
Abstract
Study 1 tested whether yoga practice is associated with greater awareness of and responsiveness to bodily sensations, lower self-objectification, greater body satisfaction, and fewer disordered eating attitudes. Three samples of women (43 yoga, 45 aerobic, and 51 nonyoga/nonaerobic practitioners) completed questionnaire measures. As predicted, yoga practitioners reported more favorably on all measures. Body responsiveness, and, to some extent, body awareness significantly explained group differences in self-objectification, body satisfaction, and disordered eating attitudes. The mediating role of body awareness, in addition to body responsiveness, between self-objectification and disordered eating attitudes was also tested as proposed in objectification theory (Fredrickson & Roberts, 1997). Body responsiveness, but not awareness, mediated the relationship between self-objectification and disordered eating attitudes. This finding was replicated in Study 2 in a sample of female undergraduate students. It is concluded that body responsiveness and, to some extent, body awareness are related to self-objectification and its consequences.
For over 50 years, feminist theorists have argued that women are sexually objectified in Western cultures (Bartky, 1990; de Beauvoir, 1949/1952; Lelwica, 1999). Empirical evidence has documented that women are sexually objectified more often than men in visual mass media (for a review, see Ward, 2003). For example, on prime time television programming, sexual comments are made more frequently about women's bodies or body parts, especially their breasts, compared to men's (Grauerholz & King, 1997); in television commercials, women are more frequently presented as sex objects (Lin, 1998); in music videos, women are more often the recipient of sexual advances (Sommers-Flanagan, Sommers-Flanagan, & Davis, 1993); and, even in Microsoft clip art, women are portrayed wearing more revealing clothing than men (Milburn, Carney, & Ramirez, 2001). In everyday situations, women are more likely to be gazed at and sexually objectified (Hall, 1984; Swim, Hyers, Cohen, & Ferguson, 2001).
Research also suggests physical appearance is more strongly related to women's than men's social and economic experiences. Physical attractiveness correlates more highly with dating experiences (Davis, 1990; Smith, Waldorf, & Trembath, 1990) and spouse's marital satisfaction (Margolin & White, 1987) for women compared to men. In addition, less attractive or overweight women, but not men, experience lower educational and economic achievements (Crandall, 1991; Crandall, 1995) and more job discrimination (for a review, see Fredrickson & Roberts, 1997; Marlowe, Schneider, & Nelson, 1996).
Researchers have examined the impact of sexual objectification on the way women experience their own bodies. In general, these theorists posit that women learn to objectify their own bodies as an outside observer might. For example, McKinley and Hyde (1996) developed the Objectified Body Consciousness Scale to measure the degree of surveillance of the body's appearance, internalization of cultural standards of female beauty, and beliefs that women can control their appearance to conform to existing standards of beauty. Similarly, Franzoi (1995) argued that women learn to view their bodies as objects of others' attention, or “body-as-object,” whereas men conceive of their bodies as instruments of action, or “body-as-process.”
An increasingly prominent theory proposed by Fredrick-son and Roberts (1997), Objectification Theory, details an array of mental health risks women face as a result of sexual objectification. These authors also argue that women are socialized to view themselves as objects of evaluation, a phenomenon they refer to as “self-objectification.” They define self-objectification as a form of self-consciousness, which leads to “a vigilant monitoring of the body's outward appearance,” and is associated with asking oneself, “how do I look?” rather than “how do I feel?” or “what can I do?” (Fredrickson, Roberts, Noll, Quinn, & Twenge, 1998). Over time, recurring states of self-objectification are thought to lead to negative psychological outcomes. Theorized acute effects include increased feelings of shame (upon realizing that one's appearance does not meet cultural standards of female beauty); diminished awareness of internal states, including bodily sensations and emotions (due to habitual monitoring of outward appearance); and reduced peak motivational states. In turn, accumulations of these experiences may account for disproportionate rates of eating disorders, depression, and sexual dysfunction in women. In order to protect against self-objectification, the authors prescribe sports participation, physical activity, and related risk taking for girls and women to “experience their bodies in more direct and positive ways” (Fredrickson & Roberts, 1997, p. 198) and “with a sense of efficacy and empowered subjectivity” (Fredrickson et al., 1998, p. 281).
A growing body of research supports several components of objectification theory. First, four experimental studies manipulated self-objectification in the laboratory and found that a self-objectified state increases feelings of shame and other negative emotions (Calogero, 2004; Fredrickson et al., 1998; Gapinski, Brownell, & LaFrance, 2003; Roberts & Gettman, 2004), reduces performance on a math test suggesting interference with processes of attention (Fredrickson et al., 1998; Gapinski et al., 2003), and leads to restrained eating compared to a control condition (Fredrickson et al., 1998). Furthermore, these findings apply to women but not men (Fredrickson et al., 1998; Roberts & Gettman, 2004). Second, cross-sectional studies report that higher levels of trait self-objectification are associated with greater body shame and disordered eating symptoms in women, with body shame mediating the relationship between self-objectification and disordered eating (Fredrickson et al., 1998; Miner-Rubino, Twenge, & Fredrickson, 2002; Noll & Fredrickson, 1998; Tiggemann & Slater, 2001). Self-objectification has also been related to symptoms of depression and anxiety (Miner-Rubino et al., 2002; Muehlenkamp & Saris-Baglama, 2002).
However, two postulates of objectification theory, which involve the concept of body awareness, have not been supported in recent studies. First, increased physical activity, which is thought to promote a direct bodily experience, has not been linked to lower levels of self-objectification and body shame as predicted. In a survey study, Parsons and Betz (2001) found that the extent of sports participation and physical activity among college women were unrelated to levels of self-objectification and associated with greater body shame. Indeed, other studies suggest that more sports participation and exercise are positively related to the consequences of self-objectification. Athletes (Burckes-Miller & Black, 1988; Zucker et al., 1985), joggers (Richert & Hummers, 1986), dancers and gymnasts (Rosen & Hough, 1988), and undergraduate students who regularly exercise (Wolf & Akamatsu, 1994) report dissatisfaction with their physical appearance and disordered eating patterns. Moreover, a recent meta-analysis concluded that college-level athletes report more eating problems than controls (Smolak, Murnen, & Ruble, 2000). These studies suggest that physical activity does not necessarily reduce self-objectification and its consequences.
Interestingly, few studies have investigated the effects of mind-body exercises. Yoga, a now popular form of mind-body exercise in the West, cultivates a direct experience of the body, which may be particularly effective in counteracting self-objectification and its consequences. Yoga entails moving the body mindfully through a series of poses, as well as stretching and balancing the body while in a single pose. Although yoga has many physical health benefits (including increased strength, flexibility, and balance), the underlying goal is to unify mind and body, in part, by immersing oneself in subtle sensations of the body (Shiffmann, 1996). Practitioners are instructed to attend to felt-bodily sensations before, during, and after a pose. Mirrors are often excluded from yoga studios, in contrast to fitness centers and dance studios, in order to encourage movement based on internal awareness rather than outward appearance. In testing whether yoga practice is associated with increased body awareness, Rani and Rao (1994) found that participants who underwent 3 months of yoga practice reported greater awareness of bodily processes compared to a nonrandomized control group who did not receive any instructions.
