
Abstract
The weeks following the birth of a child can be stressful for new mothers. Maternal stress may be increased when mothers are dissatisfied with instrumental partner support (e.g., division of childcare duties and family decision-making power). The purpose of the current study was to determine if there is an association between dissatisfaction with partner support and maternal stress in the postpartum period, and to examine whether that association is mediated by demand-withdraw communication between partners. Participants were 49 women who completed questionnaires about satisfaction with partner support, female demand/male withdraw communication in their relationship, and their own perceived stress approximately 8 weeks after giving birth. Findings support the hypothesis that demand-withdraw communication mediates the association between dissatisfaction with partner support and maternal stress. This finding suggests that fathers' withdrawal in the context of mothers' requests for discussion or change appears to be associated with increased levels of maternal stress.
Stressful events that occur after childbirth can impair mothers' physical health and psychological well-being (Affonso, 1992; Kline, Martin, & Deyo, 1998; Simpson, Rholes, Campbell, Tran, & Wilson, 2003; Tulman, Fawcett, Groblewski, & Silverman, 1990). There is evidence to suggest that women may experience more life stress after the birth of their child than during pregnancy (Goldstein, Diener, & Mangelsdorf, 1996), and this postpartum stress may adversely affect the functioning of women as they transition to motherhood. The current study explores psychosocial causes of maternal stress that may be salient during the transition to motherhood. Specifically, a mediational model is proposed and tested in which dissatisfaction with partner support leads mothers to engage in a pattern of demand/withdraw interactions with their partners, which in turn elevates their perceived stress in the postpartum period.
Maternal Stress
Women often feel overwhelmed and unprepared for the demands of young children (Francis-Connolly, 2002). Although postpartum stress is sometimes attributed to hormonal changes or the physical demands placed on the mother during and immediately after childbirth (Ugarriza, 2002), there is some evidence to suggest that stress and psychiatric morbidity are greater during the third and fifth postnatal weeks than during the first (Hung & Chung, 2001). This suggests that postpartum stress may be a consequence of factors other than the physiology, physical pain, or fatigue related to the birthing process. Although specific stressors vary among women from different cultural, geographic, and socioeconomic strata, many women experience stress generated by searching for adequate childcare, transitioning to the parenting role, and navigating changes in relationships. Stressors associated with motherhood lead women to feel psychological distress associated with ambivalence, conflict, and loss of self (Davies & Welch, 1986). After the birth of a child, mothers tend to report more stress and depression, and less self-esteem, compared to fathers (Pancer, Pratt, Hunsberger, & Gallant, 2000).
Researchers and feminists have argued that a variety of accepted parenting practices serve to increase the burden women feel as they navigate motherhood in today's society (e.g., Cappuccini & Cochrane, 2000). Among the most stressful are the demands placed on women to serve a double shift as both mothers and providers. The dynamics of romantic relationships often change after the birth of a child, and new mothers may bear the primary burden of childcare tasks while managing restrictions due to breastfeeding and/or physical complications of the birth, such as the pain of a cesarean section. This may be coupled with a relative lack of power regarding family decision making. Thus, mothers may find that the postpartum period is characterized by an increase in responsibilities and a decrease in flexibility and relationship power.
Maternal stress during the first year after childbirth is associated with poorer mother−infant relationships and less sensitive caregiving by the mother (Hiester & Sapp, 1991; Pianta & Egeland, 1990). The impact of maternal stress on the child during the first years of life has also been well documented. For instance, exposure to early maternal stress has been linked to elevated cortisol levels, decreased attention regulation, difficult temperament, and greater behavior problems in children (Essex, Klein, Cho, & Kalin, 2002; Huizink, Robles de Medina, Mulder, Visser, & Buitelaar, 2002; Kofman, 2002).
Partner Support
One factor that may decrease maternal stress in the postpartum period is partner support. Postpartum mothers typically list their partners as primary sources of support and this support often has a large influence on maternal well-being and adaptation to motherhood (Cox, Owen, Lewis, & Henderson, 1989; Crnic, Greenberg, Ragozin, Robinson, & Basham, 1983; Levitt, Weber, & Clark, 1986). Arizmendi and Affonso (1987) found that one of the most intense stressors for women during the perinatal period involved issues related to their partner. Low levels of perceived partner support and partner intimacy have been linked to maternal stress in the period after childbirth (Affonso, Mayberry, & Sheptak, 1988; Mulsow, Caldera, Pursley, Reifman, & Huston, 2002). Partner support may include balanced involvement in family decision making, assistance with child-care duties, and emotional support (Bost, Cox, Burchinal, & Payne, 2002; Too, 1997).
