
Abstract
STATISTICS AND CLINICAL CHARACTERISTICS
The phenomenon of medication overuse headache (MOH) was first described in 1951. The case was overuse of ergotamine. Patients who took ergotamine on a daily basis developed daily headache and improved significantly after withdrawal of ergotamine. Many terms, such as drug-induced headache and medication misuse headache, have been used to describe this entity. The term medication overuse headache was introduced into the International Headache Society's classification in 2004 (ICHD-II), and a further modification has been made. The new classification defines subforms of MOH according to causal drugs.
Epidemiological studies indicate that the prevalence of chronic headache is about 4–5%, and the prevalence of chronic headache due to overuse of analgesics is about 1%. MOH is a growing worldwide problem in clinical practice. Japan is not an exceptional area, even though specific statistics are scarce. Since studies from other Asian countries have indicated no racial differences in MOH prevalence, Japan seems to have a similar prevalence of MOH.
However, the drugs which cause MOH may vary from country to country, since their availabilities in the market differ, and cultural factors greatly affect people's attitudes. Combination analgesics, which are the major candidates for MOH in the USA and Europe, may contain codeine, barbiturates or caffeine. Neither codeine nor barbiturate is used in combination analgesics in Japan. The introduction of the first triptan to Japan was in 2000, which was much later than in other countries. These differences in circumstances probably affect the profile of the causative drugs of MOH in Japan.
Imai and colleagues have conducted a study to clarify clinical features of MOH in Japan (1). Patients with probable MOH (n = 47) according to ICHD-II were enrolled. They were 41 women and six men, mean age 42.0 years. Of the 47 patients, 38 (80.9%) had migraine only as their primary headache, and two (4.3%) had tension-type headache (TTH) only. Seven patients (14.9%) had both migraine and TTH. The overused medication was combination analgesics in 40 patients (85.1%), analgesics in four (8.5%), ergotamine in one (2.1%), triptans in one, and a combination of acute medications in one patient. The methods of withdrawal used were as follows: abrupt out-patient withdrawal, abrupt in-patient withdrawal, or tapering out-patient withdrawal. Amitriptyline was prescribed daily for management of rebound headache. Fluid replacement, antiemetics and tranquilizers were used to treat withdrawal symptoms. For prophylaxis of migraine, a calcium channel blocker, lomerizine, available only in Japan, was used (2). Triptans were used for migraine attacks. They defined complete resolution of chronic headache and analgesic use on < 10 days/month within 2 months after discontinuation of overused medications as successful withdrawal. According to this definition, 36 patients (76.6%) were successful.
Nagaseki, one of the authors of this communication, and colleagues have reported a large number of MOH patients who had visited his headache clinic. There were 276 MOH patients included (40 men and 236 women, mean age 42.8 years). The age distribution of the MOH patients is shown in Fig. 1. In that study, 201 patients (72.8%) had migraine as the primary headache, including menstrual migraine. Seventy-five patients (27.2%) had other types of headache such as TTH, and headache attributed to somatization disorder (18 patients, 6.5%). One hundred and ninety-nine patients took over-the-counter (OTC) medications, which were mostly combination analgesics containing caffeine. In 184 patients (66.8%) of these, OTC medications were causative drugs for MOH. Thirteen patients (4.7%) overused triptans. The duration of suffering with MOH was from 3 months to 32 years (average 6.5 years). At the end of 3 months after withdrawal treatment started, 78% of patients improved remarkably. They stopped taking medications completely, and their headache improved. Comorbidity with depression was observed in 24.6% of the MOH patients, whereas only 12.9% of migraine patients at their clinic had depression. Nagaseki and colleagues have pointed out that MOH patients have a higher percentage of comorbidity with depression than migraine patients. Some of the MOH patients were prescribed selective 5-HT reuptake inhibitors (SSRI) during withdrawal treatment. The researchers have found use of SSRI to be effective.
