
Abstract
Research suggests that a significant number of women first experience domestic violence during pregnancy. The current study examines correlates of violence during pregnancy, first by comparing women who did and did not report violence, and second examining three subgroups of women who reported violence (violence initiated, violence persisted, violence ceased). Results indicated that controlling for demographics, more frequent violence was associated with less support and satisfaction with support from the baby's father, more negative interactions with the baby's father, and more verbal aggression in their relationships than those who did not report violence. Differences among subgroups of women reporting violence emerged only for the relationship variables. Implications for detecting violence in clinical settings are discussed.
Over the past 20 years, the issue of domestic violence during pregnancy has received increasing attention, especially with respect to prevalence, screening in medical settings, and the effects of violence on birth outcomes (ACOG, 1995; Gazmararian et al., 1996; Hillard, 1985; Janssen et al., 2003; McGrath, Hogan, & Peipert, 1998). Recent studies have documented that 4% to 37% of women sustain acts of violence during pregnancy (Ghazal & Block, 1993; Martin, Mackie, Kupper, Buescher, & Moracco, 2001; McFarlane, Parker, & Soeken, 1996b; Torres et al., 2000). Several researchers have noted that a significant number of women report that partners who had not previously used violence began using violence during pregnancy (Ballard et al., 1998; Jasinski & Kantor, 2001; Webster, Sweett, & Stolz, 1994) or soon after (Gielen, O'Campo, Faden, Kass, & Xue, 1994; Stewart, 1994), whereas others have noted that pregnancy can be a respite from violence for some women (Campbell, Oliver, & Bullock, 1998). The current study cross-sectionally examined differences between women who did and did not report being the victims of violence during pregnancy. Among those reporting any violence, patterns of correlates among three subgroups of women (those who reported violence prior to and during pregnancy, those who reported violence prior to but not during pregnancy, and those for whom violence started during pregnancy) were examined.
Physical assault during pregnancy is cause for special concern because it poses a possible threat to the health of both the pregnant woman and the fetus (ACOG, 1995; Huth-Bocks, Levendosky, & Bogat, 2002; Newberger et al., 1992). For the woman, violence during pregnancy may be related to both physical and mental health outcomes, including anxiety (Campbell, Poland, Waller, & Ager, 1992), stress (Altarac & Strobino, 2002; Cokkinides & Coker, 1998; Curry, 1998), depression (Campbell et al., 1992; Cascardi & O'Leary, 1992), substance use (Cokkinides & Coker, 1998), infections (Parker, McFarlane, & Soeken, 1994), failure to gain weight during pregnancy (Parker et al., 1994), and labor and delivery complications (Valdez-Santiago & Sanin-Aguirre, 1996). In addition, there is preliminary evidence that women abused during pregnancy are more at risk for being murdered by their partner than nonpregnant abused women (Campbell, Soeken, McFarlane, & Parker, 1998). For the infant, results have been mixed, but indicate that violence during pregnancy may be associated with lower birth weight (Campbell et al., 1999; Curry & Harvey, 1998; Huth-Bocks et al., 2002; Lipsky, Holt, Easterling, & Critchlow, 2003; McFarlane, Parker, & Soeken, 1996a). Recent research has suggested that the stress specifically associated with violence during pregnancy is associated with low birth weight (Altarac & Strobino, 2002). Assault involving abdominal trauma could lead to fetal fractures, rupture of the uterus, and antepartum hemorrhage (Janssen et al., 2003; Sammons, 1981), as well as fetal loss or delivery of a preterm infant (Berenson, Wiemann, Wilkinson, Jones, & Anderson, 1994; Connolly, Katz, Bash, McMahon, & Hansen, 1997; Janssen et al., 2003; Lipsky et al., 2003; Pearlman, Tintinalli, & Lorenz, 1990; Rimsza, 1989).
Psychosocial Factors
Psychosocial factors have also been identified as important predictors of adverse birth outcomes (Stanton, Lobel, Sears, & DeLuca, 2002; Wilson et al., 1996). Stress and anxiety have been linked to adverse birth outcomes both directly and indirectly via negative health behaviors, and depression during pregnancy has been associated with lower birth weight (Hoffman & Hatch, 2000; Paarlberg et al., 1999). In particular, research over 30 years has yielded a consistent association between stress and low birth weight, and a less consistent association with gestational length and preterm delivery (Curry & Harvey, 1998; Hobel, Dunkel-Schetter, Roesch, Castro, & Arora, 1999; Hoffman & Hatch, 1996; Lederman, 1995; Lobel, 1994; Paarlberg, Vingerhoets, Passchier, Dekker, & Van Geijn, 1995; Rondo et al., 2003; Wadhwa, Sandman, Porto, Dunkel-Schetter, & Garite, 1993), with evidence that chronic stress may be more detrimental than specific episodes of high stress at critical periods (Glynn, Wadhwa, Dunkel-Schetter, Chicz-DeMet, & Sandman, 2001; Lobel, DeVincent, Kaminer, & Meyer, 2000). Explanatory mechanisms that have received support include elevated levels of corticotropin-releasing hormone in the hypothalamus, pituitary gland, and placenta during stress that trigger preterm delivery (Hobel & Culhane, 2003; Hobel, Dunkel-Schetter, & Roesch, 1998; Wadhwa, Porto, Garite, Chicz-DeMet, & Sandman, 1998), and the release of catecholamines resulting in decreased fetal growth or preterm delivery (McAnarney & Stevens-Simon, 1990). Stress may also be indirectly associated with adverse outcomes through health-compromising behaviors. A recent review (Dunkel-Schetter, Gurung, Lobel, & Wadhwa, 2001) suggests that stress is associated with several health-compromising behaviors, including substance use, poor nutrition, and lack of exercise, which may result in adverse birth outcomes (Boyles et al., 2000; Dunkel-Schetter et al., 2001; Rondo et al., 2003).