Satisfaction with family decision making (e.g., how time is spent in the house, which leisure activities are pursued by the family) appears to be especially important during the transition to parenthood, when overall relationship satisfaction often declines (e.g., Wadsby & Sydsjoe, 2001). Satisfaction with involvement in decision making is particularly relevant given that divergent perspectives about parenting roles are a common source of conflict in marital relationships (Kluwer, Heesink, & Vande Vliert, 1996; Parke, 1995). Most women (75%) in one sample reported that their responsibility for housework had increased after childbirth and that they were doing most of it themselves (Cappuccini & Cochrane, 2000).
Childcare tasks are among the greatest stressors for mothers who report high levels of stress and low levels of relationship satisfaction (Horowitz & Damato, 1999). Husband participation in childcare tasks is an important determinant in how mothers perceive their roles (Renk et al., 2003). Although fathers who perceive their marriages more positively tend to be more involved in childcare (Cox, Paley, Burchinal, & Payne, 1999), in general mothers continue to provide more direct childcare than fathers (e.g., Bond, Galinsky, & Swanberg, 1998). Cappuccini and Cochrane (2000) found that 75% of men and women reported that childcare was done primarily by the woman in couples.
Poor relationship functioning has a negative impact on mothers' and fathers' parenting behavior (e.g., Cox et al., 1999; Kerig, Cowan, & Cowan, 1993; Paley, Cox, Harter, & Margand, 2002) and children's functioning (e.g., Howes & Markman, 1989; Jouriles, Farris, & McDonald, 1991). Mothers in problematic marriages are more likely to report a sense of their own poor parenting competence and more negative perceptions regarding their infants, and these mothers exhibit poorer mother-child attachments (Coyl, Roggman, & Newland, 2002; Isabell, 1994; Knauth, 2000; Richardson, 1987; Simpson et al., 2003; Weingarten, Baker, Manning, & Kutzner, 1990).
Problem-Solving Communication
Discontent with level of partner involvement in childcare and family decision making may lead mothers to attempt to engage their partners in discussions toward change. Women are more likely than men to promote effective joint problem solving in managing the transition to parenthood (Cox et al., 1999). However, there are times when the process of problem solving can be described as a “demand-withdraw” pattern wherein one partner pressures the other for change (sometimes with complaints or criticisms) while the other partner withdraws, becomes defensive, or is passive (Christensen, 1987). This pattern is distinguishable from general negative feelings about the relationship, yet it is related to negative outcomes (Bodenmann, Kaiser, Hahlweg, & Fehm-Wolfsdorf, 1998; Caughlin, 2002; Caughlin & Huston, 2002; Caughlin & Vangelisti, 1999; Gottman & Krokoff, 1989; Schaap, Buunk, & Kerkstra, 1988; Vogel, Wester, & Heesacker, 1999).
Although the term demand often has negative connotations, the demanding behavior that takes place in demand-withdraw interactions may simply indicate that one partner is trying to begin a discussion with the other. Although the demanding style of communication maybe more noticeable because it is more active than withdrawal (by definition), the negative affect pattern may easily begin with one partner disengaging or withdrawing, resulting in the other partner demanding conversation or change. This type of interaction may spark a cycle wherein the more one partner continues to solicit the other's involvement, the more the solicited partner withdraws. This leads to the couple growing more polarized and less satisfied with the relationship.