In addition to body awareness, yoga emphasizes responsiveness to bodily sensations. According to Shiffmann (1996), a large part of the skill in yoga lies in sensing just how far to move into a pose. If one does not move far enough, there is no challenge for the muscles; however, going too far may result in pain or injury. Therefore, yoga practitioners learn to value their body's feedback and train in “listening” to the sensations of their bodies for guidance. Through both enhanced awareness and responsiveness, practitioners may increasingly value autonomic processes and physical abilities, thereby diminishing the importance of physical appearance to one's physical self-concept and overall sense of self.
Satisfaction with physical appearance may improve as a result of increased body awareness and responsiveness. In support of this hypothesis, Clance and colleagues found that body awareness training akin to yoga increased body acceptance among male and female undergraduates after 2 months compared to a nonrandomized control group (Clance, Matthews, & Joesting, 1979). In a second study, children experienced greater body acceptance compared to a randomized control group after 4 weeks of body awareness training and yoga exercises (Clance, Mitchell, & Engelman, 1980).
Yoga practice may also facilitate more healthy eating behaviors. By gaining sensitivity and responsiveness to bodily cues, including those of hunger and satiety, yoga practitioners may increasingly regulate food intake more based on bodily needs and less on emotional, situational, or other factors. In line with this reasoning, Kristeller and Hallett (1999) found that participation in a 6-week meditation-based intervention reduced the number and severity of binges among obese women diagnosed with binge eating disorder. In addition, in a randomized study, Telch, Agras, and Linehan (2001) found that dialectical behavior therapy, which fosters mindful awareness of moment-to-moment experience, reduced binge eating and eating pathology in participants diagnosed with binge eating disorder compared to a wait-list control condition.
Thus, one purpose of the present study was to address objectification theory's postulate that physical activity promotes a direct experience of the body and reduces self-objectification and its consequences in women. This study tested a modified version by predicting that some exercises, more than others, promote a direct experience of the body and lower self-objectification. Women who practice yoga were expected to report greater body awareness and responsiveness compared to women who practice other physical exercises. In addition, yoga practitioners were expected to report lower levels of self-objectification, body dissatisfaction, and symptoms of eating disorders.
A second aspect of objectification theory not confirmed in recent studies pertains to the effect of self-objectification on body awareness. Chronic experiences of self-objectification are theorized to diminish awareness of internal states due to the reduction of attentional resources (Pennebaker, 1982). In turn, a lack of awareness may lead to disordered eating patterns (Heilbrun & Worobow, 1990; Heilbrun & Worobow, 1991). However, in a correlational test of this hypothesis, Tiggemann and Slater (2001) measured awareness of bodily sensations using the Private Body Consciousness Questionnaire (PBCQ; Miller, Murphy, & Buss, 1981) and found no relation to self-objectification or symptoms of disordered eating in a sample of undergraduate women and former ballet dancers. In a second study, Muehlenkamp and Saris-Baglama (2002) defined internal awareness along emotional terms and measured alexithymia, an inability to identify or express emotions. Although they found correlations among alexithymia, self-objectification, and disordered eating, results did not support a mediation effect of alexithymia.
The failure of internal awareness to mediate between self-objectification and disordered eating could be due to methodological limitations of these studies. With regard to body awareness, the PBCQ used by Tiggemann and Slater (2001) is a brief measure (5 items), had a modest internal reliability (Cronbach's α = . 64), and was tested in relatively small samples. A more extensive measure of body awareness, such as the 18-item Body Awareness Questionnaire (BAQ; Shields, Mallory, & Simon, 1989), tested in a larger sample may reveal significant mediation. Second, the construct of body awareness could be expanded. Body responsiveness, as described above, broadens the construct of body awareness proposed by Fredrickson and Roberts (1997) by emphasizing how bodily sensations are valued and treated and not just whether they are perceived. Accordingly, self-objectification may reduce awareness of bodily sensations, reduce responsiveness to those sensations, or both. In turn, disordered eating may result from a lack of awareness of cues regulating food intake, a lack of responsiveness to those cues, or both. Hence, body responsiveness, in addition to body awareness, may mediate the relationship between self-objectification and disordered eating. Therefore, the second purpose of this paper was to test the relationships among self-objectification, disordered eating, body awareness, and body responsiveness. Body awareness was tested as a mediator using an alternative measure of body awareness (BAQ; Shields et al., 1989) to address methodological shortcomings in previous research. In addition, a measure of body responsiveness was created to test whether this expanded definition of internal awareness mediates between self-objectification and symptoms of disordered eating.
Study 1 compared women who were currently taking yoga classes to two groups of women not taking yoga classes. Aerobic students were chosen as a comparison group to control for possible effects of exercising in an instructor-led class. The second comparison group included women who were not taking yoga or aerobic classes in order to establish baseline values. Expected group differences in body awareness and responsiveness were predicted to account for the yoga group's lower self-objectification, greater body satisfaction, and fewer symptoms of disordered eating. In a secondary analysis, to determine whether more yoga practice is associated with greater favorable outcomes, extent of yoga practice was correlated with self-objectification and related measures in the yoga group only. In an effort to establish whether significant correlations were a function of yoga practice in particular, or more exercise in general, amount of aerobic practice within the aerobic sample was also correlated with self-objectification and related measures.
Finally, the hypothesized mediating roles of body awareness and responsiveness between self-objectification and disordered eating attitudes were tested across all exercise groups. Study 2 replicated the mediational analyses performed in Study 1 in a sample of younger women, who are more at risk for high levels of trait self-objectification and the development of eating disorders (Tiggemann & Lynch, 2001). Because the mean age of participants in Study 1 was 37 years (SD= 14.29), undergraduate female students were chosen as participants for Study 2.
STUDY 1
Method
Participants
Three groups of women participated in this study: yoga practitioners not currently taking aerobic classes (n = 43), aerobic exercisers not currently taking yoga classes (n = 45), and a baseline comparison group who had not practiced yoga or aerobics in the past 2 years (n = 51). Seventy-nine percent of the entire sample identified as White, 1.4% as African American, 9.3% as Asian American, 5.8% as Latina or Mexican American, and 4.3% did not respond. Participants ranged in age from 18 to 87 years old. The mean age of the entire sample was 37.16 years old (SD= 14.29). The three groups did not differ significantly in age. Annual income was reported on a 6-point scale as follows: 1 = under $12,000, 2 = $12,000–$24,000, 3 = $24,000–$35,000, 4 = $35,000–$50,000, 5 = $50,000–$65,000, and 6 = $65,000 and higher. The mean for the entire sample was 4.32 (SD = 1.71). The exercise groups did not differ in annual income. Thirty-seven percent of participants were married, and the exercise groups did not differ significantly by marital status.
Procedure
Potential participants were approached by the author at exercise studios, grocery stores, and shopping centers and offered $6 to complete a survey on “Women and Exercise.” Interested participants were given an envelope (with prepaid postage and return address) containing the survey packet and were asked to mail the survey back within 2 weeks to receive $6 by mail. The packet contained a brief description of the project, consent form, and survey instrument.
Yoga participants. Yoga practitioners were recruited from select Iyengar and Astanga-based classes at local yoga studios. A class was selected if the instructor emphasized body awareness, such as encouraging students to coordinate their breath with movement and to notice subtle changes in the body before, during, and after a pose. Classes were 1.5 hours long. Eighty-one percent of women who took the survey home mailed it back complete.
Aerobic participants. Aerobic practitioners were recruited from step aerobic classes held at the YMCA and a local fitness center. Classes consisted of following the movement of an instructor in time to music. Instructors spoke into microphones to guide participants through the routine. A short warm-up and stretch period preceded a 30-minute aerobic workout, followed by more stretching and a warm-down period. Classes were 45-60 minutes long. The aerobic sample had a 66% return rate.