Relationship Factors
One important mediator of the association between stress and adverse outcomes is social support. Evidence suggests that social support serves not only a buffering effect, but also has a direct or main effect on birth outcomes (Collins, Dunkel-Schetter, Lobel, & Scrimshaw, 1993; Dunkel-Schetter et al., 2001; Feldman, Dunkel-Schetter, Sandman, & Wadhwa, 2000; Hoffman & Hatch, 2000). Specifically, social support and large social networks have been linked to increased birth weight (Collins et al., 1993; Turner, Grindstaff, & Phillips, 1990), and recent evidence suggests this effect is a function of fetal growth rather than gestational length (Feldman et al., 2000). Who provides support is also important, with research suggesting that support from husbands and partners is associated with better birth outcomes, whereas support from family has less of an effect (Dunkel-Schetter et al., 2001), although there may be cultural differences in the role of support during pregnancy from different members of the social network (Dunkel-Schetter, Sagrestano, Feldman, & Killingsworth, 1996; Sagrestano, Feldman, Dunkel-Schetter, & Killingsworth Rini, 1999). Thus, although violence during pregnancy may not be severe enough to have physical impact on the fetus, psychosocial factors associated with being the victim of violence may have an impact on the developing fetus in adverse ways. Therefore, understanding the psychosocial effects of domestic violence during pregnancy is warranted.
Relatively little is known about the processes of change in relationship conflict and violence during pregnancy and following the birth of a new child. There is some evidence that pregnancy causes disequilibrium for couples, including shifts in power and major changes in communication patterns prior to the birth (Leifer, 1977, 1980; Seegmiller, 1993). Such changes may be magnified for couples that are not married and/or did not plan the pregnancy (Cox, Paley, Burchinal, & Payne, 1999). Fitzpatrick and colleagues (Fitzpatrick, Vangelisti, & Firman, 1994) prospectively found that 68.9% of husbands and 74.2% of wives reported an increase in conflict during pregnancy. To the extent that conflict may be a precursor to violence (Follingstad, Rutledge, Berg, Hause, & Polek, 1990; Hyden, 1995; Sagrestano, Heavey, & Christensen, 1999), and to the extent that pregnancy is associated with increased stress (Arizmendi & Affonso, 1987) and conflict (Fitzpatrick et al., 1994), it is reasonable to hypothesize that pregnancy and the impending transition to parenthood may lead to increased violence against women. This may be especially true when the pregnancy is unplanned, because an unplanned pregnancy is more likely to result in a stressful transition (Cox et al., 1999; Stewart & Cecutti, 1993). Evidence suggests a higher prevalence of violence against pregnant women when men perceive the pregnancy to be unplanned than planned (Jasinski, 2001).
Demographic Factors
In addition to psychological and relationship factors, demographic and background factors have been found to be associated with violence, and therefore should be examined as additional correlates of violence during pregnancy. For example, previous research suggests that women abused during pregnancy are more likely to be younger, unmarried, and have lower income and education than women who are not abused during pregnancy (Hedin & Janson, 2000; Newberger et al., 1992; Torres et al., 2000). However, because age has consistently been associated with violence, other associations between age-associated demographics (e.g., education, income, marital status) and violence may be spurious. Research on racial and ethnic variability in prevalence of violence during pregnancy are quite mixed (Torres et al., 2000). Few studies have examined this issue in the context of pregnancy; however, a recent study with a large, ethnically diverse sample indicated that Latinas did not differ significantly from European American women, whereas African American women were more likely to report abuse during pregnancy than European American women (Torres et al., 2000).
Race and ethnicity are also associated with psychological and relationship factors during pregnancy, although comparative research in this area is limited. Specifically, ethnic minority women tend to experience more stress during pregnancy than their peers (DaCosta, Larouche, Dritsa, & Brender, 1999; Dunkel-Schetter, 1998), and Latinas report more state anxiety and prenatal anxiety than women of other ethnic backgrounds (Lederman, 1995). Although African American women may have higher rates of depression than White women in general, among low-income pregnant women, differences in rates of depression are not evident (Hobfoll, Ritter, Lavin, Hulsizer, & Cameron, 1995; Ritter, Hobfoll, Lavin, Cameron, & Hulsizer, 2000). In the context of pregnancy, White women report receiving more support and having larger support networks than African American and Latina women (Koniak-Griffin, Lominska, & Brecht, 1993; Norbeck & Anderson, 1989), however, Latinas report more support from their partners and their mothers than do Whites and African Americans (Sagrestano, Feldman et al., 1999). These findings, however, must be considered with caution. Research suggests that when controlling for demographic differences among ethnic groups (e.g., marital status, socioeconomic status), ethnic differences in support during pregnancy were either less robust or no longer significant (Sagrestano, Feldman et al., 1999).
Patterns of Violence
In an attempt to better understand subgroups of women reporting violence and variations in prevalence estimates of violence during pregnancy, Ballard and colleagues (Ballard et al., 1998), in a review and synthesis of existing research on measurement of domestic violence during pregnancy, identified four distinct groups of pregnant women, further studied and labeled by Jasinski (2001) as: (1) no violence: no violence before or during pregnancy, (2) persistent violence: violence before and during pregnancy, (3) violence cessation: violence before but not during pregnancy, and (4) violence initiation: violence during, but not before pregnancy. Research suggests that between 36% and 50% of victims report that violence ceases during pregnancy, beginning again after the child is born, suggesting that for those women, pregnancy serves as a protective period from abusive partners (Campbell, Oliver et al., 1998; Hillard, 1985). In contrast, for some women the frequency and intensity of violence increases during pregnancy (Campbell et al., 1998; Hillard, 1985; Walker, 1984). Whether or not rates of initiation differ between pregnant women and non-pregnant women remains unclear, because once other variables such as age are controlled, differences are no longer statistically significant (Jasinski, 2001). However, certain pregnancy-related factors such as whether the pregnancy was a first pregnancy or planned are associated with higher violence (Jasinski, 2001). Ballard and colleagues (Ballard et al., 1998) suggest that variations in reported prevalence rates could be understood by examining differences in patterns of correlates among these distinct groups. Specifically, demographic, psychological, and relationship factors during pregnancy may serve to distinguish patterns among groups. One study (Jasinski, 2001) examined demographic and pregnancy-related variables and found that being younger and having an unplanned pregnancy is associated with persistent violence, violence cessation, and violence initiation, whereas cohabitation is associated with persistent violence and initiating violence, but not violence cessation. Psychological and relationship factors have not yet been investigated in this way.
Current Study
The current study examines associations between demographic, psychological, and relationship factors and the incidence of domestic violence during pregnancy. Our first goal was to examine ethnic differences in demographic, psychological, relationship, and violence variables. Based on limited previous research examining racial and ethnic differences in psychosocial factors during pregnancy, we hypothesized that Latinas would report more anxiety, depression, and stress than African Americans (Corcoran & Franklin, 2002; Lederman, 1995), but more social support (Sagrestano, Feldman et al., 1999) and less violence than African Americans (Torres et al., 2000).