Researchers have found an overall tendency for women to initiate problem-solving conversations more often, whereas men tend to be more withdrawing (Caughlin, 2002; Caughlin & Huston, 2002; Caughlin & Vangelisti, 1999, 2000; Christensen & Heavey, 1990; Heavey, Layne, & Christensen, 1993; Vogel et al., 1999). It stands to reason that women may desire more change than men, given that the social structure is designed so that women have less access to opportunities and rewards (Goodrich, 1991). Indeed, Christensen and Heavey (1990) suggest that women's roles as demanders may result from their power-down position in the social structure rather than any inherent gender difference in demanding behavior. For instance, men are more likely to hold positional power, including a greater ability to exert influence through status and access to and control over economic resources (Blanton & Vandergriff-Avery, 2001). Consequently, men may be able to ignore or withdraw from conflict with less cost to economic and societal security compared to their disadvantaged female counterparts. Noller (1993) has suggested that withdrawing may be a method for men to get their way when they are not prepared or willing to change their position, which ultimately allows them to maintain independence and control in relationships.
Given the extant literature, we posited that partner support (specifically, participation in childcare duties and the promotion of joint decision making about family matters) would be especially salient in the weeks following childbirth. We predicted that a lack of adequate partner support (as defined by the mother) would lead to maternal stress. Moreover, we expected that in some couples, partners who were perceived as unsupportive would also be perceived as withdrawers from conversations when mothers requested change. We predicted that this combination of inadequate support and an inability or unwillingness to discuss change would mediate the relationship between perceived partner support and maternal stress. More specifically, for the current study, we hypothesized that: (a) postpartum mothers' dissatisfaction with partner support would be associated with increased likelihood of female demand/male withdraw communication, which in turn would be associated with maternal stress; (b) dissatisfaction with partner support would independently correlate with maternal stress; and (c) demand-withdraw communication would mediate the relation between support dissatisfaction and maternal stress. This would imply that when the demand-withdraw variable is included in regression analyses, support dissatisfaction would no longer be significantly associated with maternal stress.
METHOD
Participants
Women were approached for inclusion in a larger research study investigating relationship functioning during the perinatal period (Lynch, 1996). Of the 79 women who took part in the larger study 49 provided complete data for the questionnaires used in the current study. Recruitment took place in 1994–1995 in Ohio, at two community obstetric private practice offices, one community hospital outpatient clinic, and six different childbirth classes located at a community hospital. All participants were at least 18 years old (mean age 28 years) and were Caucasian. The women in this study were assessed approximately 8 weeks after they had given birth (M = 7.81; SD = 2.56, range 6 to 18 weeks). This was the first child for 39% of the sample and other mothers had up to three additional children. Participants were not compensated.
All participants were involved in a heterosexual, cohabiting marital or common-law relationship. Couples had been together at least 1 year and up to 15 years (M = 5.35 years; SD = 3.12). Mean level of education for participants was 15 years, and the mean income for the couples was $40,000 to $50,000 per year. Seventy-five percent of participants reported that they carried medical insurance, 16% were on public assistance, and 9% self-paid their medical bills.
Measures
Maternal stress.
We used the Perceived Stress Scale (PSS; Cohen, Kamarck, & Mermelstein, 1983) to measure the degree to which participants experienced their life as uncontrollable, overwhelming, and unpredictable. This 14-item scale assesses cognitions and emotions related to global stress (rated on a 5-point scale as occurring never to very often), rather than measuring specific, objective life events. The PSS has been shown to predict depressive and physical symptomatology better than life-event scales, and it has the potential to detect stress from ongoing circumstances, from events experienced by friends and family, and from events not listed in scales of objective occurrences (Cohen et al., 1983). The scale demonstrated good reliability (Cronbach's α = .90) in the current study.
Partner support dissatisfaction.
The Who Does What? scale (WDW; Cowan, Cowan, Coie, & Coie, 1978; Cowan, Cowan, & Coysh, 1983) was designed to assess the relative involvement of each partner in family decision making and family tasks. Each item is rated on a 1–9 scale for “How it is now” and “How I'd like it to be,” with 1 indicating primary involvement by the female partner and 9 indicating primary involvement by the male partner. A rating of 5 indicates that both partners are involved about equally. The WDW has good psychometric properties (Whisman & Jacobson, 1989). We measured WDW items related to mothers' satisfaction with family decision making and childcare but eliminated items that would not apply to parents of newborns (e.g., disciplining the child or arranging the child's play visits with friends). We derived the index for Dissatisfaction with Partner Support (DPS) by summing the absolute discrepancies between “How it is now” and “How I'd like it to be,” as suggested by Cowan and Cowan (1988). This index evaluates levels of dissatisfaction with instrumental support but does not measure dissatisfaction with partner's emotional support. For example, participants rated their current and desired level of participation in cleaning and bathing their child, getting up at night with the child, and deciding how time is spent out of the house. We used the modifications suggested by the authors of the WDW (Cowan & Cowan, 1988), which incorporated additional items (primarily about childcare tasks). The resulting scale of 38 items had an α of .92.
