
Abstract
Immediately after publication of the ICHD 2nd edition, we developed a computerized, structured medical record based exclusively on the proposed new classification system for primary headaches. This computerized system examines all the diagnoses of primary headaches on the basis of the variables needed to fulfil their mandatory criteria. This is very difficult to obtain in particular cases without having the support of a computerized device.
We tested the computerized structured record by entering and analysing different cases of primary headaches and the corresponding output diagnoses, with particular regard to the new entities introduced: diagnoses of probable migraine with and without aura, probable frequent and infrequent tension-type headache, chronic and probable chronic migraine, and finally, probable tension-type headache.
We would like to bring to your attention two examples, which prompted us to propose some modifications to the new diagnostic criteria. For each case we will provide the input variables (Case 1, Table 1) and output diagnoses (Case 1, Table 2) as well as the fulfilled mandatory criteria.
Input variables for Case 1

The output diagnosis for Case 1
Some considerations are needed when we examine these 2 diagnoses. First of all, the diagnosis to make is surely the certain diagnosis, leaving out the probable diagnosis.
If the output of our computerized sheet does not modify our clinical judgement, it will lead us to consider, also, from a theoretical point of view, the diagnostic criteria of probable infrequent episodic tension-type headache, which are all fulfilled in the case presented above. However, if we look at the days with headache/month (13 days/month for >3 months), our clinical judgement must strongly question the diagnosis of frequent episodic tension-type headache.
The diagnostic criterion A for probable infrequent episodic tension-type headache is, in any case, misleading; it states: ‘Episodes fulfilling all but one of criteria A–D for 2.1 Infrequent episodic tension-type headache’. This means that even criterion A for ‘2.1 Infrequent episodic tension-type headache’ could not be fulfilled. This criterion reports: at least 10 episodes occurring on <1 day per month on average (<12 days per year), and fulfilling criteria B–D for ‘2.1 Infrequent episodic tension-type headache’. No definition of time of observation is given.
According to the definition of probable infrequent tension-type headache, if criterion A in all its components could not be fulfilled, this also implies that the frequency <1 day per month on average, which defines infrequent tension-type headache, could not be satisfied, as is the case described above, in which there are 13 days with headache/month. Theoretically, therefore, it could also be given the diagnosis of probable infrequent tension-type headache.
To avoid this drawback, we therefore propose to change the criteria for infrequent tension-type headache as follows:
bilateral location
pressing/tightening (nonpulsating) quality
mild or moderate intensity
not aggravated by routine physical activity such as walking or climbing stairs
Both of the following:
no nausea or vomiting (anorexia may occur)
no more than one of phonophobia or photophobia
Not attributed to another disorder
Consequently, we propose the following definition of ‘2.4.1 Probable infrequent episodic tension-type headache’:
Episodes do not fulfil criteria for 1.1 Migraine without aura
Not attributed to another disorder
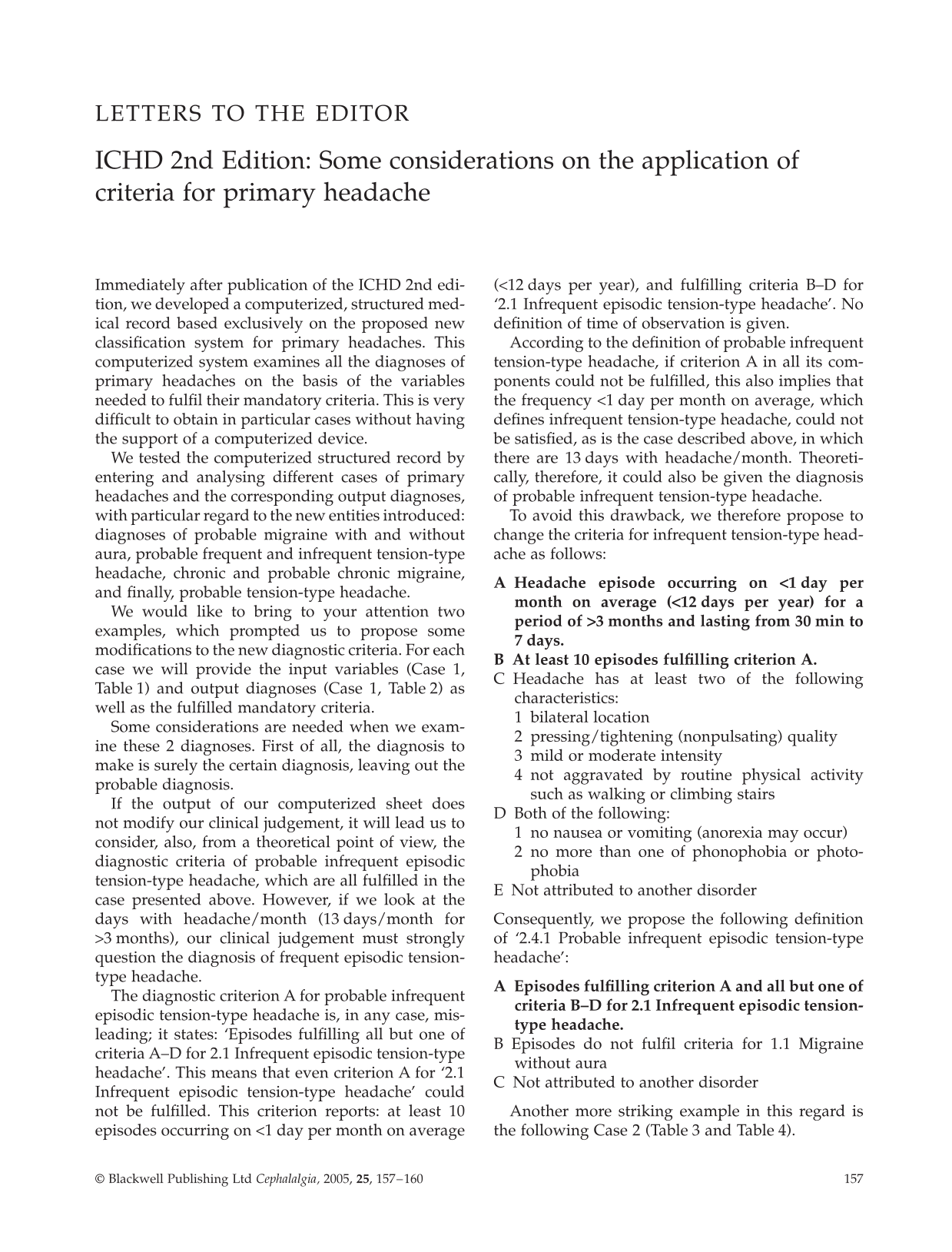
Another more striking example in this regard is the following Case 2 (Table 3 and Table 4).
Input variables for Case 2
The output diagnosis for case 2