The second goal of the study was to examine the extent to which demographic, psychological, and relationship variables explained variance in the frequency of violence reported by women. We hypothesized that each set of variables (demographic, psychological, relationship) would predict unique variance, above and beyond the previous set of variables, in explaining the frequency of violence experienced by women. Specifically, it was expected that higher levels of stress, anxiety, depression, negative interactions with the baby's father, and verbal aggression, and less support from the baby's father and satisfaction with that support, would be associated with higher frequency of violence.
The third goal of the study was to examine differences among subgroups of women who reported violence, because the pattern of correlates for these groups may differ. Based on limited previous research examining these subgroups, it was hypothesized that women who cohabited with their partners would be more likely to report patterns of violence initiation or persistence than cessation as compared to those who were married to their partners (Jasinski, 2001). Women who reported that violence initiated during pregnancy would be more likely to report an unplanned pregnancy than those who reported persistent violence, followed by a pattern of violence cessation (Jasinski, 2001). Finally, younger women were hypothesized to report patterns of violence initiation or persistence more so than cessation (Jasinski, 2001). A series of intuitive hypotheses were developed with respect to psychological and relationship variables, as there was no literature on which to base them. Women who reported that violence initiated or persisted during pregnancy were expected to report higher levels of anxiety, depression, and stress, and lower levels of social support and satisfaction with support than those who reported that it ceased. Women who reported that violence persisted were expected to report more negative interactions with the baby's father and more verbal aggression than those who reported that violence initiated or ceased during pregnancy.
METHOD
Participants
Two hundred pregnant women with a gestational age of at least 20 weeks (M = 28.68, SD = 5.49) were recruited randomly from the University of Illinois at Chicago Women's Care Center. The clinic serves primarily African American and Latina women who are low-income, inner-city residents. Three women who had no interaction with the baby's father were dropped, resulting in a sample of 197 women with complete data. Sample demographic characteristics are presented in the results section.
Measures
Domestic violence.
The Conflict Tactics Scale (CTS; Straus, 1979) is a psychometrically sound (e.g., Barling, O'Leary, Jouriles, Vivian, & MacEwan, 1987), 19-item measure designed to assess interaction techniques used during conflict. The CTS is the most widely used measure of marital violence (Babcock, Waltz, Jacobson, & Gottman, 1993; Straus, Hamby, McCoy, & Sugarman, 1996), although it has several disadvantages, most notably that the effects, severity, and consequences of violent acts are not considered (White, Smith, Koss, & Figueredo, 2000). It has been used in several national samples (e.g., Straus, Gelles, & Steinmetz, 1980), and has been tested with pregnant women (McFarlane et al., 1996b). For each item, patients indicated how often in the past year their partner had engaged in the behavior toward them on a scale of 0 (never) to 6 (more than 20 times). They were then asked if it had ever happened during this pregnancy (yes or no), and if so, whether the first time it had happened was during this pregnancy (yes or no). Responses to these items were used to categorize women into the four groups as defined by Ballard et al. (1998). Two subscales were used in the current analyses. The Verbal Aggression subscale consisted of six items describing frequency of verbal and nonverbal acts to symbolically hurt the other. The Violence subscale consisted of eight items describing the frequency of use of physical force. The verbal aggression (α = .83) and violence (α = .84) subscales were internally consistent in this sample.
Anxiety.
Anxiety was measured using the state anxiety form of the State-Trait Anxiety Inventory (Spielberger, 1983). Participants responded to 10 items (e.g., I am tense; I am presently worrying over possible misfortune) on a scale of 1 (not at all) to 4 (very much). This measure has been used extensively in research on pregnancy anxiety, including samples of low-income women and women of color (Engle, Scrimshaw, Zambrana, & Dunkel-Schetter, 1990; Killingsworth Rini, Dunkel-Schetter, Wadhwa, & Sandman, 1999; Lobel, Dunkel-Schetter, & Scrimshaw, 1992), and has been shown to predict birth outcomes (Levin & DeFrank, 1988). The scale had high inter-item reliability (α = .84) in the current sample.
Depression.
Depressive symptomatology was measured with the Center for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977). Participants responded to 20 items (e.g., I had trouble keeping my mind on what I was doing, I felt that everything I did was an effort) on a scale of 1 (rarely or none of the time) to 4 (most or all of the time). The CES-D is a widely used measure of depressive symptomatology and has been shown to be valid and reliable in many samples, including pregnant women (Turner et al., 1990) from ethnically diverse and low-income backgrounds (Collins et al., 1993; Hoffman & Hatch, 2000). The CES-D had high inter-item reliability (α = .90).
Perceived stress.
The Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983) was used to measure general or nonspecific stress. The PSS is a psychometrically sound, 14-item questionnaire measuring the degree to which women feel that their lives are unpredictable, uncontrollable, and overwhelming on a scale of 1 (never) to 5 (almost always). The measure has been used extensively in pregnancy research, including low-income women and women of color (Lobel et al., 1992; Rondo et al., 2003; Wadhwa, Dunkel-Schetter, Chicz-DeMet, & Porto, 1996). The scale had moderately high inter-item reliability (α = .78) in this sample.
Social support from baby's father.
Social support from the baby's father was measured using a 6-item scale developed for use with pregnant women and first tested in two samples of ethnically diverse, low-income women (Collins et al., 1993; Sagrestano, Feldman et al., 1999). The scale assesses received support rather than perceived support. Participants were asked how much the baby's father provided them various types of support (e.g., information, material needs, advice) on a scale of 1 (never) to 5 (always). The scale had high inter-item reliability in this sample (α = .92).
Satisfaction with support from baby's father.
Satisfaction with social support from the baby's father was measured using a 6-item scale developed for use with pregnant women and first tested in two samples of ethnically diverse, low-income women (Collins et al., 1993; Sagrestano, Feldman et al., 1999). Following each of the support items described above, participants were asked to indicate their satisfaction with the level of support received for that type of support on a scale of 1 (not at all satisfied) to 5 (completely satisfied). The satisfaction with support scale had high inter-item reliability in this sample (α = .93).
Negative interactions with the baby's father.