Demand-withdraw.
The Communication Patterns Questionnaire-Revised (CPQ-R; Christensen, 1987, 1988; Christensen & Sullaway, 1984) is a self-report measure that was administered to assess dyadic communication. All items are rated on a 9-point scale, ranging from Very unlikely to Very likely. For the current study, the CPQ-R was used to assess mothers' perceptions of communication when a relationship problem arises and during the discussion of such a problem. Only the female demand−male withdraw communication (FDMW) subscale was analyzed in the current study. This subscale has been shown to discriminate happy and unhappy couples, whereas the complementary subscale (male demand−female withdraw) does not (Noller & White, 1990). The FDMW subscale consists of six items that assess asymmetrical behaviors in which the female partner tries to engage in a discussion, pressures her partner for change, or criticizes while her partner tries to avoid discussion, becomes silent, refuses to discuss the matter, or defends himself. In the current study, α for the subscale was .77.
Procedure
Potential participants were initially contacted during a routine obstetric office visit or while attending a prenatal class. After participants gave birth, they were sent packets of questionnaires in the mail. These packets included the measures described in the current study and other questionnaires used in the larger study. Participants completed the questionnaires at home and returned them within 2 weeks.
RESULTS
Descriptive Statistics and Correlations
Descriptive statistics and correlation coefficients of the predictor variable (dissatisfaction with partner support; DPS), mediating variable (demand-withdraw), and criterion variable (maternal stress) are presented in Table 1. The means and standard deviations for these measures closely approximate those of other published nonclinical samples (Cohen et al., 1983; Kohn, Lafreniere, & Gurevich, 1991; Noller & White, 1990). As expected, DPS, demand-withdraw, and maternal stress were moderately and significantly correlated with one another.
Pearson Correlation Coefficients and Descriptive Statistics for Predictor, Mediating, and Criterion Variables (N = 49)
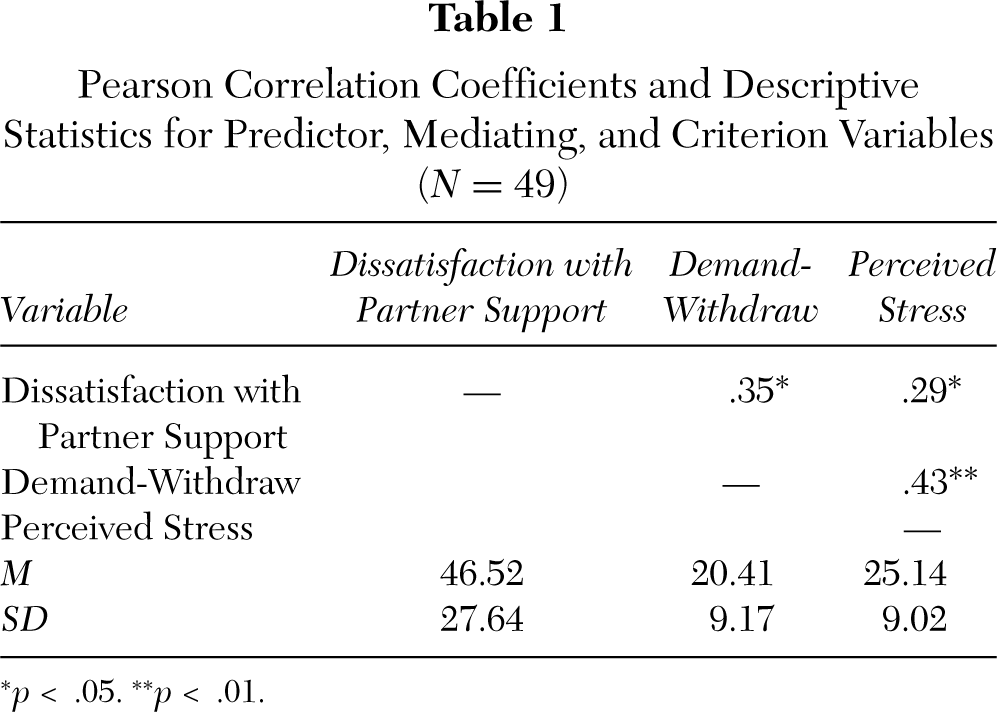
p < .05. ∗∗p < .01.
