evidence that some of the apparent ill effects of childhood poverty on stress regulation are due to elevated cumulative risk exposure. These longitudinal data on poverty and cumulative risk exposure extend the results of prior cross-sectional studies showing elevated exposure to single physical and social risks among low-income children (Repetti et al., 2002; Taylor et al., 1997). Moreover, we have demonstrated that elevated cumulative risk exposure during early childhood compromises the ability of the body to handle environmental demands efficiently. One possible reason why cumulative risk exposure had significant mediational effects on cardiovascular reactivity but not on the HPA axis may be found in allostatic-load theory. Elevated HPA activity from chronic stress is viewed as an early marker of allostatic load, whereas alterations in dynamic stress regulation, such as reactivity to an acute stressor, are posited to occur later in the etiology of allostatic load (McEwen, 1998; 2000). It is interesting to note in this regard that the cumulative risk index mediated the effects of poverty on cortisol in this same sample of children at Wave 1, when they were 9 years old (Evans & English, 2002). Unfortunately, dynamic cardiovascular responses were not assessed in the first wave of this study. It is also worth repeating that the well-documented associations between childhood social class and adult morbidity and mortality occur irrespective of adults' social class (Kuh et al., 2002; Poulton et al., 2002). An early history of poverty appears to set children on a life-course trajectory of ill health.
The overall pattern of chronically elevated HPA activity, inefficient cardiovascular mobilization, and elevated cumulative risk exposure accompanying childhood poverty is consistent with the findings of two epidemiological studies of early-childhood risk and adult health. The accumulation of risk factors beginning in childhood (e.g., not owning a home at age 11) related prospectively to self-reported health at age 23 in a national birth cohort in Britain (Power & Matthews, 1998). Felitti et al. (1998) showed that the 10 major causes of adult mortality were associated with retrospective reports of early-childhood risks (e.g., domestic violence). Although these two epidemiological studies and the present results suggest linkages among poverty in early childhood, elevated cumulative risk exposure, and eventual morbidity, more definitive results will require continued prospective tracking of disease outcomes in the present sample as these individuals develop over the life course.
Footnotes
Acknowledgements
We are grateful to the many families who have participated throughout this research and to Jana Cooperman, Kim English, Missy Globerman, Tina Merilees, Chanelle Richardson, Adam Rokhsar, and Amy Schreier for their assistance with data collection. This work has been supported by the W.T. Grant Foundation and the John D. and Catherine T. MacArthur Foundation Network on Socioeconomic Status and Health and by the Virginia F. Cutler, Martha E. Roulk, Flora Rose, and Anna Cora Smith Graduate Fellowships from Cornell University.