
Abstract

Migraine pathophysiology remains incompletely understood. However, migraine symptoms imply involvement of multiple anatomical structures. The trigeminal nucleus caudalis and the ventro-postero-medial nucleus of thalamus convey afferent pain signals from cerebral and meningeal blood vessels. The hypothalamus regulates autonomic functions such as carbohydrate craving. The limbic system plays a role in emotional disturbances such as irritability. The reticular activating system possibly regulates sensitization to pain. The cerebral cortex is the site of the hyperexcitability reported in migraine (1). These structures are directly or indirectly connected to the nucleus- and tractus-solitarius (NTS). This nucleus receives visceral sensations from the vagus nerve.
The efficacy of vagus nerve stimulation (VNS) in seizures has been well established. The clinically available stimulator (Cyberonics®) has been used in thousands of patients (2, 3).
The mechanisms by which VNS controls seizures remain hypothetical. Conceptually, the stimulation provokes an activating or inhibiting effect downstream from the NTS: reticular activating system, thalamus, hypothalamus, amygdalo–hippocampal complex and cerebral cortex (2, 4) (Fig. 1).
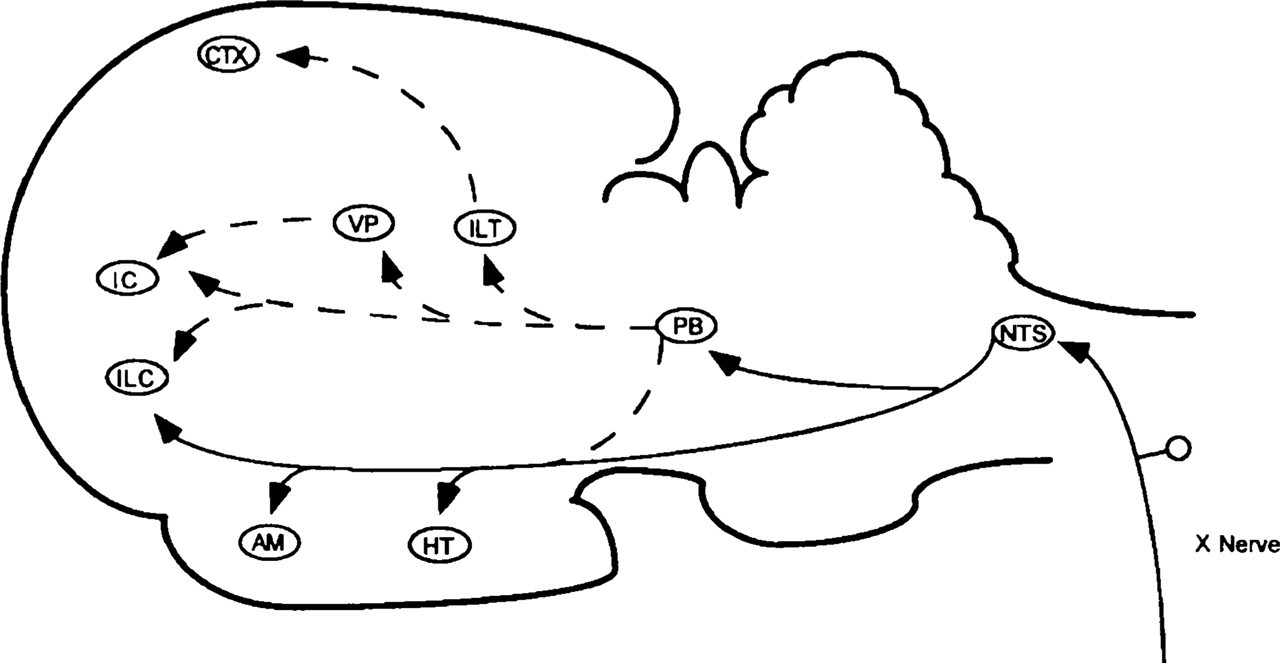
Schematic view of central projections of vagus nerve afferents. NTS, Nucleus and tractus solitarius; PB, parabrachial nucleus; HT, hypothalamus; AM, amygdala; ILC, infralimbic cortex; VP, ventroposterior thalamic complex; IC, insular area; ILT, intralaminar and midline thalamic nuclei; CTX, cerebral cortex (From Schachter et al., with permission (2)).
The NTS projects to the trigeminal nucleus caudalis.
In addition, there have been several reports of the efficacy of VNS in the treatment of experimental pain (5–8). Using the human device Neuro Cybernetic Prosthesis (Cyberonics, Houston, TX, USA), left vagus nerve stimulation in the rat significantly decreased fos-immunoreactivity in trigeminal nucleus caudalis neurons and dramatically reduced nociceptive behaviour induced by ipsilateral formalin injection in the vibrissae (9).
Epidemiological data indicate comorbidity between migraine and epilepsy. This suggests partially common pathophysiological mechanisms (10, 11).
A case series including four patients with migraine indicates a potential benefit on migraine frequency and pain scores and another reports improvement in two chronic migraineurs (12, 13).
Pain in the lower jaw has been reported under certain vagus nerve stimulation parameters, while subsiding under others (14). Finally, a recent report has described a patient whose migraine attacks could be aborted by the activation of his VNS (placed for intractable epilepsy) (15).
Therefore, it was thought that VNS could help reduce the burden of migraine attacks or even abort them. Initial data of the present study have been presented elsewhere (16).
Report of cases
In this context, we set out to investigate whether VNS could prevent migraine.
We performed a retrospective, systematic study of all the patients in our VNS registry of the Neurology Department of Oklahoma University Health Sciences Center (n = 34).
With the local Institutional Review Board approval a questionnaire was sent to all patients. The questionnaire inquired about the presence of headaches, then about their characteristics. The patients were also systematically contacted by telephone by M.E.L. to review and/or complete the questionnaire. This allowed screening for the diagnosis of migraine according to the criteria set forth by the International Headache Society (IHS) (17).
Although the first question inquired about any headache, the count purposefully included only headache attacks that responded to IHS criteria for migraine (17).
The monthly frequency of migraine attacks was established for the following periods: 3 months prior to placement of the device (period I); 3 months following the placement of the device (period II); and the subsequent 3 months (period III). Due to the non-normal distribution of the data, a non-parametric Friedman's test was used for statistical analysis to determine if the median number of headaches per month was different between the time periods, which accounts for the dependence of the observations and the non-normal distribution. Multiple comparisons were then made to determine where the differences occurred.
The response of seizures to treatment was also evaluated and improvement deemed significant if at least 50% reduction in frequency was observed. Period I was compared with periods II and III combined. Finally, the questionnaire also included whether patients suffered from depression and whether this condition subjectively improved on vagus nerve stimulation compared with treatment. As for seizures, period I was compared with periods II and III combined. For statistical analysis of these two parameters, a Sign test was used.
Patients were excluded if adequate information could not be obtained. Patients who suffered from chronic headaches, i.e. occurring > 15 days/month, could not participate. Finally, patients were excluded from analysis if there was a change in their antiepileptic medications.
The Ethics Committee of the University of Oklahoma Health Sciences Center approved the study.
The following results were obtained. Five of the 34 patients in the registry did not answer either by mail or by telephone. Among the 29 remaining patients, four were excluded because of mental retardation. None suffered from chronic headache. There remained 25 patients with adequate information. The delay between the placement of the vagus nerve stimulator and the questionnaire varied (4–36 months, mean 17).
Ten migraineurs were identified (five male, five female; ages 18–36 years) (Fig. 2).