In this case we have three probable diagnoses. From a clinical point of view we assume the described cases should be coded as probable frequent episodic tension-type headache, because we have 5 attacks/month with the characteristics of frequent episodic tension-type headache. However, the period of observation is only 2 months, so we also have to consider, from a theoretical point of view, that the criteria of probable infrequent tension-type headache are also fulfilled, because episodes satisfy all but one of criteria A–D for ‘2.1 Infrequent episodic tension-type headache’. To avoid this drawback, we again suggest using the above proposed changed criteria for probable infrequent tension-type headache. According to these modified criteria, the diagnosis of probable infrequent headache will be excluded. It will remain therefore the differential diagnosis between probable episodic tension-type headache and probable migraine without aura. This possibility is considered in the comment to ‘2.4 Probable tension-type headache’. Patients meeting one of these sets of criteria may also meet the criteria for one of the subforms of ‘1.6 Probable migraine’. In such cases, all other available information should be used to decide which of the alternatives is the more likely.
Other suggestions to improve the classification are to avoid the use of ‘for at least 3 months’ instead of ‘≥3 months’ (is this the meaning?) in criterion A of frequent episodic tension-type headache, as well as to avoid the generic definition ‘Headache lasts hours’ or ‘may be continuous’ in criterion B of ‘2.3 Chronic tension-type headache’.
Some questions also arise that are more strictly related to the clinical practice. How should a chronic tension-type headache without medication overuse, which fulfils all but one of criteria B–E, be classified? How should a chronic migraine without medication overuse be classified, which fulfils all but one of criteria C–D for ‘1.1 Migraine without aura’ on ≥15 days/month for >3 months, given that in this as in the previous case, the term probable is exclusively limited to the occurrence of a medication overuse fulfilling criterion B for any of the subforms of ‘8.2 Medication overuse headache’?
In this regard, I would like to bring to your attention the following Case 3 (Table 5, Table 6).
Input variables for Case 3
The output diagnosis for case 3

As you can see, the lack of one of the diagnostic criteria for ‘2.3 Chronic tension-type headache’ leads to the diagnosis of a headache not classified. The situation is also more complicated when chronic tension-type headache and chronic migraine fulfil all but one of criteria C–E for tension-type headache occurring on ≥15 days per month on average for >3 months, or criteria C–D for ‘1.1 Migraine without aura’ on ≥15 days/month for >3 months, respectively, when medication overuse is present.
The validation of the new diagnostic criteria, improved with the aid of a computerized instrument, will help us, in the near future, to answer these and other questions. Comments of those experts who helped elaborate the International Classification of Headache Disorders are warranted. They could surely help us to clarify these unclear points. A debate on this topic is urgent for all those who are trying to apply the new diagnostic criteria, both in the clinical setting and in the research field!