Baseline comparison participants. The baseline comparison group was defined as women who had not taken a yoga or aerobics class in the past 2 years or participated in any mind-body activities (e.g., meditation, t'ai chi, biofeedback). This group was recruited in two ways. First, yoga and aerobic participants were asked to give a survey to a female friend or family member who had not practiced yoga or aerobics in the past 2 years. If they knew someone, they were handed a survey to pass on to them. Eleven participants were recruited in this manner (7 from the yoga and 4 from the aerobic group). Remaining participants (n = 40) were recruited from outside grocery stores and shopping centers. Potential participants were asked whether they had taken a yoga or aerobics class or participated in any mind-body related activities in the past 2 years. If they had not and were willing to participate in the study, they were given a return envelope with prepaid postage and the survey inside and asked to return it within 2 weeks to receive reimbursement by mail. Sixty-four percent of those who took a survey returned it within 2 weeks.
Measures
Participants completed the survey measures in the order presented below. The first page requested demographic information as well as height and weight to calculate body mass index. The rationale to ask for these variables first was to allow the women to become comfortable filling out the survey before answering potentially more sensitive questions. In general, the predicted measures (e.g., self-objectification) were placed before the predictors (e.g., body responsiveness) to minimize the influence of predictor variables on predicted ones.
Extent of exercise participation. Extent of exercise participation was measured in three ways. Participants were asked for how many months or years they had regularly practiced their exercise, how many hours per week they practiced on average, and at what level of proficiency they considered themselves to be: (a) beginning, (b) beginning-intermediate, (c) intermediate, (d) intermediate-advanced, (e) advanced.
Self-objectification. The Self-Objectification Questionnaire (Noll & Fredrickson, 1998) was used to measure the degree to which participants viewed their bodies in terms of observable, appearance-based (objectified) aspects versus nonobservable, competence-based aspects. Participants rank ordered 10 body attributes by how important each is to their own physical self-concept. The instructions were changed from “When considering your physical self-concept, how important is… ”to “When you think about your body, how important is… ”to clarify the meaning of the question. The 10 body attributes differ along two dimensions: appearance-based attributes, which included weight, sex appeal, physical attractiveness, firm/sculpted muscles, and measurements (e.g., chest, waist, hips) and competence-based attributes, which included physical coordination, health, strength, energy level, and physical fitness level. The rankings of the appearance-based and competence-based attributes were separately summed to create two scores. The highest ranked attribute received a score of 9 and the least important attribute received a score of 0. Then, the competence-based score was subtracted from the appearance-based score. Scores could range from −25 to +25 with higher scores indicating a greater tendency to view one's body in terms of appearance-related attributes. The measure has been shown to have sufficient convergent validity (Noll, 1996, as cited in Noll & Fredrickson, 1998). Specifically, it correlated positively (r= . 52, p < .01) with the Appearance Anxiety Questionnaire (Dion, Dion, & Keelan, 1990), a measure of preoccupation with appearance. It also correlated highly with the Surveillance subscale of the Objectified Body Consciousness Scale (r = . 63, p < .001; McKinley & Hyde, 1996) as reported by Miner-Rubino et al. (2002). Previous research also demonstrated high test-retest reliability (r = . 92; Frederickson, 1999, as cited in Miner-Rubino et al., 2002). In the present study, 13 women had missing data due to errors in following instructions (1, 6, and 6 participant(s) in the yoga, aerobic, and baseline groups, respectively) and were therefore excluded from analyses involving this variable.
Body satisfaction. Body satisfaction was measured using the Body Areas Satisfaction scale, a subscale of the Multidimensional Body-Self Relations Questionnaire, a well-validated instrument (Brown, Cash, & Mikulka, 1990). Nine items assess satisfaction with face, hair, lower torso, mid-torso, upper torso, muscle tone, weight, height, and overall appearance. Responses were recorded on a 5-point scale ranging from 1 (very dissatisfied) to 5 (very satisfied). The scale is reported to have an internal consistency of. 80 (Cash, 1989) and test-retest reliability of r= . 86 (Cash, 1994, as cited in Foster, Wadden, & Vogt, 1997). In the present study, Cronbach's α was. 80.
Eating disorder symptomatology. The Eating Attitudes Test (EAT-26; Garner, Olmstead, Bohr, & Garfinkel, 1982) is a 26-item scale, measuring cognitions, emotions, and behaviors associated with anorexia and bulimia nervosa. Responses were measured on a 6-point scale ranging from 1 (never) to 6 (always). This scale consists of three subfactors: dieting behavior, bulimic symptomatology, and anorexia nervosa symptomatology. It has been shown to differentiate between women diagnosed with an eating disorder and a comparison group of college females and is also useful as a screening instrument for the presence of disturbed eating patterns in nonclinical samples (Garner et al., 1982). Overall, the scale has an internal consistency of. 83 in a nonclinical sample using cut-off scores (Garner et al., 1982). In the present study, the measure was used as a continuous variable and Cronbach's α was. 90.
Body awareness. Attentiveness to normal, internal bodily processes and sensations was measured using the BAQ (Shields et al., 1989). The BAQ is an 18-item scale and has been shown to be internally consistent (Cronbach's α = . 82) in an undergraduate student sample. The scale consists of four factors: note responses or changes in body process (e.g., “I notice differences in the way my body reacts to various foods.”); predict bodily reaction (e.g., “When my exercise habits change, I can predict very accurately how that will affect my energy level.”); sleep-wake cycle (e.g., “There seems to be a ‘best’ time for me to go to sleep at night.”); and onset of illness (e.g., “I know I'm running a fever without taking my temperature.”). Responses were measured on a 7-point Likert scale ranging from 1 (not at all true about me) to 7 (very true about me). Higher scores indicate greater body awareness. As reported by Shields et al., the scale correlates with the PBCQ in women (r = .48, p < .01; Miller et al., 1981) but is independent of the Pennebaker Inventory of Limbic Languidness (Pennebaker, 1982), an index of the frequency with which physical symptoms are experienced, thereby demonstrating convergent and discriminant validity, respectively. Test-retest reliability over 2 weeks was good, r = .80. In the present study, Cronbach's α for the entire scale was .89.
Body responsiveness. A 7-item scale was created to measure responsiveness to bodily sensations. The 7 items were: (a) “I am confident that my body will let me know what is good for me,” (b) “My bodily desires lead me to do things that I end up regretting” (reverse coded), (c) “My mind and my body often want to do different things” (reverse coded), (d) “I suppress my bodily feelings and sensations” (reverse coded), (e) “I ‘listen’ to my body to advise me about what to do,” (f) “It is important for me to know how my body is feeling throughout the day,” and (g) “I enjoy becoming aware of how my body feels.” Responses were measured on a 7-point scale ranging from 1 (not at all true about me) to 7 (very true about me). Higher scores reflect greater body responsiveness. Cronbach's a for this measure was .83.
Results
Sample Characteristics
Current self-reported weight and height were used to calculate body mass index (BMI = kg/m2). Higher scores indicate greater body mass. Significant differences were found among the three exercise groups (see Table 1). The yoga group reported leaner body mass than the aerobic and baseline comparison groups. No differences were found between the aerobic and baseline groups. Body mass index was therefore included as a covariate in later analyses when applicable.