Mediational Path Analyses
The data obtained in the present study are cross-sectional and thus causal pathways cannot be determined. However, Baron and Kenny (1986) provide a useful model for testing potential mediators in a three-variable system. They suggest that a variable may serve as a mediator when it satisfies four criteria: (a) changes in the ratings of the independent variable (in our case, DPS) account for changes in ratings for the proposed mediator (in our case, demand-withdraw communication); (b) changes in the proposed mediator (demand-withdraw) account for changes in the dependent variable (in our case, maternal stress); (c) changes in the independent variable (DPS) account for changes in the dependent variable (maternal stress); and (d) the association between the independent variable (DPS) and the dependent variable (maternal stress) is no longer significant when the mediator (demand-withdraw) is included.
To test the present model for mediation based on Baron and Kenny's (1986) proposal, four multiple regression analyses were conducted. Potential confounding variables (participants' age and education, couples' income, length of relationship, and number of children) were not significantly correlated with the other measures of interest, and therefore these variables were not included in subsequent analyses. To test Baron and Kenny's (1986) first criterion, demand-withdraw (the mediating variable) was regressed on DPS (the independent variable). This model was significant, F(1, 47) = 6.71, p < .05. As hypothesized, dissatisfaction with partner support significantly predicted demand-withdraw communication, accounting for 13% of the variance in that variable.
To test the second criterion, the association between the mediator variable (demand-withdraw) and the dependent variable (maternal stress) was examined. Thus, maternal stress was regressed on demand-withdraw. This model was also significant, F(1,47) = 10.91, p < .01. Demand-withdraw significantly predicted maternal stress, accounting for 19% of the variance, as posited.
To test the third criterion, maternal stress scores were regressed on DPS scores to determine if the independent variable (DPS) significantly predicts the dependent variable (maternal stress). This regression model was significant, F(1,47) = 4.43, p < .05. Consistent with the hypotheses, dissatisfaction with partner support significantly predicted maternal stress, accounting for 9% of the variance.
Baron and Kenny's (1986) fourth and final test for mediation is to showthat the independent variable (DPS) will no longer significantly predict the dependent variable (maternal stress) when the mediating variable (demand-withdraw) is included in the model. To test this, maternal stress was simultaneously regressed on demand-withdraw and DPS. This regression was significant, F(2,46) = 6.14, p < .01, and accounted for 21% of the variance in maternal stress. As hypothesized, demand-withdraw remained significant over and above the effects of dissatisfaction with partner support (β = .43, p < .01), and uniquely accounted for 19% of the variance in maternal stress. Consistent with the model, participants' dissatisfaction with partner support no longer significantly predicted maternal stress when demand-withdraw was included in the model (β = .16, p = ns). Figure 1 illustrates the entire mediational model.
Test of the Mediated Effect
The causal step test described by Baron and Kenny (1986) is necessary, but not sufficient, to confirm a mediated effect, because it provides no direct significance test of the entire mediated pathway. MacKinnon, Lockwood, Hoffman, West, and Sheets (2002) recommend adding to the previous analyses a test of the joint significance of the pathways involved to provide a more complete test of mediation. MacKinnon et al. (2002) found that the test of mediation with the highest power and most accurate Type 1 error rate is a test of the product of regression coefficients divided by its standard error. This test statistic is designated z' because it uses an empirically established sampling distribution that differs from the normal distribution. MacKinnon, Lockwood, and Hoffman (1998) determined that the empirical critical value for z' at the .05 significance level is .97. Our final test of the mediated effect determined that z' = 2.04, p < .05, indicating that the combined effect of dissatisfaction with partner support on demand-withdraw and of demand-withdraw on maternal stress significantly differed from zero. This finding, in conjunction with the earlier path analysis, satisfies a more strict evaluation of mediation.