An 8-item scale developed for use with pregnant women (Collins et al., 1993; Dunkel-Schetter, Feinstein, & Call, 1986) and tested in a sample of ethnically diverse, low-income women (Collins et al., 1993) was used to assess frequency of negative interactions with the baby's father (i.e., criticized, been angry, disappointed, irritated, put unreasonable demands, threatened, hurt, anything else upsetting) on a scale of 1 (never) to 5 (always). The scale had high inter-item reliability (α = .82).
Demographic and background variables.
Participants were asked a series of demographic and background questions about themselves, the baby's father, and their pregnancy. Specifically, women were asked to report age, ethnicity, education, and income for themselves and for their partners. Income was assessed using a 6-point scale of 1 = under $10,000; 2 = $10,001 to $20,000; 3 = $20,001 to $30,000; 4 = $30,001 to $40,000; 5 = $40,001 to $50,000; and 6 = above $50,000. In addition, questions were included to assess marital status, whether or not the pregnant women lived with the baby's father (living status), whether the pregnancy was planned, and whether the pregnant woman currently wanted the baby.
Procedure
Eligible women (pregnant women at least 20 weeks gestational age) were identified based on clinic schedules and recruited for the study. Specifically, potential participants were randomly approached in the waiting room of the clinic and asked if they would be willing to participate in a study of attitudes and feelings during pregnancy. Care was taken not to reveal the specific nature of the study, because many women were accompanied by partners who may not have allowed participation in a study of violence during pregnancy. If potential participants agreed, they were taken to a private room where confidentiality was explained and written informed consent was obtained. Fifteen women who were approached refused participation, resulting in a response rate of 93%. Reasons for refusal included not wanting to participate (n = 6), having a child with them (n = 4), lack of time (n = 3), being too tired (n = 1), and not speaking English well enough (n = 1). Women who agreed to participate were interviewed for approximately 45 minutes (in English or Spanish) by a trained member of the health care team. Women responded to background questions about their pregnancy, followed by measures of anxiety, perceived stress, social support from the baby's father, negative interactions with the baby's father, social support from friends and family (not included in the current analyses), depression, and domestic violence. Demographic information regarding themselves and their partners was collected last. All participants were thanked for their participation and provided with $10 for parking and other incidental expenses. Participants who indicated during the interview that their partner had abused them were referred to a social worker in the clinic for counseling and/or additional services.
Participants were assessed once, late enough in pregnancy to allow sufficient time for violence to begin (in cases where violence begins during pregnancy), yet early enough to capture adverse outcomes resulting from abuse, although this might have been limited by the timing, form, and severity of abuse. A single assessment was decided upon because the clinic management did not approve tracking appointments in their system, and following women outside of the clinic setting exceeded the resources of this study.
Spanish Translation
The complete interview protocol and all instructions and related materials were translated into Spanish. Specifically, Spanish versions of all published measures were sought from the original authors of the measures, and if not available, from others who had used the measure for research with Spanish-speaking populations. Spanish versions of all of the psychosocial measures were obtained from outside sources. For both the CTS and the CES-D, two different versions were obtained. In these two cases, two native Spanish-speaking translators affiliated with the project considered the two available translations and decided upon the translation that seemed most accurate. The consent forms, instructions, and other relevant materials were translated into Spanish by a native Spanish-speaking health care worker, and then back-translated into English by a different native Spanish-speaking health care worker. Comparisons were made between the two versions and where discrepancies existed, the researchers worked with the translators to resolve them.
Approximately 25% of the sample (N = 49) completed the interview in Spanish. Alpha reliabilities of the measures in Spanish were moderate to high, as follows: anxiety, .85; perceived stress, .78; depression, .93; received support from baby's father, .92; satisfaction with support from baby's father, .96; negative interactions with the baby's father, .81; verbal aggression, .66; and violence, .71.
RESULTS
Data Analytic Plan
Correlations among all study variables are presented in Table 1. Sample characteristics, including means and standard deviations for each of the measures, are reported below. The first goal of the study was to examine ethnic differences in demographic, psychological, and relationship variables. To test this series of hypotheses, t tests or chi-square analyses were conducted for each of the measures comparing Latinas and African American women.
The second goal of the study was to examine the extent to which demographic, psychological, and relationship variables explained variance in the frequency of violence reported by women. To test this hypothesis, a linear regression was performed with demographic variables entered in the first step, psychological variables entered in the second step, and relationship variables entered in the third step, to examine the percentage of variance in frequency of violence (as measured by the CTS violence scale score) explained by demographic, psychological, and relationship variables.
The third goal of the study was to examine differences among subgroups of women who did report violence, because the pattern of correlates for these groups may differ. To test this set of hypotheses, one-way ANOVAs or chi-square analyses were conducted to compare the three groups of women reporting violence.
Correlations Among Study Variables (N = 197)
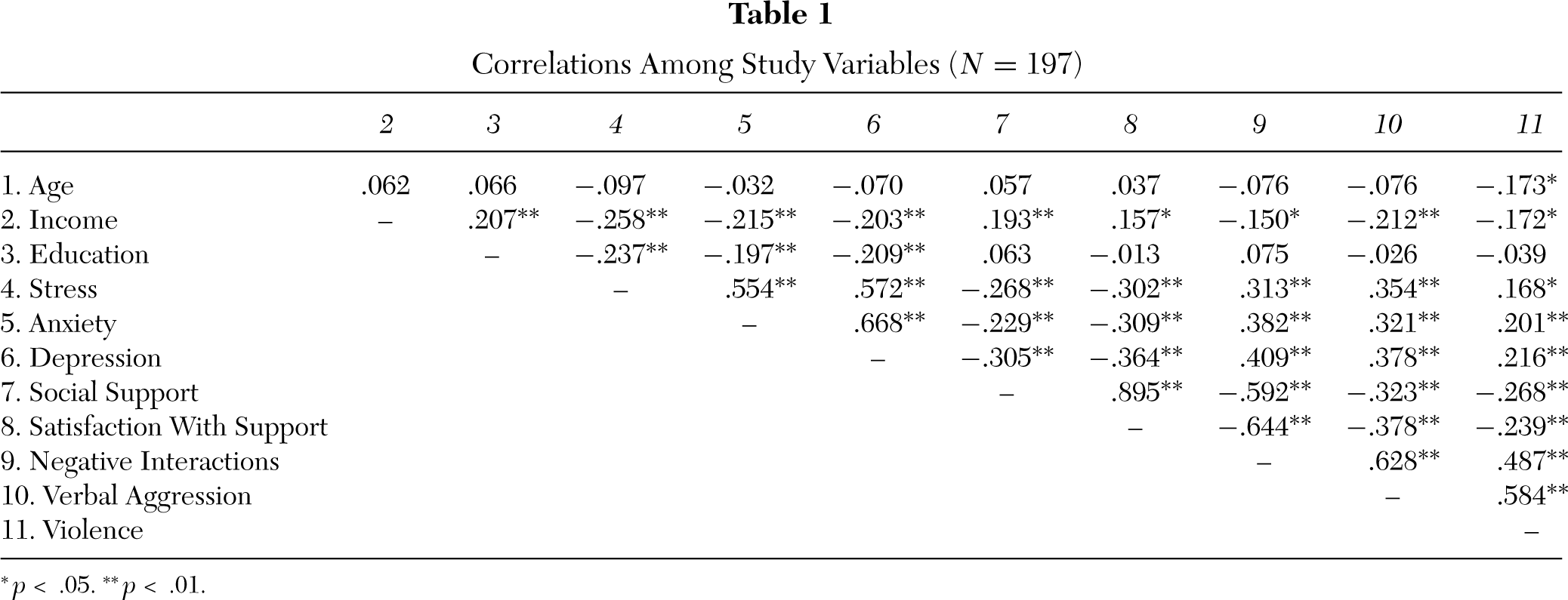
p < .05.