The yoga participants practiced an average of 4.96 hours perweek (SD = 3.19) for an average of 6 years and 2 months (SD = 87.58 months). The aerobic group practiced 3.19 (SD = 1.37) hours per week for an average of 6 years and 4.5 months (SD = 65.28 months). Eighty-six percent of participants in the baseline comparison group reported some form of regular exercise, whereas 14% reported exercising less than one hour per week for the past 2 months. Among the exercisers, 37% reported walking as their predominant form of exercise, 16% running, 8% using machines at the gym, 8% dancing, 4% biking, and 6% other. These participants reported engaging in their most frequent type of exercise an average of 4.06 hours per week (SD = 3.21) for an average of 7 years and 5.9 months (SD = 101.36 months). The three exercise groups did not differ in total months of experience, but the yoga group did practice more hours per week compared to the aerobic group, F(1, 86) = 11.62, p < .001, and the baseline group, F(1, 92) = 4.72, p < .05. With regard to level of expertise, the aerobic group reported greater experience on average (M = 3.58, SD = 1.13) compared to the yoga group (M= 3.00, SD= 1.07), F(1, 84) = 5.96, p < .05, and baseline group (M= 2.74, SD= 1.20), F (1, 84) = 11.04, p < .001. The yoga and baseline groups did not differ significantly on level of expertise.
Study 1: Means and Standard Deviations of Variables for Three Exercise Groups

Note. Means in the same row that do not share subscripts differ at p < .05.
BMI included as a covariate in the ANCOVA.
∗ p < .05. ∗∗ p < .01.
Between-Group Analyses
A one-way multivariate analysis of covariance (MANCOVA) using Pillai's Trace was used to analyze self-objectification, body satisfaction, disordered eating attitudes, awareness, and responsiveness with BMI as a covariate and exercise group as the independent variable. The MANCOVA indicated a significant effect of exercise group, Pillai's trace = . 273, F (10, 236) = 3.73, p < .001.
Follow-up analyses of variance (ANOVA) and analyses of covariance (ANCOVA) were computed to examine differences among the exercise groups. BMI was correlated with body satisfaction, disordered eating attitudes, and body responsiveness across groups (see Table 2) and, therefore, included as a covariate in the respective analyses. Univariate analyses revealed that the yoga participants reported significantly greater body awareness, responsiveness, body satisfaction, and less self-objectification than the aerobic and baseline comparison groups (see Table 1). The aerobic and baseline groups did not differ on these variables, with the exception that the baseline group reported greater body satisfaction compared to the aerobic group. For disordered eating attitudes, the yoga group reported lower scores compared to the aerobics group. The baseline group reported similar scores as the yoga group and lower scores compared to the aerobic group.
Mediational Analyses
Mediational analyses were conducted to test whether body awareness and body responsiveness accounted for the yoga group's less self-objectification, greater body satisfaction, and lower disordered eating attitudes compared to the aerobic and baseline groups. According to Baron and Kenny (1986), the following three conditions must be met before mediation can be tested: (a) the predictor variable (e.g., exercise group) must correlate with the proposed mediator (e.g., body awareness), (b) the proposed mediator must correlate with the predicted variable (e.g., self-objectification), and (c) the predictor variable must correlate with the predicted variable. If these conditions are met, the predictor variable is entered on the first step of a regression equation and the proposed mediator on the second step to predict the predicted variable. Mediation is demonstrated when the partial regression coefficient (beta weight) of the predictor variable is substantially reduced once the proposed mediator enters the equation. To test for significant reduction, the Sobel method was used (Sobel, 1982).
Study 1: Intercorrelations, Means, and Standard Deviations of Variables Across Entire Sample (N= 139)
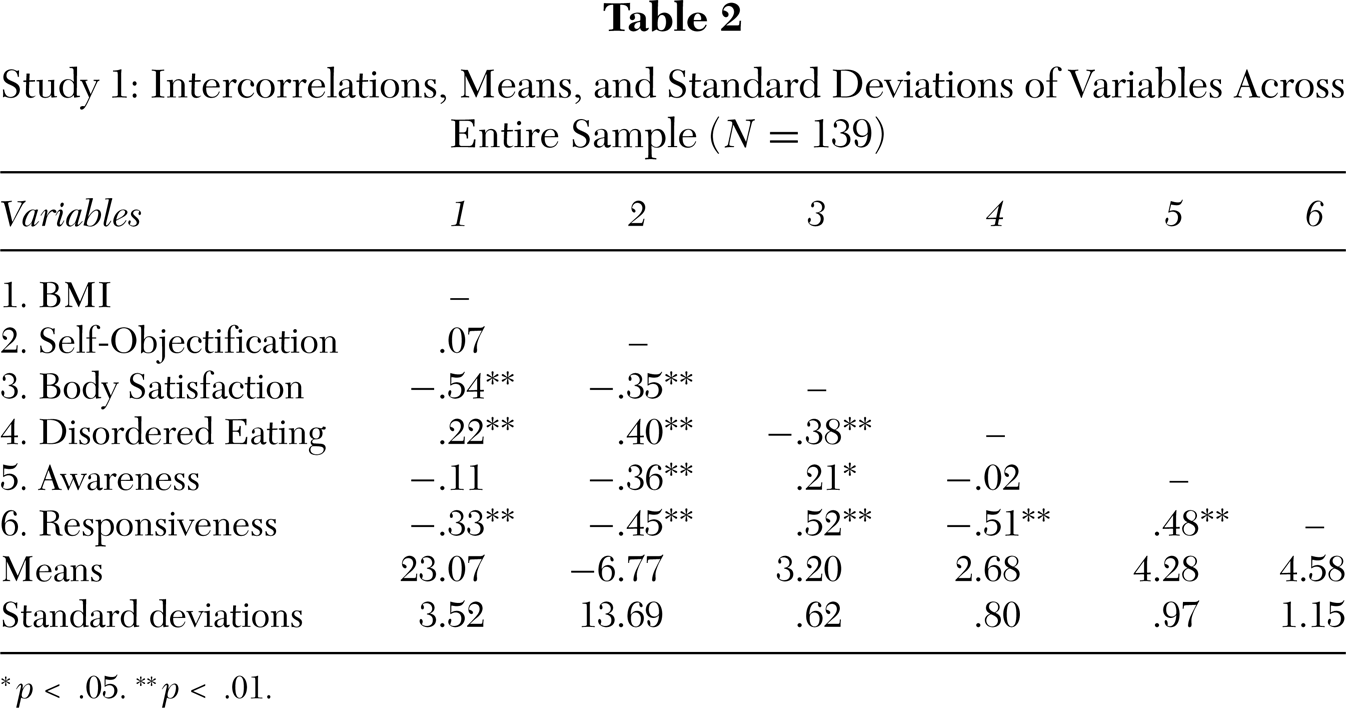
∗ p < .05. ∗∗ p < .01.
