
Abstract
Prenatal depressive symptoms have been linked to negative outcomes for mothers and children. Using attachment theory as a framework, this study examined developmental differences in the interpersonal context of prenatal depressive symptoms among adolescents (age 14 to 19 years; n = 352) and young adults (age 20 to 24 years; n = 348). Participants included low-income, single, predominantly African American and Latina women. Moderating and mediating factors were found in the relation between caregiving history (perceived unavailability and inconsistency of maternal and paternal figures during childhood) and depressive symptoms. For pregnant adolescents, maternal unavailability predicted depressive symptoms whereas maternal inconsistency did not. In contrast, for pregnant young women, only maternal inconsistency predicted depressive symptoms; and this association was mediated by perceptions of prenatal support. For both groups, paternal caregiving history had a small yet independent association with depressive symptoms. Results highlight the need to consider developmental differences in the interpersonal context of prenatal depressive symptoms in delivering mental health interventions to young women of color.
In recent years, there has been increased awareness among perinatal mental health researchers of the need to study prenatal depression, in addition to the well-studied area of postpartum depression. Depressive symptoms during pregnancy have been linked to negative birth outcomes and poorer newborn health (Field et al., 2004; Hoffman & Hatch, 2000; Orr, James, & Prince, 2002). In addition, there is growing evidence that heightened negative affect during pregnancy may have adverse effects on later child development by altering fetal neurodevelopment (e.g., Huot, Brennan, Stow, Plotsky, & Walker, 2004). Finally, the presence of depressive symptoms during pregnancy is a robust predictor of postpartum depression, and the negative effects of postpartum depression on parenting and early mother–infant relationships are well established (for review, see Field, 2002).
Given these adverse outcomes, it is important to identify psychosocial characteristics that may increase the risk for prenatal depressive symptoms. There are at least two reasons why it is particularly important that research in this area include women of color. First, because women of color are disproportionately affected by poverty, they are at increased risk for experiencing stress and depression during pregnancy (Deal & Holt, 1998). Depressive symptoms may also have a stronger impact on birth outcomes among poor women (Hoffman & Hatch, 2000). Second, there are cultural differences in the meaning of pregnancy and motherhood that may influence women's emotional experiences during the perinatal period (Beck, 2006). Consequently, theoretical assumptions and intervention efforts based on research primarily with White women may not be fully applicable in women from other cultural backgrounds.
One characteristic that has consistently emerged as a risk factor for depression during the prenatal and postnatal period across diverse samples concerns a woman's history of relationships with her own caregivers. Specifically, women who recall harsh or negative early caregiving relationships report greater depression during pregnancy and show increases in depression from the prenatal to postpartum period (Matthey, Barnett, Ungerer, & Waters, 2000; McMahon, Barnett, Kowalenko, & Tennant, 2005; Milan et al., 2004). These findings can be understood within the framework of attachment theory. According to attachment theory, humans are born with an innate potential to form attachments with caretakers (Bowlby, 1988). Ideally, interactions with attachment figures provide a child with a sense of “felt security,” which can be viewed as a sense of personal safety and interpersonal closeness. In this context, children learn to use close relationships as a source of comfort during times of heightened emotional distress. In contrast, when a caretaker is harsh, unavailable, or inconsistent, children must learn strategies for dealing with negative emotions (Sroufe, Carlson, Levy, & Egeland, 1999). As a result, children who experience parental unavailability or inconsistency are particularly vulnerable to later depression (e.g., Dozier, Stovall, & Albus, 1999).