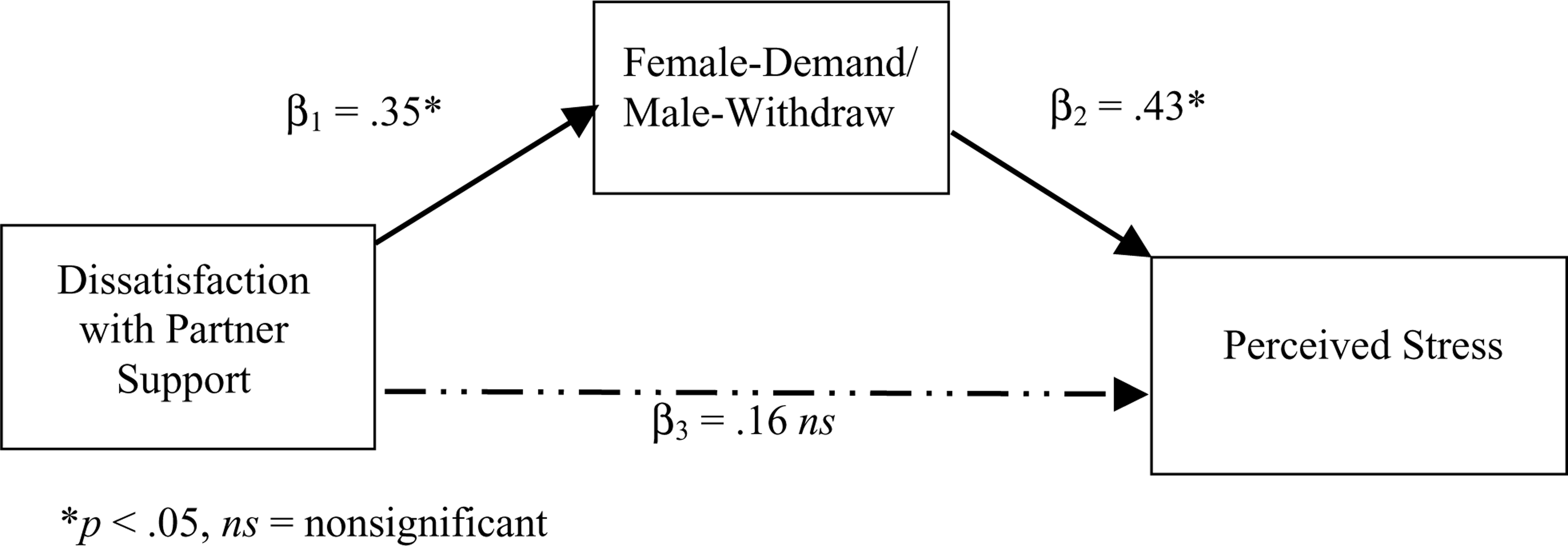
Standardized regression coefficients for the pathways among dissatisfaction with partner support, female-demand/male-withdraw, and perceived stress.
DISCUSSION
The results from this study provide support for a fully mediated model of relationship functioning in which postpartum women's perceptions of demand-withdraw interactions mediate the association between their dissatisfaction with instrumental partner support (for family decision making and family tasks) and their perceived stress. The proposed model met each of the criteria described by Baron and Kenny (1986) and satisfied the more stringent test of joint significance described by MacKinnon et al. (2002). To our knowledge, this study presents the first test of the relationships among these three constructs (dissatisfaction with partner support, female-demand/male-withdraw, and maternal stress) in a sample of postpartum women.
Postpartum mothers may feel especially overwhelmed by the sudden demands of a new or extended family, and maternal stress may be exacerbated by partners who wield greater decision-making power yet make inadequate contributions to childcare. We found that when postpartum mothers experience dissatisfaction with their decision-making power and with childcare support from their partners, it is likely that the couple engages in female demand−male withdraw communication. This result lends support to a social structural view of the tendency for women to request relationship change while men withdraw in problem-solving discussions. We have argued that this pattern evolves not from sex-determined traits, but from women's less powerful position in the traditional structure of marriage (Christensen & Heavey, 1990). Indeed, research shows that women are burdened with household and childcare duties more than men even when both spouses are employed fulltime and in equal status careers (Biernat & Wortman, 1991; Bond, Galinsky, & Swanberg, 1998; Jacobson, 1983). Fathers may withdraw from mothers who are soliciting change in an effort to passively maintain the status quo (Jacobson, 1983). The result may be a postpartum period characterized by maternal stress.