Study 1: Results of Hierarchical Regression Analyses Predicting Self-Objectification, Body Satisfaction, and Disordered Eating Attitudes (Yoga and Aerobic Groups)
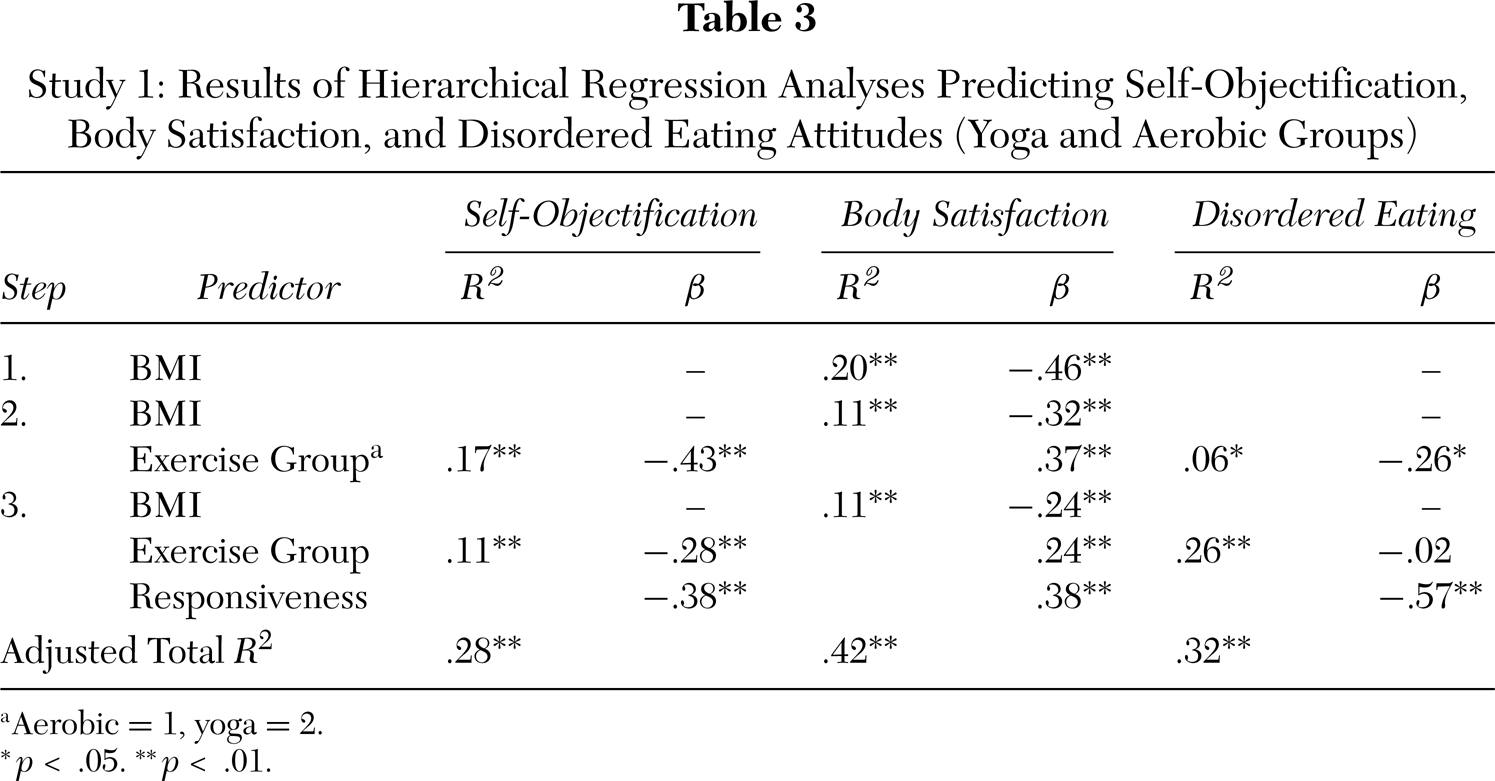
a Aerobic = 1, yoga = 2.
∗ p < .05. ∗∗ p < .01.
Two sets of hierarchical regression equations were computed: one for the yoga and aerobic groups and one for the yoga and baseline groups. Within each set, body awareness and body responsiveness were tested as mediators in separate regression equations. Exercise group was entered on the first step and either body awareness or body responsiveness was added on the second step. If BMI was correlated with the predicted variable, it was entered on the first step.
Yoga and aerobic groups. The three conditions were examined in the yoga and aerobic groups. Exercise group (aerobic = 1, yoga = 2) was significantly related to both body awareness (r = . 41, p < .01) and body responsiveness (r = . 42, p < .01), meeting the first requirement. For the second and third conditions, body awareness, body responsiveness, and exercise group were each significantly related to self-objectification and body satisfaction (p < .05). Disordered eating attitudes was related to body responsiveness (p < .05) but not body awareness (p > . 05). Therefore, the conditions were met to conduct tests of mediation for body awareness and body responsiveness for each predicted variable, except for the test involving body awareness and disordered eating attitudes. BMI was related to body satisfaction (r = −.46, p < .01) but not self-objectification or disordered eating attitudes (p > . 05). Hence, BMI was entered on the first step in the regressions that predicted body satisfaction.
The regression analysis testing whether body awareness mediated the relationship between exercise group and self-objectification showed that the beta weight for exercise group dropped from β = −.43 (p < .001) to β = −.34 (p < .01) once body awareness entered the equation (β = −. 22, p = . 05). According to the Sobel test, the reduction in the beta value was marginally significant (Z = −1.80, p = . 07). Body awareness did not mediate the relationship between exercise group and body satisfaction after BMI was entered on the first step of the equation.
Results of the regression analyses that tested the mediating role of body responsiveness are presented in Table 3. As predicted, for self-objectification, the beta weight for exercise group was reduced once body responsiveness entered the equation. Sobel's test indicated that the decrease in the beta value was significant (Z = −2.77, p < .01). For body satisfaction, after BMI was entered on the first step, the beta weight for exercise group was reduced when body responsiveness entered the equation. However, the Sobel test could not be computed for this analysis due to the inclusion of the BMI covariate. For disordered eating attitudes, the beta weight for exercise group was reduced from significance to nonsignificance once body responsiveness entered the equation. The drop in the beta value was significant (Z = −3.45, p < .01).
Yoga and baseline groups. The three conditions necessary to test for mediation of body awareness and body responsiveness in the yoga and baseline groups were examined. Exercise group (yoga = 1, baseline = 2) was correlated with body awareness (r = −.33, p < .01) and body responsiveness (r = −.33, p < .01). Body awareness, body responsiveness, and exercise group were significantly related to self-objectification and body satisfaction (p < .05); however, exercise group and body awareness were not correlated with disordered eating attitudes (p >.05). Therefore, the conditions were met to test body awareness and body responsiveness as mediators with self-objectification and body satisfaction as predicted variables, but not disordered eating attitudes. BMI was related to body satisfaction (r = −.58, p < .001) but not self-objectification (p > .05). BMI was therefore entered on the first step of the regression equations that predicted body satisfaction.