p < .01.
Sample Description and Examination of Ethnic Differences in Demographic, Psychological, and Relationship Variables
Means, standard deviations, and ethnic differences were examined for the demographic, psychological, and relationship variables.
Demographic characteristics.
The sample was 49% African American, 45% Latina, and 6% White or of other descent. The women ranged in age from 14 years to 41 years (M = 25.76, SD = 6.16). The majority of women were unmarried (65.5%), and 59.6% reported living with the baby's father (living status). Among those who were married, 85.3% lived with the baby's father, whereas among those who were unmarried, 45.3% lived with the baby's father. The median annual family income was between $10,000 to $20,000, and 49.4% reported an income of less than $10,000. The mean educational level was 10.8 years (SD = 3.07). Women's reports concerning the baby's father indicated that the mean age of the fathers was 28.81(SD = 7.44), the mean level of education was 11.22 years (SD = 2.83), and 79.3% were employed. Although 67% of the pregnancies were unintended, 98% of the women reported wanting the baby now.
Differences between the Latina and African American women were examined for all demographic variables. Significant differences emerged for education, marital status, living status, and whether the pregnancy was planned. Specifically, African American women (M = 12.13, SD = 2.29) had significantly higher levels of education than Latinas (M = 9.68, SD = 3.26). Latinas were significantly more likely to be married (45.5%), to live with the baby's father (74.2%), and to plan their pregnancies (41.6%) than were African American women (24.0% married, 43.8% live with, 21.9% planned pregnancy). In addition, African American women (M = 12.30, SD = 1.60) reported their partners to have significantly more education than did Latinas (M = 9.95, SD = 3.27), and partners of Latinas (88.4%) were more likely to be employed than partners of African American women (70.5%).
Psychological variables.
The sample reported moderate levels of anxiety (M = 2.05, SD = 0.65), depression (M = 1.85, SD = 0.57), and stress (M = 2.23, SD = 0.62). No significant ethnic differences emerged for the three psychological measures.
Relationship variables.
The sample reported moderate levels of social support from the baby's father (M = 3.88, SD = 1.18), satisfaction with support from the baby's father (M = 3.70, SD = 1.23), and negative interactions with the baby's father (M = 1.75, SD = 0.71). Ethnic differences emerged such that Latinas (support: M = 4.09, SD = 1.11; satisfaction: M = 3.98, SD = 1.15) reported more social support from the baby's father and more satisfaction with that support than did African American women (support: M = 3.68, SD = 1.20; satisfaction: M = 3.42, SD = 1.21). In contrast, African American women (M = 1.91, SD = 0.69) reported more negative interactions with the baby's father than did Latina women (M = 1.53, SD = 0.63).
With respect to domestic violence, women reported fairly low frequency of verbal aggression (M = 1.13, SD = 1.17) and violence (M = 0.20, SD = 0.60), as measured by the CTS. Scores on the CTS indicated that 84.3% of the women experienced some form of verbal aggression and 17.0% experienced some form of violence from their partner in the past year. During the current pregnancy, 68.1% experienced verbal aggression and 13.3% experienced violence from their partner. When asked when the violence began, 4.8% of the total sample (36.6% of those who reported violence during the current pregnancy) reported they first experienced some type of violence during this pregnancy. The majority of women reporting violence reported that their partners pushed, slapped, kicked, or hit them, whereas two women reported that their partners threatened them with a knife or gun.
Ethnic differences emerged such that African American women (M = 1.42, SD = 1.30) reported that their partners used verbal aggression more frequently in the past year than did Latinas (M = 0.81, SD = 0.90), however, no significant ethnic differences emerged for the violence subscale.
Comparisons of women reporting violence and those not reporting violence indicated that women reporting violence in the past year reported significantly younger age (violence, M = 23.02, SD = 5.41; no violence, M = 26.49, SD = 6.15; t = 3.29, p < .001), lower income (violence, M = 1.50, SD = 0.94; no violence, M = 1.92, SD = 1.09; t = 2.30, p < .05), younger age of the baby's father (violence, M = 26.68, SD = 6.38; no violence, M = 29.38, SD = 7.62; t = 2.08, p < .05), lower likelihood of the baby's father being employed (violence, 65.9%; no violence, 82.9%; χ2 = 5.71, p < .05), lower likelihood of being married (violence, 16.7%; no violence, 39.6%; χ2 = 7.67, p < .01), and lower likelihood of living with the baby's father (violence, 42.9%;no violence, 63.9%; χ2 = 6.05, p < .05) than those who did not report violence. No differences emerged in the educational levels of the women or their partners.
Do Demographic, Psychological, and Relationship Variables Explain Unique Variance in the Frequency of Violence Reported?