From an attachment theory perspective, relationships with attachment figures may be especially relevant for understanding mental health during the transition to motherhood. The prenatal and postnatal periods are stressful for most people (Cowan & Cowan, 2000), and stress is theorized to trigger the attachment system (Bowlby, 1988). In addition, becoming a parent involves normative changes in close relationships and increased focus on caregiving experiences (e.g., Feeney, Hohaus, Noller, & Alexander, 2001). As a result, the quality of current and past relationships may be particularly potent during this time. Empirical studies in this area are limited, yet they support the view that the nature and impact of relationships with attachment figures may change during the transition to motherhood. For example, in a study comparing pregnant and nonpregnant women, Feeney, Alexander, and Noller (2003) found that attachment insecurity was associated with increases in depression over time only among the pregnant women. Similarly, in a study comparing pregnant and nonpregnant adolescents from similar low-income communities over a 2-year period, Milan et al. (2004) found that adolescents' reports of negative caretaking experiences during childhood were associated with chronic and increasing emotional distress only among the pregnant adolescents.
These studies highlight how the quality of a woman's caregiving history may be an especially important factor in understanding depressive symptoms during pregnancy. Within this line of inquiry, however, several issues have not yet been fully addressed. First, most studies have focused on women's reports of maternal hostility or abuse. In contrast, attachment theory posits that different types of parental behaviors may have distinct effects on child development. Specifically, different outcomes are expected when attachment figures are experienced as rejecting or unavailable versus when they are experienced as inconsistent or erratic (Bowlby, 1988). In addition, the quality of maternal and paternal relationships may have a differential impact on an offspring's mental health (Connell & Goodman, 2002). To date, most studies focusing on prenatal depression have not empirically considered the potentially distinct influence of different caregivers (mothers versus fathers) or different types of negatively perceived caregiving behaviors (hostile and unavailable vs. inconsistent and erratic).
Second, the mechanisms by which caregiving history relate to prenatal depression remain largely unexamined. Plausibly, associations between caregiving history and prenatal depression may be mediated by differences in pragmatic and emotional support surrounding pregnancy. This may be particularly true among young, unmarried women, who may depend more on parental figures, and among young women of color, who may be more likely to raise children in three-generation households (Caputo, 1999). Although there is a large body of literature indicating that low levels of support during pregnancy increase the risk for depression, researchers generally have not examined whether perceptions of caregiving history relate to depressive symptoms through differences in pregnancy-related support. Understanding potential mechanisms of influence has implications for the type of interventions that may be useful during pregnancy, such as programs aimed at increasing pragmatic support versus interpersonal models of psychotherapy.
Finally, few studies have examined age differences in the association between caregiving history and prenatal depressive symptoms. The influence of caregiving history should depend in part on an individual's level of dependency on parental figures. Consequently, negative relationships with parents may be especially detrimental to the mental health of pregnant adolescents when compared to their older counterparts. More broadly, adolescence is a transitional period involving a number of biological, social, and contextual changes that alter the nature of attachment relationships with parents (Allen & Land, 1999); thus, the influence of parental relationships on mental health may also change at this time. Despite theoretical reasons to believe caregiving history may have a different meaning for adolescents relative to young women, few studies have examined the potential moderating effect of age on interpersonal risk factors for prenatal depression. Because adolescent parenthood often occurs in the context of other potential risk factors for depression (e.g., poverty, single parenthood), it is important that research in this area include adolescents and young adults with similar demographic and socioeconomic characteristics (Milan et al., 2004). To date, this line of study has not been adequately pursued.
In sum, the current study expands existing literature on the interpersonal nature of prenatal depression by clarifying the role of young women's caregiving history on prenatal depressive symptoms within a sample of unmarried, low-income, primarily minority adolescent and young adult women. More specifically, the goals of this study are to: (a) specify what aspects of caregiving history relate to prenatal depressive symptoms, (b) examine whether effects of care-giving history on prenatal depressive symptoms differ for adolescent versus young adult women, and (c) determine whether relations between caregiving history and prenatal depressive symptoms are mediated by prenatal support.