Study 1: Results of Hierarchical Regression Analyses Predicting Self-Objectification and Body Satisfaction (Yoga and Baseline Groups)
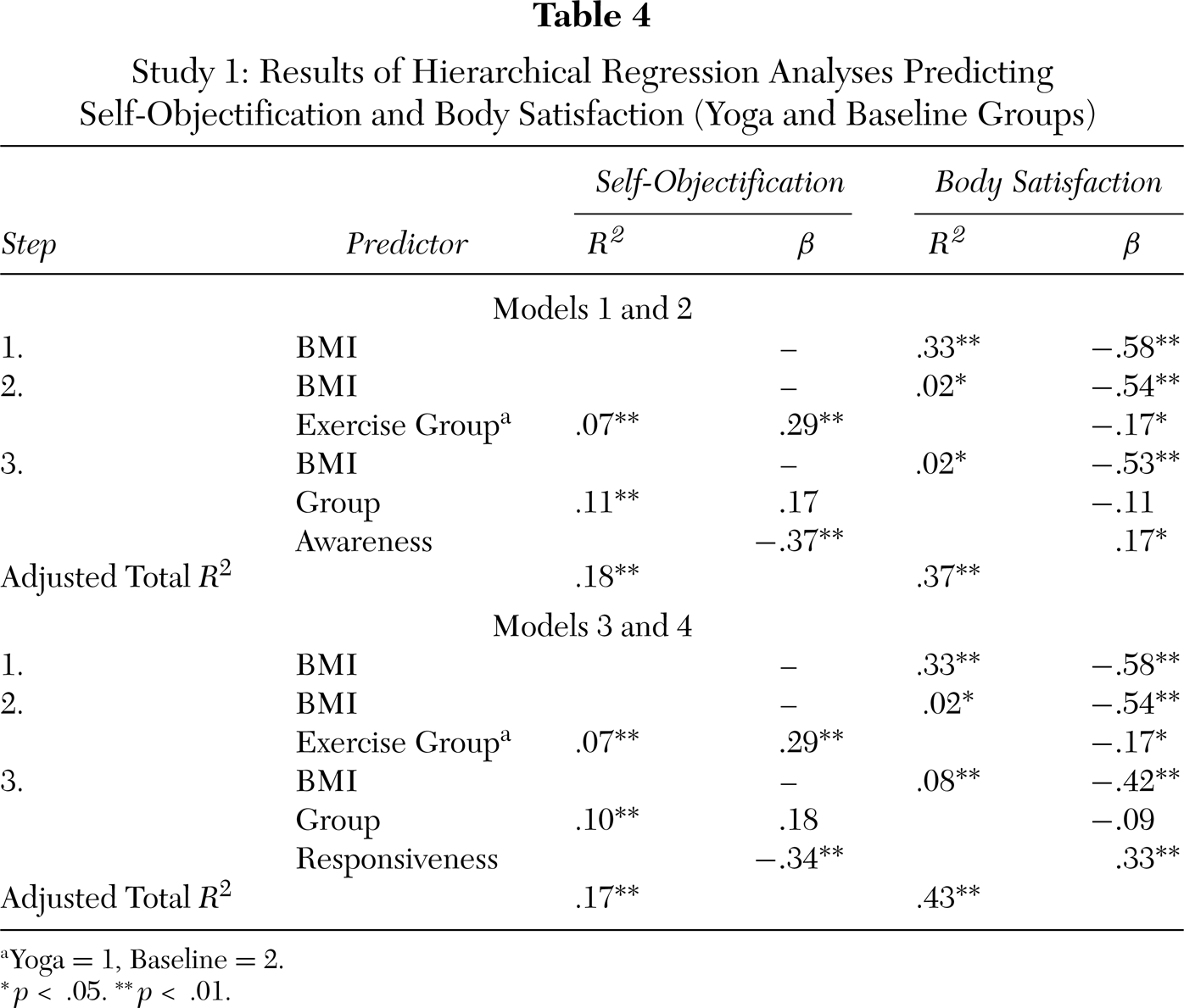
a Yoga = 1, Baseline = 2.
∗ p < .05. ∗∗ p < .01.
Results of the mediational analyses for body awareness are presented in Table 4 (Models 1 and 2). As predicted, when body awareness was tested as a mediator for exercise group and self-objectification, the beta weight for exercise group reduced from significance to nonsignificance. The Sobel test was significant (Z= 2.36, p < .05). For body satisfaction, after controlling for BMI, the beta weight for exercise group dropped from significance to nonsignificance once body awareness entered the equation. Although the Sobel test could not be computed due to the presence of the covariate, Baron and Kenny (1986) state that mediation is established when the beta weight of the predictor variable drops to a nonsignificant level.
As shown in Table 4 (Models 3 and 4), when body responsiveness was tested for mediation between exercise group and self-objectification, the beta weight for exercise group was reduced from significance to nonsignificance once body responsiveness entered the equation (Z = 2.32, p < .05). For body satisfaction, after BMI was entered on the first step, the beta weight for exercise group reduced from significance to nonsignificance once body responsiveness entered the equation.
Analyses Within Exercise Groups
To determine whether more yoga practice is associated with greater body awareness, responsiveness, body satisfaction, and less self-objectification and disordered eating attitudes, correlational analyses were conducted within the yoga group. Three measures of extent of exercise participation (i.e., total number of months, total hours per week, and level of experience) were correlated with the predicted variables. Average hours per week was negatively related to self-objectification (r = −.30, p= . 05), such that more hours spent doing yoga per week was associated with less self-objectification. After controlling for age, level of experience was positively related to body satisfaction (r = . 38, p < .05), such that greater expertise was associated with greater body satisfaction. The same analyses were conducted within the aerobic group. Average hours per week was positively associated with disordered eating attitudes (r = . 35, p < .05), such that more hours of aerobics per week was associated with greater disordered eating attitudes. No other correlations were significant (p > .05).
Analyses Across Exercise Groups
As predicted, greater body responsiveness was associated with lower self-objectification, greater body satisfaction, and fewer disordered eating attitudes across the entire sample (see Table 2). Greater body awareness was also associated with less self-objectification and greater body satisfaction, although it showed no relationship with disordered eating attitudes. Body awareness and body responsiveness were moderately correlated.
To test whether the relationship between self-objectification and symptoms of disordered eating is mediated by body responsiveness, a hierarchical multiple regression analysis was conducted across the three exercise groups. Self-objectification was entered on the first step of the equation and body responsiveness was entered on the second step. As seen in Table 5, the beta weight for self-objectification was significantly reduced once body responsiveness was included in the equation (Z = 3.98, p < .01).
Studies 1 and 2: Results of Hierarchical Regression Analyses for the Prediction of Disordered Eating Attitudes
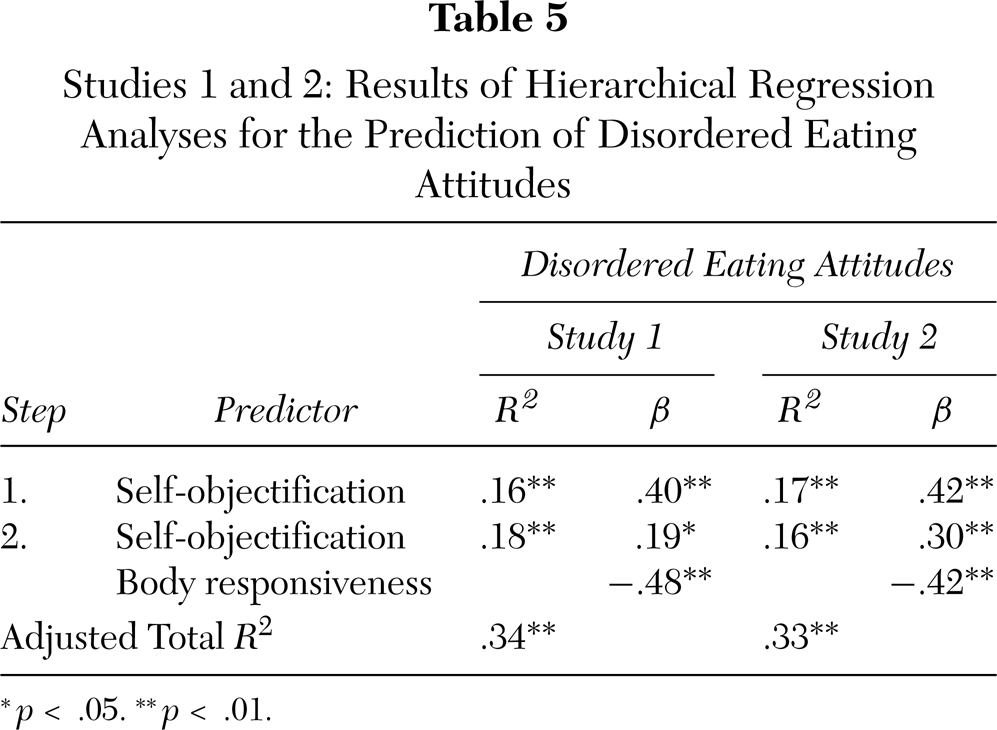
∗ p < .05. ∗∗ p < .01.