The second goal of the study was to examine the extent to which demographic, psychological, and relationship variables explained variance in the frequency of violence reported by the full sample of women in the study. A linear regression was performed with age, ethnicity, income, and living status entered in the first step; anxiety, stress, and depression entered in the second step; and negative interactions with the baby's father, support from the baby's father, satisfaction with support from the baby's father, and verbal aggression entered in the third step, to examine the percentage of variance in frequency of violence explained by demographic, psychological, and relationship variables. The overall regression accounted for 36.8% of the variance, however, several variables (i.e., ethnicity, living status, anxiety, stress, depression) did not emerge as significantly associated with frequency of violence. Therefore, those variables were dropped and a more parsimonious regression was run with the remaining variables (i.e., age, income, negative interactions with the baby's father, support from the baby's father, satisfaction with support from the baby's father, verbal aggression; see Table 2). 1 Results indicated that the demographic variables explained 6.3% of the variance in frequency of violence, and the relationship factors explained an additional 30.9% of the variance, for a total of 37.2% of the variance explained. Specifically, those who were younger, had less income, reported more negative interactions with the baby's father, less support from the baby's father, less satisfaction with the support they received from the baby's father, and more verbal aggression reported more frequent violence than their peers.
Linear Regression Analyses Regressing CTS Violence Scale Scores on Demographic, Psychological, and Relationship Variables (n = 188)
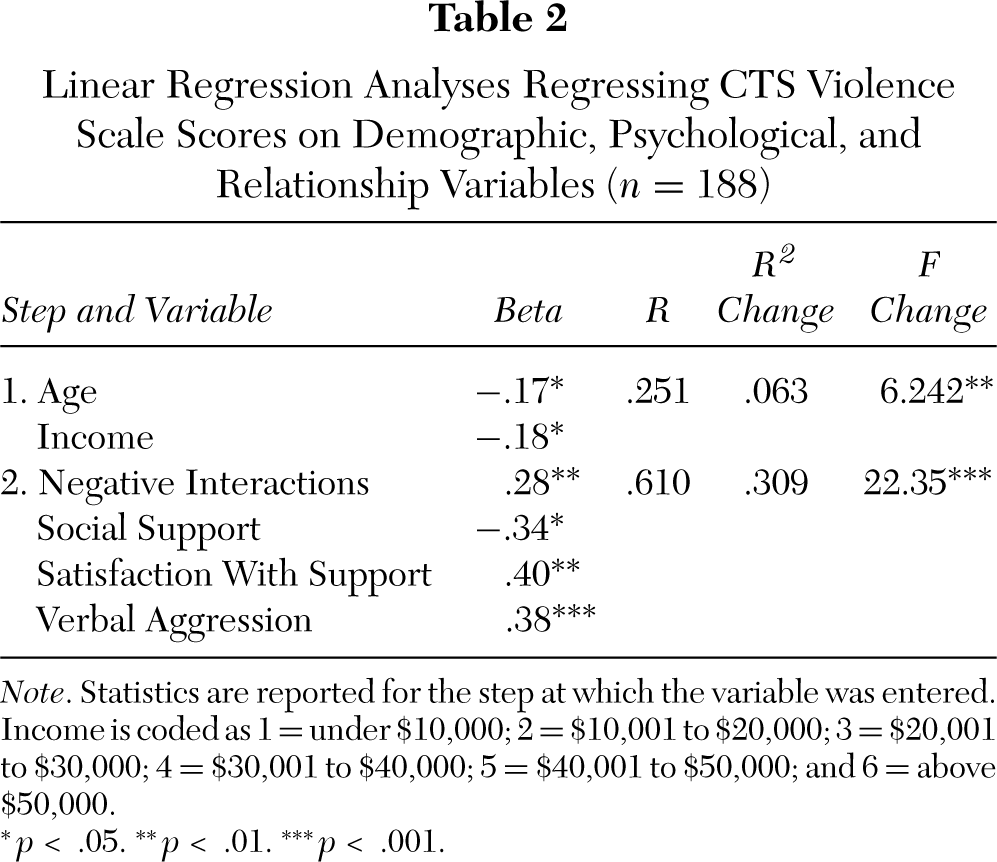
Note. Statistics are reported for the step at which the variable was entered. Income is coded as 1 = under $10,000; 2 = $10,001 to $20,000; 3 = $20,001 to $30,000; 4 = $30,001 to $40,000; 5 = $40,001 to $50,000; and 6 = above $50,000.
p < .05.
p < .01.
p < .001.
Examination of Differences Among Subgroups of Women Who Reported Violence
The third goal of the study was to examine differences among subgroups of women who reported violence. One-way ANOVAs or chi-square analyses were conducted to compare the three groups of women reporting violence (see Table 3), although the group sample sizes were fairly small, resulting in relatively low power. Contrary to hypotheses, there were no significant differences among these groups of women in demographic variables, nor were there differences in the psychological variables. However, with respect to the relationship variables, as hypothesized, results indicated that women who reported that the violence ceased during pregnancy reported more support and satisfaction with support from the baby's father than did women who reported that the violence initiated during pregnancy. Women who reported persistent violence reported more frequent verbal aggression and violence than women who reported that the violence either ceased or initiated during pregnancy.