METHOD
Participants and Procedures
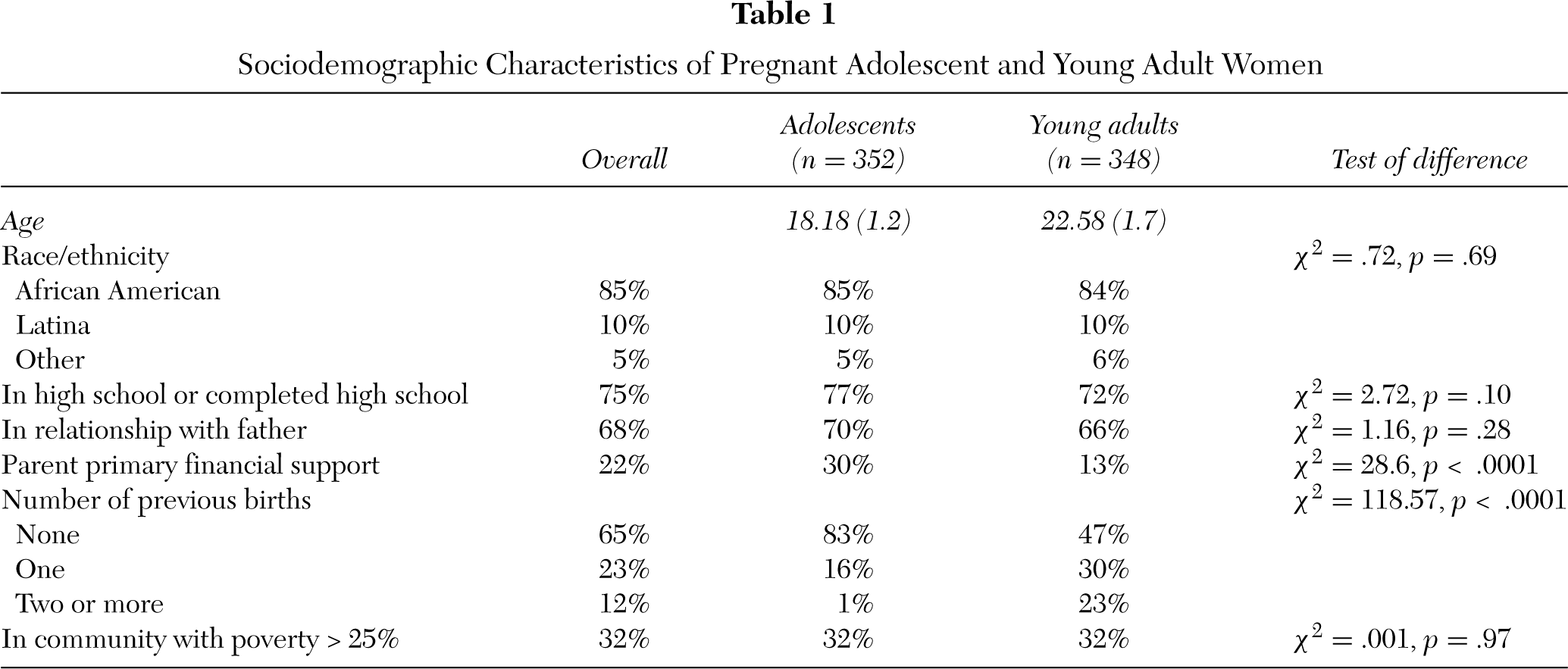
Data for this study are based on a subsample from a larger study of 1,047 young pregnant women (ages 14 to 25 years) enrolled in a randomized controlled trial (RCT) aimed at promoting improved general health and reproductive health behaviors through group prenatal care. This is a prospective study following participants from early pregnancy through 1-year postpartum. Participants were recruited from obstetrics and gynecology clinics in two large hospitals in New Haven, Connecticut and Atlanta, Georgia. Participants in the study were predominantly African American and Latina (mostly Puerto Rican), reflecting the population of prenatal patients using these clinics. The care-giving history measures of interest for the present purposes were added during the second year of the RCT; thus, the current sample includes all women enrolled in the study after this point (n = 748). In addition, because of the focus on young, unmarried women, 48 women who were married at study initiation were excluded, bringing the final sample to n = 700. There were no significant differences between the RCT participants included in this study and those not included on demographic characteristics or variables of interest. Descriptive data about the current sample is presented in Table 1.