Discussion
Study 1 tested whether yoga is associated with more positive body experiences in women by comparing current yoga practitioners with aerobic exercisers and those who do not practice yoga or aerobics (i.e., baseline group). As predicted, yoga practitioners reported less self-objectification, greater satisfaction with physical appearance, and fewer disordered eating attitudes compared to nonyoga practitioners, with the exception that the yoga and baseline groups reported similar levels of disordered eating attitudes. It is important to note that these findings cannot be attributed to group differences in BMI because BMI was controlled for in the analyses.
In addition, the concept of body awareness was expanded from its original version proposed by Fredrickson and Roberts (1997) into two aspects: degree of perceptual awareness of internal bodily sensations and degree of responsiveness to them. As expected, yoga practitioners reported both greater awareness and responsiveness. In turn, the greater body responsiveness reported by the yoga participants explained their less self-objectification, greater body satisfaction, and fewer disordered eating attitudes compared to the nonyoga participants. Higher levels of body awareness also mediated the yoga group's more favorable self-objectification and body satisfaction scores relative to the baseline group. However, for the aerobic group, body awareness showed only a marginal effect of mediation for self-objectification, and no effect for body satisfaction or disordered eating attitudes. It is not clear why body awareness did not explain the greater body dissatisfaction and disordered eating attitudes in the aerobic group. A lack of body awareness is one of several factors related to the development of body dissatisfaction and eating disorders (Thompson, Heinberg, Altabe, & Tantleff-Dunn, 1999). Other factors may play a more significant role among aerobic exercisers. For instance, researchers have shown that a drive for thinness is very high among aerobic instructors and in patients with eating disorders who frequently engage in aerobic exercise (Olson, Williford, Richards, & Brown, 1996; Solenberger, 2001). In any case, these results suggest that responsiveness to bodily sensations, and not just awareness of them, may be a key factor to protect against the development of self-objectification and its consequences in women.
Further analyses confirmed that yoga is associated with lower levels of self-objectification and its proposed consequences. For yoga practitioners, greater yoga experience, in terms of number of hours practiced per week and level of expertise, was associated with less self-objectification and greater body satisfaction, respectively. These results are interesting given the concern in the literature that excessive exercisers may be at greater risk for developing eating disorders (for instance, see Brehm & Steffen, 1998; le Grange & Eisler, 1993). Among the aerobic participants this was evident: more time spent doing aerobics per week was associated with greater disordered eating attitudes. These results suggest that not all physical activities have the same relationship to disordered eating symptoms with increased participation, and some, such as yoga, may promote better eating habits with greater practice.
Lastly, this study examined objectification theory's postulate that a lack of awareness of bodily sensations may partly explain why self-objectification may lead to disordered eating (Fredrickson & Roberts, 1997). Similar to the findings of previous research, internal awareness did not meditate the relationship between self-objectification and disordered eating attitudes (Muelenkamp & Saris-Baglama, 2002; Tiggemann & Slater, 2001). However, responsiveness to bodily sensations did show strong evidence of mediation. These findings suggest that self-objectification may interfere with the ability to value and respond appropriately to bodily signals, but not mute them from conscious awareness. In turn, decreased body responsiveness may trigger disordered eating habits. However, one limitation of this finding concerns its generalizability. Because the participants in this study were considerably older than the college students participating in previous research (Muelenkamp & Saris-Baglama, 2002; Tiggemann & Slater, 2001) and others more at risk for eating disorders, there is doubt concerning the generalizability of these results. The purpose of Study2, therefore, was to address this limitation by attempting to replicate these findings in a sample of female undergraduate students, a population known to be at greater risk for self-objectification and the development of eating disorders (Tiggemann & Lynch, 2001).
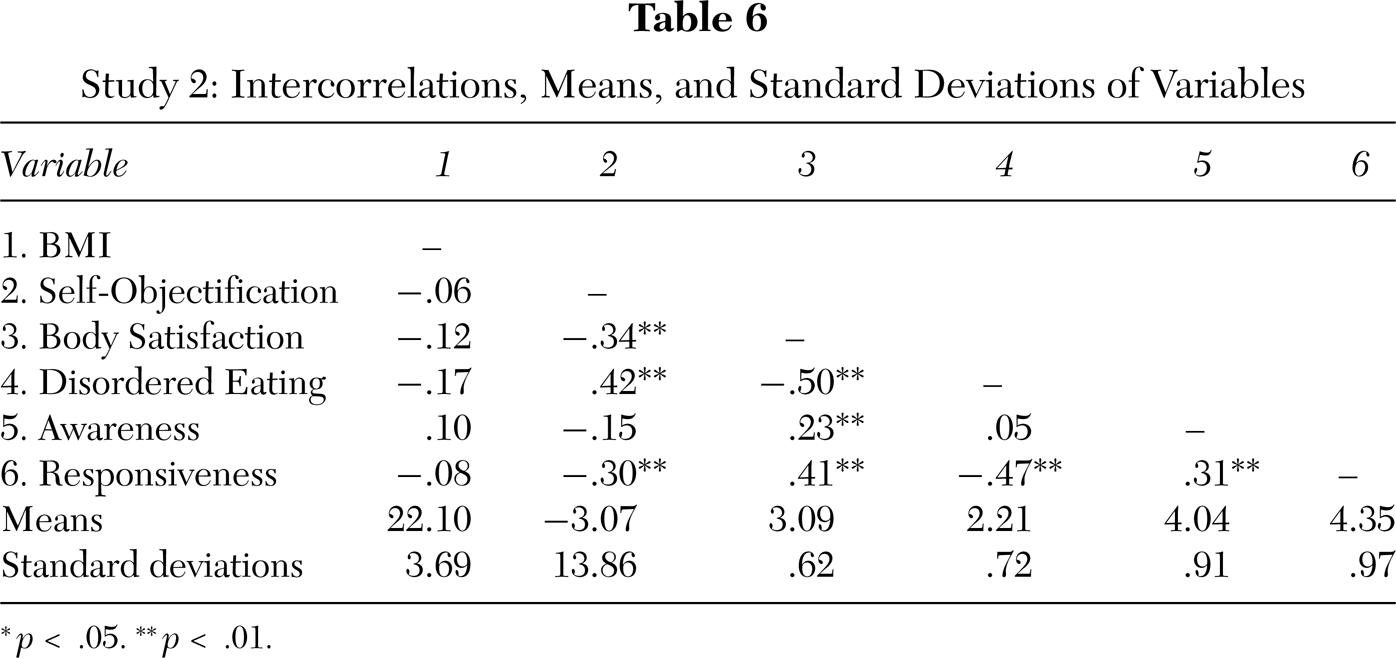
Study 2: Intercorrelations, Means, and Standard Deviations of Variables
∗ p < .05. ∗∗ p < .01.