Individual monthly number of attacks for the three study periods, for each of the 10 migraineurs.
Eight (80%) had a reduction of monthly frequency of at least 50%. In these eight patients, improvement occurred in the first 3 months following stimulator placement and was maintained throughout the following 3 months. The median numbers of headache per month (range) were as follows (Table 1): period I: 1.9 (2); period II: 0.5 (2); period III: 0.6 (2). The difference was statistically significant between periods I and II (P < 0.05), between periods I and III (P < 0.05), but not between periods II and III (NS). Five patients became completely headache free. The gender distribution of improvement was even, with four of five women and four of five men improving.
Migraine headache days per period for the entire group
Two of the 10 migraineurs neither improved nor worsened, and there was no difference in attack frequency between the three periods of study.
Mood and/or anxiety disorder was present in six migraine patients, five of whose migraine improved. Among the five patients whose migraine improved, mood/anxiety changes brightened in three (Table 2). These changes were not statistically significant (P = 0.0625).
Relation between change in mood disorder and change in migraine

Among the eight improved migraineurs, seizure frequency improved in four, and among the two non-improved migraineurs, seizures improved in one (Table 3). These changes were not statistically significant (P = 0.25).
Relation between change in seizures and change in migraine

Discussion
These observations suggest that VNS may have a prophylactic effect on migraine.
However, this study has to be interpreted with great caution, for the following reasons. The series is small. The period of study was necessarily short for the following reasons, but represented a compromise. Indeed, on one hand too long a period of study carries the risk of inaccurate recollection, the study being retrospective. On the other hand, because of the natural fluctuation of migraine attack frequency, a minimum length of time is required. It is generally accepted that at least 1 month is necessary to cancel out this effect. The vagus nerve stimulator placement itself may have an unexpected effect on migraine, hence the need for a prolonged postplacement study. Finally, the delay between intervention and questionnaire may add recall bias. Overall, the frequencies of migraine attacks were small, allowing 50% shifts more easily. The comorbidity between migraine and depression could impact on the effect of the device on migraine. However, as seen in Table 2, there does not appear to be a correlation of effect, hence the improvement in migraine is likely to be independent. Likewise, as seen in Table 3, the response of seizures themselves did not seem to have an effect on the change in migraine frequency.
Nevertheless, it seems encouraging to pursue further, larger and more accurate studies. Future possibilities include prospective follow-up of patients, analysis of stimulation parameters, study of a potential abortive effect of vagus nerve stimulation and, of course, larger-scale studies.