Between September 2001 and December 2004, young women attending their first or second prenatal care visit were referred by a health care provider or approached directly by research staff. Inclusion criteria were: (a) pregnant at less than 24 weeks gestation, (b) age at last birthday less than or equal to 25, (c) no severe medical problem requiring individualized assessment and tracking as “a high-risk pregnancy,” (d) able to attend groups conducted in English or Spanish, and (e) willingness to be randomized to group versus individual prenatal care. Sixty-eight percent of women approached for potential participation were enrolled in the RCT. Those who agreed to participate were more likely to be African American, older, and at a later gestational age at initial screening than those who refused to participate (p < .01 for all).
Baseline interviews occurred in the second trimester at an average gestational age of 18 weeks (SD = 3.3). Baseline interviews involved structured interviews via audio computer-assisted self-interviewing (A-CASI). A-CASI allows respondents to listen over headphones to spoken questions that have been digitally recorded and stored on a computer, as well as displayed on the computer's screen. Numerical responses are given on the computer keyboard and automatically stored in an electronic database. All procedures were approved by the Yale University and Emory University Human Investigation Committees and by Institutional Review Boards at study centers. Participants were paid $25 for each interview.
Measures
Center for Epidemiological Studies-Depression (CES-D; Radloff, 1977). The CES-D was used to assess depressive symptoms. The CES-D is a widely used, 20-item scale designed to measure the major components of clinical depression. Respondents rated the frequency with which they had experienced various depression symptoms (e.g., sadness, crying, hopelessness) over the last 7 days on a 0 to 3 scale ranging from 0 (rarely or none of the time) to 3 (most or all of the time). Acceptable psychometric properties have been reported in a variety of samples; however, the CES-D can inflate estimates of depression in medical samples because several items reflect somatic complaints that occur with illness, medical conditions, or pregnancy (e.g., changes in sleep patterns or appetite). As recommended by others (e.g., Kalichman, Rompa, & Cage, 2000), we addressed this possible confound by using only the cognitive-affective subcomponent of the CES-D, in which the five somatic items were removed. Within this sample, alpha for the CES-D cognitive-affective subcomponent was .85.
Sociodemographic Characteristics of Pregnant Adolescent and Young Adult Women
Prenatal social support (adapted from O'Brien, Wortman, Kessler, & Joseph, 1993). This 4-item scale assessed perceived availability of support specific to prenatal care and pregnancy. An example item is: “Are there people to give you information about your prenatal care, someone to take you to your prenatal care visits?” Responses were rated on a 5-point scale ranging from 1 (definitely not) to 5 (definitely yes). Alpha for the measure was .71.
Descriptions of parental caregiving style (Hazan & Shaver, 1986). The Parental Caregiving Style measure was used to assess the perceived quality of caregiving during childhood from primary caretakers. This measure presented three descriptive paragraphs about different caretaker behaviors that theoretically influence quality of attachments to caretakers. One paragraph described parental behaviors associated with a secure attachment (e.g., “My mother was generally warm and there for me. She was good at knowing when to give me support and when to let me do things on my own …”). The other two paragraphs described caregiver behaviors associated with insecure attachments, particularly parental unavailability (e.g., “My mother was fairly cold and distant. Most of the time, she was not there for me …”) and parental inconsistency (e.g., “My mother was inconsistent in the way she reacted to me. Sometimes she was warm but other times she was not …”). Respondents rated how true each descriptive paragraph was for them using a 7-point scale ranging from 1 (not at all true) to 7 (completely true). Responses on this measure can be provided regardless of parent residential status, and participants were told to base their response on the relationship with their biological parent or the most applicable parental figure (e.g., stepfather). Participants responded separately for the relationship with their mother or mother figure and father or father figure. Items reflecting maternal unavailability, maternal inconsistency, paternal unavailability, and paternal inconsistency were included in this study.
