
Abstract

A 27-year-old male patient presented to our hospital with a migraine-like headache, which had begun 8 days earlier with a sudden onset. The pulsating-throbbing pain had an undulating course and reached an intensity of 8/10 on the numeric rating scale (NRS). The maximum was localized at the right forehead spreading subsequently to the entire cranium. The patient complained of nausea, vomiting, aggravation on exertion, photophobia and mild vertigo. He had never before suffered from headache, whereas his father had.
Prior to admission, acetylsalicylic acid had been taken with moderate effect. The past medical history was unremarkable apart from nicotine abuse (10–12 cigarettes/day) and occasional alcohol and cannabis consumption. On examination the vital signs were normal. The patient reported percussion pain over the right frontal sinus and showed a minimally dysmetric finger–nose test bilaterally, moderately impaired tandem gait, and a slight imbalance in Romberg's test with eyes closed. In addition, the nerve exit of the right V1 was painful to pressure. An ECG was normal, while routine lab tests showed an increased total bilirubin (1.12 mg/dl, reference < 1.0 mg/dl) and C-reactive protein (22.6 mg/l, reference < 5 mg/l), which normalized later.
The patient was first treated with 1000 mg paracetamol per day (acetaminophen). As the effect was only moderate, 50 mg sumatriptan was given with a pain reduction from 8 to 2 on the NRS. However, as the pain intensity increased on the next day, 50 mg sumatriptan and later 12.5 mg almotriptan were administered with marked pain relief. At that stage, magnetic resonance imaging of the brain revealed an atypically localized haematoma of the left cerebellum with a diameter of 5 cm (Fig. 1a–c). Digital subtraction angiography of the extra- and intracranial vessels showed a superficially localized arteriovenous malformation in the left cerebellar hemisphere (Fig. 1d).
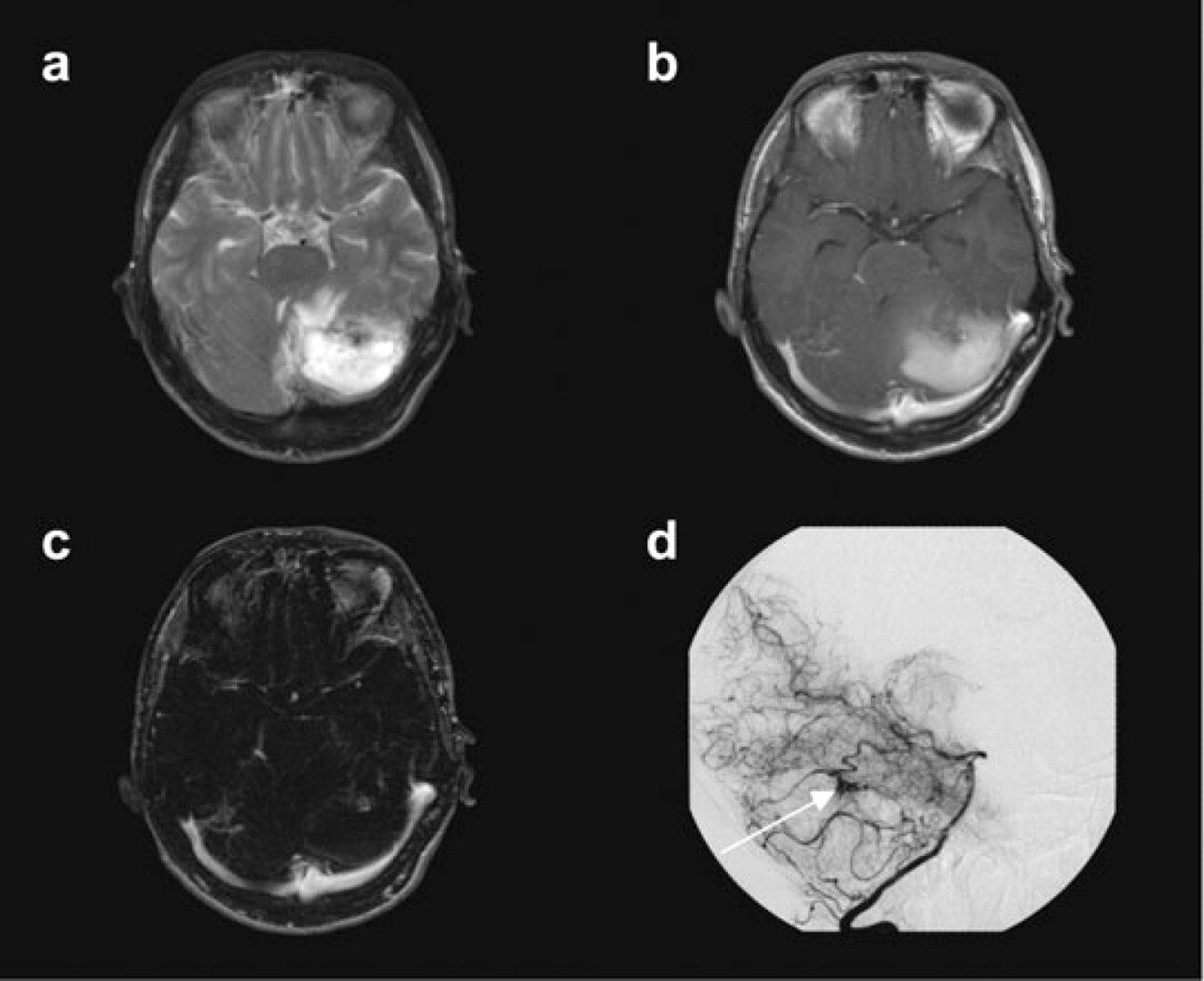
Results of neuroimaging. (a–c) Magnetic resonance imaging of the brain: atypically localized subacute haematoma within the left cerebellum with a diameter of 5 cm and significant impression of the IVth ventricle and mild displacement of the brainstem without signs of a hydrocephalus occlusus (a, T2-weighted image; b, contrast enhanced T1-weighted image; c, subtraction image of T1-weighted image after–before contrast). (d) Digital subtraction angiography of the left vertebral artery: the arrow marks a superficially localized arteriovenous malformation in the left cerebellar hemisphere fed by a branch of the left superior cerebellar artery and draining into the transverse sinus via a cortical vein.