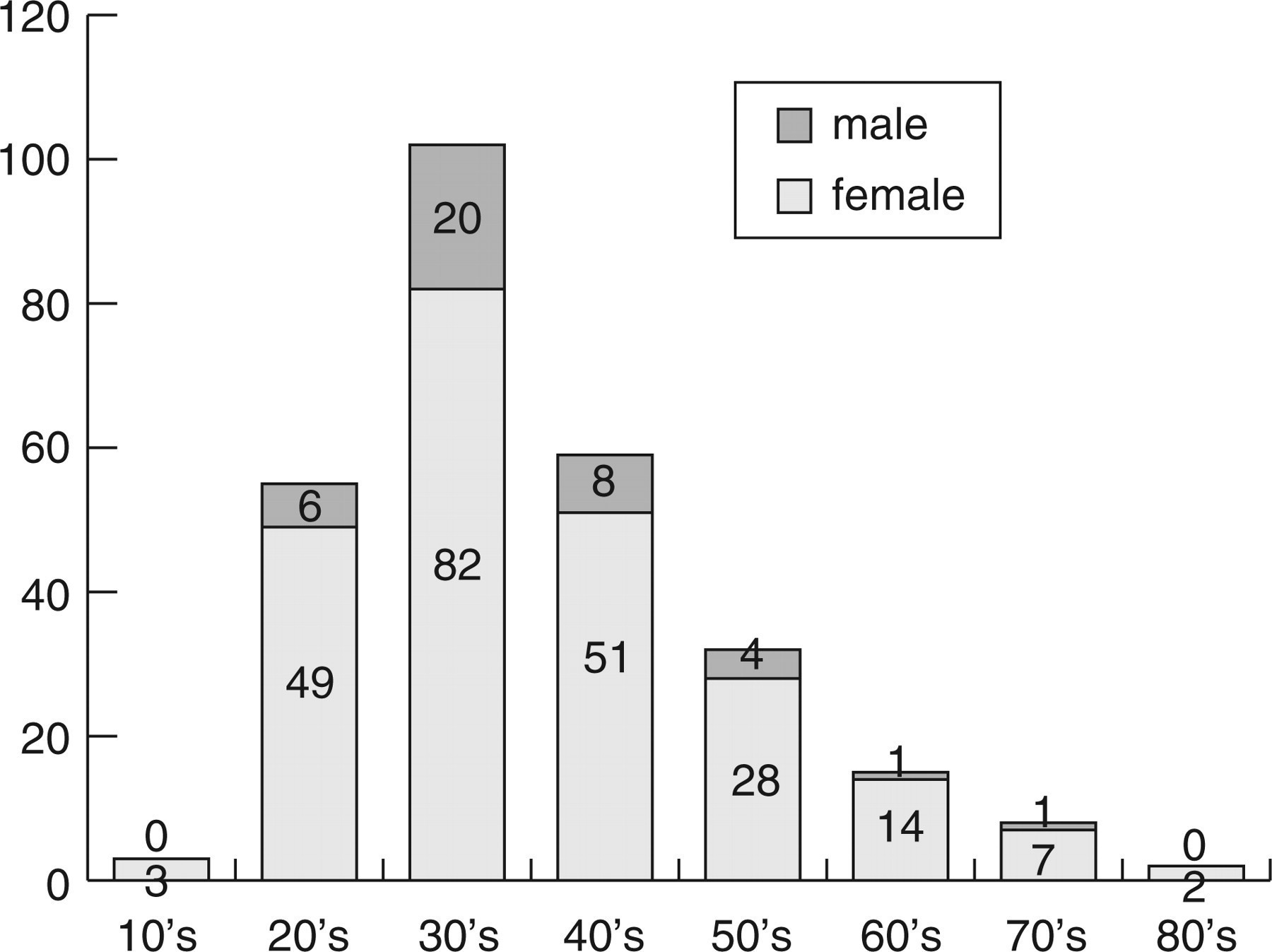
The age distribution of medication overuse headache (MOH) patients. Male : female = 40 : 236.
Diener and Dahlöf have summarized 29 studies, which included 2612 MOH patients (3). According to their meta-analysis, migraine was the primary headache in 65% of patients, TTH in 27%, and mixed or other headaches in 8%. Migraine was the primary headache in 80.9% of the MOH patients in Imai's study, and in 72.8% of the MOH patients in Nagaseki's. These figures were higher than the data in the meta-analysis. The prevalence of migraine in Japan is reported to be 8.4%, which is roughly equivalent to other countries (4). Thus, the higher percentage of migraine as the primary headache in Japanese MOH patients cannot be explained by a higher prevalence of migraine in Japan. Many of migraine patients in Japan do not visit a doctor and take only OTC medications. Of migraine sufferers, 56.8% use only OTC analgesics in Japan (4). Many OTC analgesics are combination medications and readily available. It can be speculated that migraine is not well controlled by OTC medications, and therefore many migraine sufferers keep taking medications, ending up with medication overuse. Some may acquire MOH in that process. It is strongly recommended that migraine sufferers consult a doctor in order to lift the burden of migraine and also to prevent MOH attributed to OTC medications.
Women are thought to be more prone to MOH than men even after taking the sex differences in the prevalence of migraine into account. The same tendency is recognized in Japan also.
Regarding causative drugs for MOH, combination analgesics were the most popular ones in Japan. Neither barbiturates nor codeine are used in analgesics in Japan, but doctors should pay attention to what a patient is prescribed by other doctors, since that might contain some of those substances. Some cold remedies of OTC medications contain codeine, and some headache patients have found these remedies effective for their headaches. Special attention should be paid to this fact in clinical practice.
Triptans were not as much overused as in other countries. There are some possible explanations for the difference. Triptans have been introduced only recently to Japan compared with other countries. Thus Japanese headache patients have not yet been much exposed to triptans. Furhtermore, many Japanese migraine patients do not visit a doctor regularly and they manage to handle their headaches with only non-prescribed drugs. As prescriptions for triptans increase, MOH attributed to triptans may also increase in Japan.
As regards treatments for MOH, there are no specific guidelines in Japan. Abrupt withdrawal of causative drugs seems to be the most effective way. Abrupt out-patient withdrawal is usually recommended in the first place. If that method seems to be difficult, in-patient withdrawal will be considered. Tapering out-patient withdrawal seems to be the last method to be chosen. Takase and colleagues have reported a study on long-term prognosis of MOH in Japan (5), which indicated tapering out-patient withdrawal results in a poor outcome. Ninety-five per cent of their long-followed cases with tapering method have failed to withdraw analgesics.
During withdrawal treatment, prophylaxis medications for primary headache are often used. Tricyclic antidepressants such as amitriptyline are widely used for prevention of both migraine and TTH. For migraine, a calcium channel blocker, lomerizine, is used in Japan. Anticonvulsants are also used, and topiramate is now in clinical trial. Oriental herbal medicine, acupuncture and headache exercise are applied with some intractable headache cases. They could be a supportive choice for MOH treatment.
MOH is a growing problem in Japanese clinical practice. Many MOH patients continue to take analgesics unaware that their actions cause headache. For prevention of MOH, education of patients is the most important factor. Mental support for patients who are under withdrawal treatment is also necessary. Primary headaches need to be well controlled before development of MOH, since overuse of analgesics occurs in dealing with poorly controlled primary headaches. There are a growing number of headache specialists in Japan, and thus it is not difficult for a headache patient to consult a headache specialist. It should be widely recognized that headache is a symptom requiring appropriate medical attention and treatment.