Sociodemographic control variables. Participants provided information about demographic characteristics on a questionnaire designed for this study. These variables were: race (African American, Latina, White/other), education (high school degree/currently in school or high school dropout), employment (full/part-time employment or unemployed), parent as primary source of financial support (yes or no), number of previous births (0, 1, 2, or more), and relationship status with baby's father (currently in romantic relationship or not). In addition, level of community poverty was measured based on the percent of people below the poverty level within the participant's census tract, using 2000 census data. For the current purposes, participants under the age of 20 years were considered adolescents (n = 348), and participants age 20 and over were considered young adults (n = 352). The similar number of adolescent and young adult women included in this sample was not an explicit part of the study design but rather reflects the demographic composition of the targeted patient population.
Analytic Plan
Potential age group differences in the association between caregiving history and depressive symptoms were examined using nested model, multigroup comparisons in structural equation models (SEM; Byrne, 2001). In this approach, the same model (i.e., the four caregiving variables predicting depressive symptoms; see Figure 1) is simultaneously generated for different groups (i.e., adolescents vs. young adults). Group differences in specific parameter estimates can be examined as a z test in which the null hypothesis is equality across groups (e.g., regression weight of maternal unavailability on depression in adolescents equals regression weight of maternal unavailability on depression in young adults). Significant differences suggest that the parameter value is not the same for the two groups (i.e., a moderating effect of age on that parameter). After testing for group differences, the fit of a final SEM model was estimated. In the final model, correlations between the four caregiving variables were constrained to be equal across age groups, as were the paths from caregiving variables to depressive symptoms that were found to be similar across age groups in pairwise comparisons, as described above. Paths that differed significantly by age group were allowed to vary in the two age groups.
Next, a SEM approach to the Baron and Kenny (1986) framework for testing mediation was used to determine whether prenatal support mediated the relation between caregiving history and depression. In this approach, mediating effects are suggested if a significant direct path between caregiving history variables and depressive symptoms becomes nonsignificant or is significantly reduced when prenatal support (the mediating factor) is entered in the model. All models were tested using AMOS 5.0 and full-information maximum likelihood (FIML) approaches to estimation.
RESULTS
The average age in the adolescent group was 18.2 years (SD = 1.23, range = 14 to 19), and the average age in the young adult group was 22.6 years (SD = 1.71, range = 20 to 24). Demographic characteristics are presented in Table 1. Adolescents did not differ from young women in terms of race, education, employment, relationship status with the baby's father, or level of community poverty. Not surprisingly, adolescents were significantly more likely to receive primary financial support from a parent (29% versus 12%) and less likely to have other children at home (17% versus 54%). These two characteristics were not associated with depressive symptoms, and thus, they were not potential confounds for the relations under investigation. Nonetheless, analyses were run both with and without these variables in the model to be conservative. Results did not differ.