The patient remained conscious and alert all the time and felt generally well. He was transferred to the neurosurgical department for surgical treatment on the next working day, as he was deemed ineligible for an endovascular embolization. Despite comprehensive information about the increased risk of rebleeding, the patient did not wish any intervention and left the hospital on his own responsibility. After dismissal, he was unfortunately lost to follow-up.
Discussion
Headache as the leading symptom has been reported in cerebellar haemorrhage in up to 86% of patients (1). As symptoms of intracranial haemorrhage comprise nausea and vomiting apart from headache (2), it can be mistaken as migraine.
The posterior fossa is innervated by the upper three cervical roots and the IXth and Xth cranial nerve, whereas the anterior and middle fossas are innervated by the trigeminal nerve (3). Wolff showed in his pioneering work that irritation above the tentorium cerebelli causes frontal headache, whereas an irritation below the tentorium mostly leads to pain in the neck and posterior head and is only rarely frontal (4). Our patient experienced frontotemporal pain and displayed typical migraine-like accompanying symptoms without a previous history of headache.
Many patients with primary headache report occipital hypersensitivity and a march-like shifting of the pain from the neck to the forehead, which can be explained by functional connectivity between the trigeminal and the greater occipital nerve (GON) in animals (5, 6) and in humans (7). Consequently, irritation of the GON can cause pain within the trigeminally innervated areas (8, 9). Ropper and Davis (10) observed mostly retro-orbital pain ipsilateral to occipital haemorrhages, although this has not been reported by others (1, 11).
Explanations of how cerebellar irritation causes a migraine-like headache in a previously headache-free subject range from direct mechanical irritation of the dura mater (due to oedema and haemorrhage) or larger vessels to the development of aseptic meningitis, increase in blood pressure and activation of vascular nerve ends in the torn or ruptured blood vessels (1, 11). However, this would still only explain an altered occipital input into the trigeminocervical complex. Neuroimaging studies show consistently that the brainstem plays a pivotal role in migraine headache (12–14). Since vascular malformations of the brainstem can cause symptomatic migraine (15–17), compression of nociceptive structures in the brainstem could be aetiological in our case, but this seems unlikely, given the anatomical situation. As the majority of cases with cerebrovascular disease and benefit from triptans report a pre-existing migraine, the question arises whether migraine patients are especially prone to develop migraine-like symptomatic headaches. The headache in our case could have been the beginning of a migraine, although unfortunately the patient was lost to follow-up.
Pain relief after triptan intake has been reported in headache due to head and neck cancer (18), lumbar puncture (19) and intravenous immunoglobulins (20). Several patients with response to triptans have been reported, in whom later cerebrovascular complications were diagnosed (21–24). In the literature, four migraine patients have been reported where the headache attacks heralding a subarachnoid haemorrhage responded well to triptans (25, 26).
Although there have been various recommendations for neuroimaging in headache (27–29), the need for immediate neuroimaging has to be evaluated individually. In our patient, two ‘red flags’ were present: new-onset headache and an abnormal neurological examination. Since cerebellar signs have been reported in migraine (30), the pathological results in the neurological examination were (wrongly) interpreted as migraine-associated deficits. Nevertheless, it has to be pointed out that migraine-associated cerebellar signs are rare in clinical practice.
In conclusion, there are several lessons to be learned from our case. First, a response to triptans does allow differentiation between migraine and symptomatic (migraine-like) headache. Second, infratentorial pathology can cause a pain in the first trigeminal branch. Third, new-onset headache with abnormal findings on neurological examination should always prompt immediate neuroimaging, even if the clinical picture is suggestive of migraine. Lastly, migraine patients could be prone to develop migraine-like headache in the presence of an underlying symptomatic origin of their headaches more easily than subjects not suffering from primary headache.