Descriptive Data and Univariate Analyses of Demographic, Psychological, and Relationship Variables Among the Three Groups Reporting Violence (n = 43)
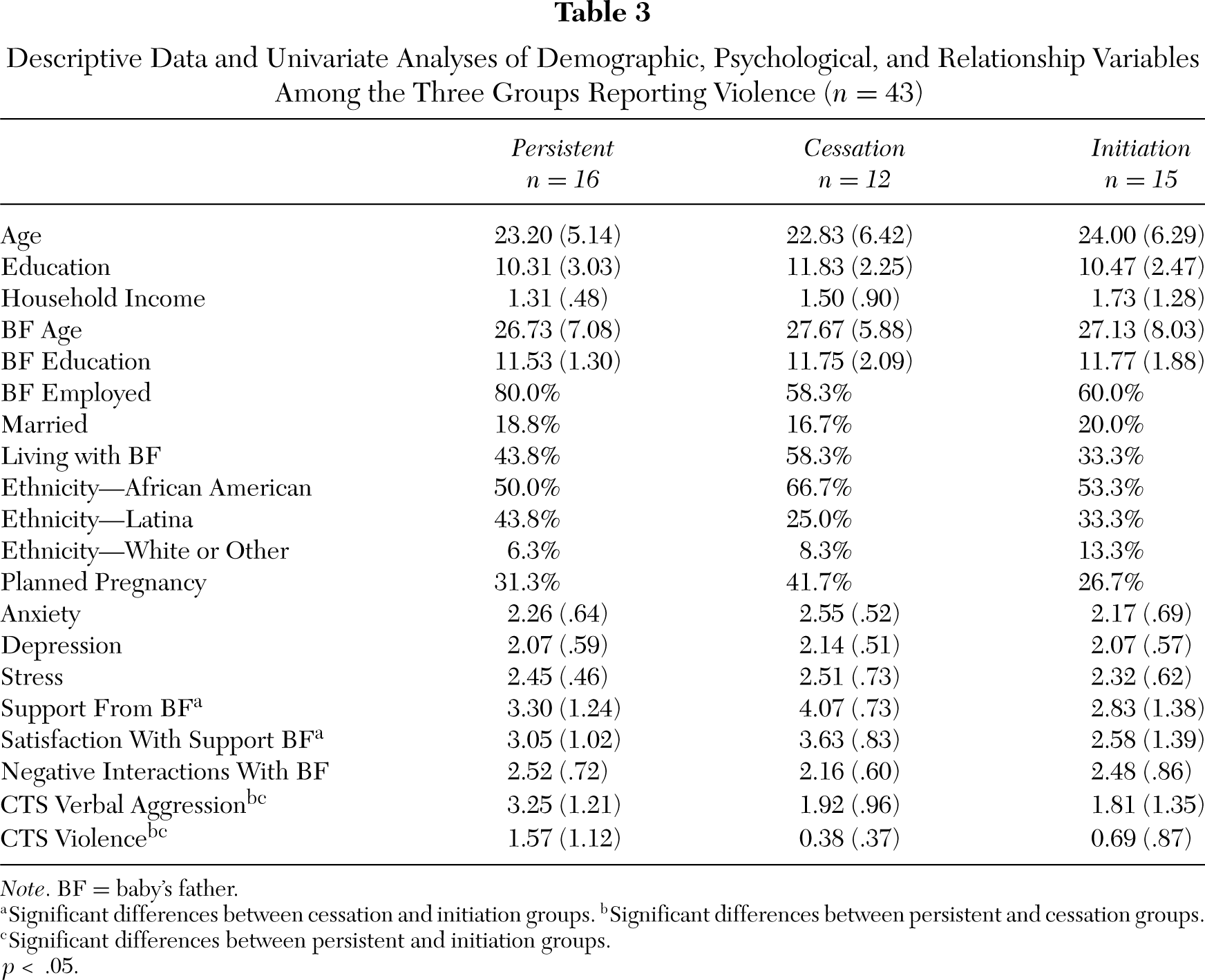
Note. BF = baby's father.
Significant differences between cessation and initiation groups.
Significant differences between persistent and cessation groups.
Significant differences between persistent and initiation groups. ∗p < .05.
DISCUSSION
The current study cross-sectionally examined differences between women who did and did not report being the victims of violence during pregnancy, and among those who did, examined patterns of correlates among three subgroups of women: those who report violence prior to and during pregnancy, those who report violence prior to but not during pregnancy, and those for whom violence starts during pregnancy. Specifically, it examined psychosocial correlates of violence during pregnancy, including stress, depression, anxiety, social support, and relationship conflict. Three main goals were outlined for the study, the findings of which will be discussed in turn.
The first goal of the study was to examine ethnic differences in demographic, psychological, relationship, and violence variables. The findings partially confirmed hypotheses based on limited previous research, specifically with respect to the relationship variables, but not the psychological variables. Latinas reported more social support from the baby's father, fewer negative interactions and less verbal aggression from him than did African American women. Contrary to hypotheses, no ethnic differences in psychological variables emerged. The findings with respect to the relationships variables likely reflect differences in marital status between the groups, as previous research suggests that univariate ethnic differences in social support do not hold up when other demographic factors are controlled (Sagrestano, Feldman et al., 1999). Specifically, research suggests marital status is the most important predicator of support from the baby's father, and when controlling for marital status and socioeconomic status, ethnic differences in support are no longer significant (Sagrestano, Feldman et al., 1999). In the current sample, the Latinas were significantly more likely to be married than the African American women (Latinas: 45.5% married, 74.2% live with; African Americans: 24.0% married, 43.8% live with), which may partially explain differences in the relationships variables, in general. One could conjecture that married and cohabiting couples spend more time together than couples who are unmarried and not living together, and that the married father may be more available and committed to the relationship, and therefore more likely to provide support. In contrast, unmarried couples may experience more conflict surrounding the pregnancy and their relationship status, thus resulting in higher levels of negative interactions and verbal aggression.
Contrary to hypothesis, ethnic differences did not emerge for the psychological variables. Given that there was such limited previous research reporting ethnic differences, it is possible that the few studies that were found reporting differences reflect Type I error, and many other studies did not report on whether there were ethnic differences because none were found. From a theoretical perspective, there is little reason to expect ethnic differences in stress, anxiety, and depression. It is more likely that other demographic factors, such as socioeconomic status, explain more variance in the psychological experience of women during pregnancy (Hobfoll, 1989). Given that this sample is predominantly low-income, the general circumstances surrounding their pregnancies may be more similar than different, leading to similar levels of stress, anxiety, and depression.
The second goal of the study was to examine the extent to which demographic, psychological, and relationship variables explained variance in the frequency of violence reported by women. Results indicated that both demographic and relationship variables explained unique variance, whereas psychological variables did not. Furthermore, relationship variables explained considerably more variance in frequency than did demographic variables. Given causal ordering and that women do not tend to have control over the frequency with which they are victimized, it is not surprising that the demographic variables explain less variance than the variables that are specific to women's interactions with their partners.
With respect to the relationship variables, controlling for demographics, those reporting more negative interactions with the baby's father, more use of verbal aggression by the baby's father, less support from the baby's father, and less satisfaction with the support they received from the baby's father, were more likely to report violence than their peers. These findings are especially interesting because most research on the psychosocial correlates of violence during pregnancy focus on the psychological variables (e.g., stress, anxiety, depression), which were found to be nonsignificant in these analyses, and not variables related to the nature of the relationship with the baby's father. This may give us insight into the conflict dynamics of those couples in which the man initiates violence during pregnancy. Especially notable, the negative interactions with baby's father questionnaire explicitly measures the amount of stress experienced by the woman as a result of negative interactions with the baby's father (as opposed to the PSS, which measures nonspecific stress). This suggests that women who report violence are experiencing a fair amount of stress specifically derived from their intimate relationship, and in addition, they are not receiving high levels of social support or experiencing satisfaction with that support. Although it is not surprising that women who experience violence experience lack of support, this may be especially critical for pregnant women. Previous research suggests that stress associated with violence is associated with low birth weight (Altarac & Strobino, 2002), whereas social support from the baby's father is associated with increased birth weight (Collins et al., 1993; Turner et al., 1990), and therefore, increased relationship stress coupled with lack of support from the primary partner may not only put the woman at increased risk for adverse psychological and physical outcomes, but may also put her baby at increased risk for adverse birth outcomes (Altarac & Strobino, 2002; Collins et al., 1993; Lobel et al., 1992; Turner et al., 1990; Wadhwa et al., 1993).