STUDY 2
The purpose of Study 2 was to test the relationships among body awareness, body responsiveness, self-objectification, and disordered eating attitudes in a sample of female undergraduate students. Based on the results of Study 1, it was hypothesized that body responsiveness, but not body awareness, would be associated with self-objectification and disordered eating. Furthermore, it was expected that the relationship between self-objectification and disordered eating attitudes would be mediated by body responsiveness but not body awareness.
Method
Participants
One hundred thirty-three female undergraduate students (mean age = 20.46, SD = 3.96) participated in the study. Fifty-two percent of the sample identified as Asian American, 26% as White, 8% as Hispanic/Latina, 4% as African American, 8% as other, and 2% chose not to respond. Self-reported mean height was 63.73 inches (SD = 2.53) and mean weight was 127.71 pounds (SD = 22.81), resulting in an average body mass index of 22.10 (SD = 3.69).
Procedure
Participants were recruited from psychology courses and given course credit upon completion of the study. Participants completed a survey entitled “Women and Exercise.” The surveys were completed in small groups ranging from 3 to 10 participants.
Measures
The measures of BMI, self-objectification, disordered eating attitudes, body awareness, and body responsiveness used in Study 1 were used in Study 2 and presented in the same order. Cronbach's alphas for the BAQ, body responsiveness measure, and EAT-26 were. 87,. 70, and. 92, respectively.
Results
Correlations
Means, standard deviations, and intercorrelations for all variables are reported in Table 6. As predicted, self-objectification was positively related to disordered eating attitudes. Self-objectification was negatively related to body responsiveness but only marginally related to body awareness (p = . 10). Disordered eating attitudes were negatively related to body responsiveness but not to body awareness. BMI was not significantly correlated with any of the variables.
Mediational Analyses
The three conditions necessary, according to Baron and Kenny (1986), to test whether body responsiveness mediates between self-objectification and disordered eating attitudes were met (see Table 6). However, body awareness could not be tested as a mediator because it did not correlate with self-objectification or disordered eating attitudes. Therefore, only one regression analysis that tested the mediating role of body responsiveness was conducted. Self-objectification was entered on the first step and body responsiveness was entered on the second step of the regression equation with disordered eating attitudes as the predicted variable. As seen in Table 5, the beta weight for self-objectification was significantly reduced once body responsiveness entered the equation (Z = 2.69, p < .01).
Discussion
The results of Study 2 replicate the findings of Study 1 and provide some support for the tenets of objectification theory. Similar to the findings of previous research, self-objectification was significantly related to symptoms of disordered eating (Fredrickson et al., 1998; Noll & Fredrickson, 1998; Muelenkamp & Saris-Baglama, 2002; Tiggemann & Slater, 2001). Replication of this relationship provides further evidence that self-objectification may play a role in the development of eating disorders.
However, as found in Study 1 and previous research, awareness of internal sensations did not meditate self-objectification and disordered eating attitudes (Muelenkamp & Saris-Baglama, 2002; Tiggemann & Slater, 2001). In both Studies 1 and 2, body awareness did not show any relationship to disordered eating attitudes. It is perplexing why a lack of body awareness was not related to symptoms of disordered eating. One explanation concerns the relative health of both samples (both had low scores for disordered eating attitudes and self-objectification). Perhaps it is only when self-objectifying tendencies are extreme that bodily sensations become muted. To test this hypothesis, future research should examine the relationship between self-objectification, body awareness, and severity of eating disorder symptoms among those diagnosed with an eating disorder. Interestingly, in both Studies 1 and 2, body responsiveness showed significant mediation between self-objectification and disordered eating attitudes. This pattern of findings suggests that self-objectification may first diminish body responsiveness, and over time, take its toll on actual awareness of bodily sensations. Based on the results of these studies, body responsiveness appears to be an important variable to consider in future research, and, therefore, the validity of its measurement should be further established.
GENERAL DISCUSSION
Results of Studies 1 and 2 indicate that body responsiveness and, to some extent, body awareness have important implications for self-objectification and its consequences. Objectification theory states that, through a direct experience of the body, physical activity may counteract self-objectification and its consequences in women. Yoga, a mind-body exercise, was theorized to be especially effective for reducing self-objectification due to its emphasis placed on body awareness and body responsiveness. In support of this notion, Study 1 found that yoga practice is associated with greater body awareness and responsiveness, which, in turn, are associated with lower levels of trait self-objectification, greater body satisfaction, and lesser disordered eating attitudes. These results are encouraging because they suggest that yoga may be a means to reduce the internalization of a self-objectified view in girls and women. Future experimental and longitudinal research is warranted to examine the impact of yoga on self-objectification and its consequences. If positive results are found, yoga training could be incorporated into existing programs for the prevention and treatment of eating disorders.
This study also demonstrates the importance of distinguishing between body-oriented and mind-body exercises in order to understand better the complex relationship between exercise and disordered eating in women. Mind-body exercises, or exercises that explicitly encourage body awareness and responsiveness, may promote healthy eating patterns. Prior research has conceptualized physical activities varying in terms of the emphasis placed on leanness (Smolak et al., 2000) and perception as masculine or feminine (Parsons & Betz, 2001) to understand which physical activities are associated with greater body shame and eating problems. The emphasis placed on body awareness and responsiveness may be another dimension worthy of consideration.
The results of Study 1 and Study 2 provide support for the role of body responsiveness as a mediator between self-objectification and eating disorder symptoms. The concept of body awareness may need to be enlarged from its original conception (Fredrickson & Roberts, 1997) to include responsiveness to bodily sensations as well as awareness of them. Though body awareness did not mediate between self-objectification and eating disorder symptoms in the present studies, it did explain the yoga group's lower self-objectification and greater body satisfaction scores relative to the baseline comparison group. These results suggest that increasing sensitivity to awareness of bodily sensations may prove effective in minimizing self-objectification in some cases.
The most significant limitation of Study 1 is that the cross-sectional design does not permit causal inference. An alternative explanation of these results is that women who are drawn to practice yoga already experience lower levels of self-objectification, greater body satisfaction, and fewer disordered eating attitudes. Only future experimental research, which randomly assigns women to practice yoga or another type of exercise, can determine the causal relationships. However, given the significant relationships between greater amounts of yoga practice and lower levels of self-objectification and greater body satisfaction found in Study 1, a longer or more intense yoga intervention with a longer follow-up period may be necessary to show significant improvement.
A second limitation of Study 1 concerns the nature of the sample. Over 90% of the yoga participants identified as European American. The small proportion of women of color could be due to the cost of classes (to the extent that ethnicity is correlated with income) or that fewer women of color are interested in yoga. The question remains as to whether these results generalize to non-White samples. As of now, there is no reason to think that developing body awareness and responsiveness would not equally benefit women of color. The sample in Study 2 was ethnically diverse, with over 50% of the sample identifying as Asian American. Given that greater body responsiveness was associated with less disordered eating attitudes in this sample, it is reasonable to suggest that the results of Study 1 would generalize to Asian Americans and other women of color. However, it is important to note that the average BMI of the women who participated in Study2 was lower than the mean of those in Study 1. It remains unclear whether the findings of Studies 1 and 2 apply to overweight or obese women (i.e., BMI > 25). Future research should examine the relationship of body responsiveness to self-objectification and disordered eating in women who have higher BMIs.
In conclusion, future research is needed to replicate the findings from both of the present studies. Given that this study is one of the first to examine yoga and promising findings were observed, further research on yoga is warranted. In general, more research that seeks to identify factors that protect against the internalization of self-objectification is needed to promote the psychological and physical well-being of young girls and women.