Considering the impact of postpartum stress on mothers' mental health, children's development of attachments, and future family adjustment, programs that prevent or intervene in this detrimental cycle may be beneficial for expectant parents. Feinberg (2002) has suggested that the birth of a child provides an excellent opportunity for teaching parents new skills and possibly preventing maladaptive relationship behaviors. Education about heightened maternal stress and the importance of partner support in terms of childcare and family decision making during the weeks following childbirth could better prepare new parents and ward off ineffective communication patterns. In addition, new parents may benefit from learning about conflictual interactions that may result from the stresses of early parenthood. It is possible that dissatisfaction with partner support may cause less maternal stress once couples are taught effective methods of communicating about that dissatisfaction. Learning appropriate ways to meet one another's needs may lead to less confusion, smaller power differentials, and better relationship adjustment for both partners (Rosenbluth & Steil, 1995).
Attempts at improving relationship communication may have little effect, however, if men continue to retain greater power relative to women in our society. This gender inequality may create a type of double bind for new mothers who perceive partner support as unsatisfactory, such that attempts to change the relationship lead to more intense demand-withdraw interactions. Some fathers may be especially resistant to changes, such as those with traditional views about helping mothers with housework and parenting while allowing family decisions to be shared. This underscores the need for increased awareness about the importance of joint, equal involvement in childcare and family decision making. Efforts aimed at improving individual relationships will have limited utility until the many factors associated with the oppression of women (e.g., underrepresentation in positions of power, the glass ceiling effect, de facto gender discrimination in institutional policies) are acknowledged and eliminated through efforts of both men and women.
Several factors limit conclusions and/or the generalizability of the results of the present study and suggest directions for future research. As stated earlier, the cross-sectional nature of the study prevents the determination of causal pathways. In addition, the sample was Caucasian, heterosexual, and predominantly well educated, and the present findings may not apply to other populations. Women from other racial, ethnic, or socioeconomic backgrounds and those with other sexual preferences may face different stressors associated with childbirth, including different family dynamics, discrimination, role expectations, and employment demands. Our sample size also limited comparisons between first-time mothers and mothers who had other children. Although our results did not appear to be affected by number of children, a larger sample size may have allowed for meaningful comparisons between primapara mothers and multipara mothers.
It is important to note that our measure of partner support was limited to mother's reports of satisfaction with her partner's contributions to family decision making and child-care tasks. It is quite possible that if other components of partner support or overall relationship satisfaction were included, our results would have been altered. Global relationship dissatisfaction or dissatisfaction with emotional support would likely lead to different expressions of the demand-withdraw pattern. Data were obtained from mothers only, which also qualifies our interpretations. However, evidence suggests that partners tend to agree on the presence of patterns in their relationship and on the separate role each member plays (Christensen & Sullaway, 1984; Cowan & Cowan, 1988; Foltz, Morse, & Barber, 1999; Heavey et al., 1993). Moreover, maternal behaviors may influence the adjustment of the couple more than paternal behaviors (Parke, 1996). Our results were also limited by the biases inherent in self-report methods. However, as compared to observing partner behaviors, self-report may encourage the report of private or embarrassing matters. In addition, when couples are observed, it is less likely that partners will withdraw from conflict even if they would do so if they were not observed (Christensen & Heavey, 1993; Kluwer, Heesink, & Van de Vliert, 1997). Nonetheless, future research would benefit from a multimethod approach, ideally obtaining self-report data from both partners, observational data, and collateral information. It will also be important to include broader measures of partner support to include satisfaction with intimacy and emotional support as well as the instrumental support measured in this study.
In summary, our results supported the hypothesis that demand-withdraw communication mediates the relationship between dissatisfaction with partner support (for family decision making and childcare tasks) and maternal stress. This finding highlights the importance of psychosocial causes of maternal stress, and it suggests that gender inequities at the societal level may be especially salient for mothers during the postpartum period. Couples who are expecting a child may benefit from counseling or education about effective versus maladaptive communication regarding desired relationship change, but such interventions may be limited until there are changes in institutional discrepancies that encourage men to withdraw from requested change.