Negative interactions or conflict with the baby's father may be a promising area for screening in obstetrical settings. Although the American College of Obstetricians and Gynecologists has long been calling for routine screening for domestic violence during obstetric and gynecological visits (ACOG, 1995; McGrath et al., 1998), preliminary research suggests that many practices and clinics do not screen. This likely happens for multiple reasons, ranging from lack of training to lack of time during visits. Instead, research suggests that screening in the OB/GYN setting is likely to occur primarily when abuse is suspected (Horan, Chapin, Klein, Schmidt, & Shulkin, 1998; Parsons, Zaccarro, Wells, & Stovall, 1995). Although routine prenatal screening is recommended, to the extent that correlates of violence can serve as markers, women who present with these symptoms could be targeted for screening for domestic violence by those health care providers who choose not to routinely screen. Furthermore, many women may not feel comfortable revealing violence to their health care provider because they may be concerned about increased violence, unwanted police involvement, or loss of child custody (Chang et al., 2003; Petersen, Moracco, Goldstein, & Clark, 2003). A screening measure that explicitly examines negative interactions with the baby's father, administered previous to screening for violence during pregnancy, may help identify women who are experiencing violence but do not choose to report it to their health care provider. Similar to other screening measures, women who score high on negative interactions may be referred to a social worker or other mental health professional that could follow up and identify potential victims and provide them with appropriate services or shelter. Indeed, although women report multiple barriers to disclosing violence in the health care setting, research indicates that women perceive the health care system as a potentially valuable source of referrals to community-based services such as job training and financial support (Petersen et al., 2003).
The third goal was to examine differences among subgroups of women who did report violence, because the pattern of correlates for these groups may differ. Although all three groups of women were small, it is interesting to consider the similarities and differences among these women, especially because data comparing these groups are rare (Ballard et al., 1998; Jasinski, 2001). Contrary to hypotheses, no significant differences emerged among the three groups for any of the demographic or psychological factors; however, differences did emerge when comparing women on the relationship factors. Specifically, analyses revealed that those who reported the violence initiated during pregnancy reported less support from the baby's father and less satisfaction with that support than those who reported that the violence ceased. Not surprisingly, the women who reported that violence persisted from prepregnancy into pregnancy reported that their partners used verbal aggression and violence more frequently than those women who reported that violence ceased or was initiated during pregnancy. However, given the small sample sizes, these results must be considered with caution.
The findings that the group for whom violence initiated during pregnancy reported the lowest levels of social support and higher (although not significantly higher) levels of violence than the violence cessation group fits with an ecological explanation of the interdependence of stress and social support. Specifically, stress may ultimately diminish support, especially for those with fewer resources, in this case leading to a sense of betrayal in the time of need, so to speak (Hobfoll, 1988; Vaux, 1988). The violence initiation group, then, may include those women whose partners viewed the impending birth as especially threatening (Jasinski, 2001) and decreased support and increased violence are negative outcomes potentially associated with that threat. Considering the verbal aggression and violence measures, the persistent violence group scored significantly higher than either the cessation or initiation groups. Although one might expect the persistent group to score higher, it is surprising that the initiation group did not differ significantly from the cessation group; intuitively one would expect initiation of violence to be coupled with increased levels of verbal aggression. Indeed, previous research suggests that conflict may be a precursor to violence (Follingstad et al., 1990; Hyden, 1995; Sagrestano, Heavey et al., 1999). One explanation, however, may be that in the cessation group, although physical violence stops, verbal aggression may not, and may even increase as an alternative outlet to physical aggression. It would be interesting to assess conflict levels across the transition to pregnancy and parenthood, to examine whether conflict increases and eventually escalates into violence, or if, in contrast, violence starts without an initial increase in conflict. Similarly, comparisons of levels of conflict for the cessation and initiation groups across the transition to pregnancy would allow for better understanding of these processes. Information of this type would provide a concrete basis for designing appropriate interventions for men and women at the transition to pregnancy.
An alternative way to consider the data comparing the three groups is to look at the pattern for each group across measures; this might suggest how the interpersonal environment for each of these sets of couples differs. The cessation group is characterized by higher levels of support and lower levels of verbal aggression. Perhaps the men recognize that they could do harm to their offspring and decide to back off from conflict and violence, instead trying to create a more nurturing environment for their partners and future offspring. The initiation group is characterized by low levels of support and low levels of verbal aggression. This may suggest that low levels of support may be a precursor to initiation of violence. Finally, the persistent group is characterized by moderate levels of support and higher levels of verbal aggression.
Several limitations of this study should be noted, each of which limits the generalizability of the results. First, the women in this study represented a clinic sample of low-income, pregnant women of color rather than a more representative sample of pregnant women, and additionally, there was no comparison group of nonpregnant women. Second, the sample size was small (N = 197), including both women who did and did not report violence. Analyses comparing the three subgroups of women who reported violence were especially limited by small sample size (n = 43), and therefore these findings should be regarded with caution. Third, the authors chose to interview women in a face-to-face setting, which may have led to underreporting of violence. Fourth, the use of a single assessment may have resulted in missing those women who may have miscarried prior to enrolling in the study. In addition, some women may have experienced violence initiation following the interview, thus effectively putting them in the no violence category when they were in fact eventually victims of interpersonal violence. Fifth, data were not collected from other sources (e.g., the baby's father, other family members, police records) to provide additional insight into women's reports. Finally, the CTS, used to measure violence, has several limitations, most notably that it does not consider severity and consequences of violence.
In summary, the findings of this study suggest that demographic, psychological, and relationship variables are all valuable contributors to understanding domestic violence during pregnancy. They provide increased support for screening in medical settings, not just for domestic violence, but also for psychosocial variables such as negative interactions. This may serve as an indication that violence is occurring, in addition to other problems that may be occurring during pregnancy, warranting referral or intervention.
Footnotes
1.
Dropping ethnicity from the regression allowed for a larger sample size, because 6% of the sample was not African American or Latina.