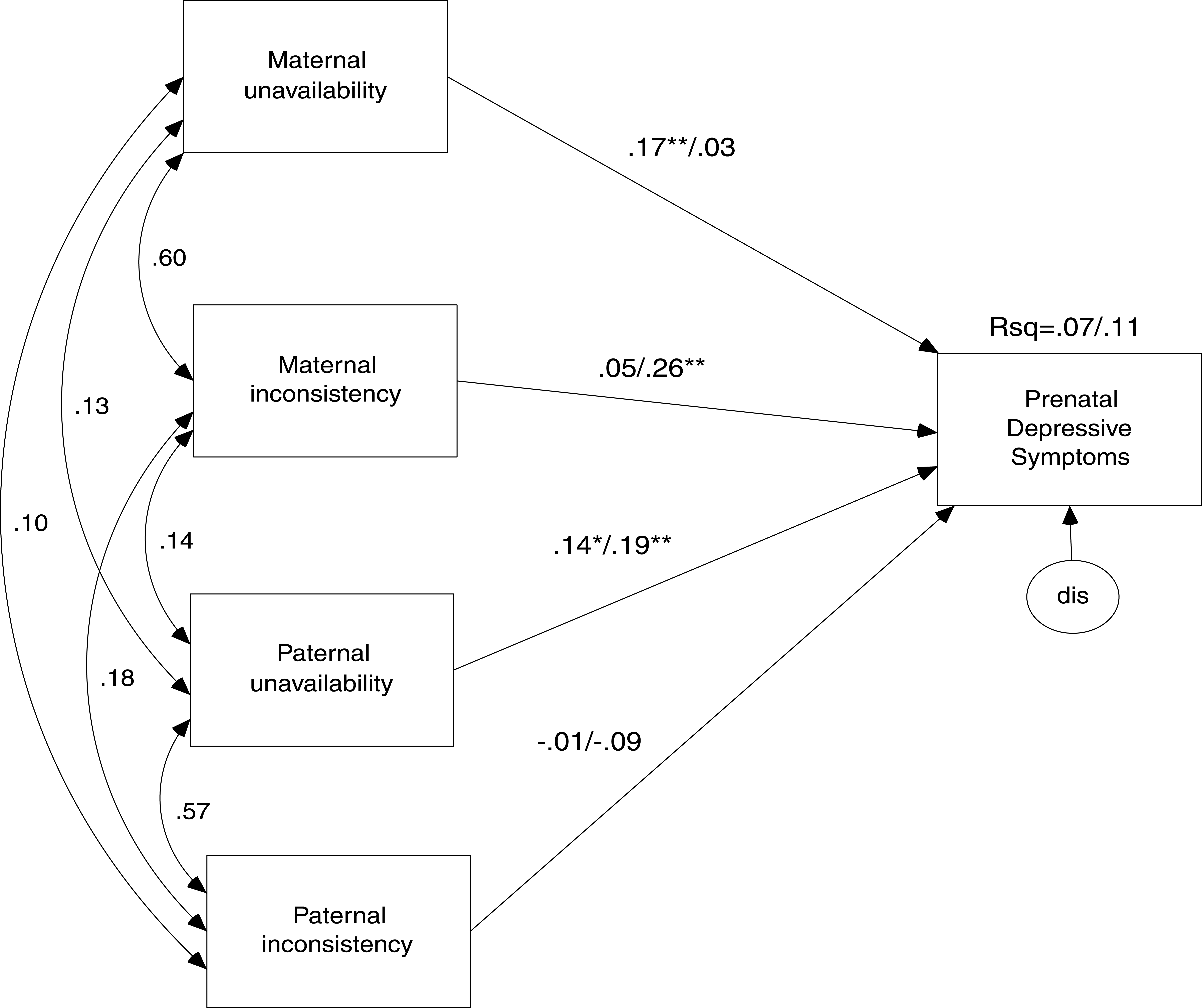
Parameter estimates from model predicting depressive symptoms from parental caregiving variables for pregnant adolescents (n = 352) and young adult women (n = 348). Parameter estimates before the slash represent values for pregnant adolescents; parameter estimates after the slash represent values for pregnant young adults. All correlations between caregiving variables were significant. Correlations between caregiving variables did not differ by group and were constrained to be equal across groups in the presented model. ∗ p < .05. ∗∗ p < .01. ∗∗∗ p < .001.
Table 2 presents descriptive information and age-group differences in the four caregiving variables (i.e., maternal unavailability, maternal inconsistency, paternal unavailability, paternal inconsistency), prenatal support, and depressive symptoms. Overall, participants reported more unavailability and inconsistency in relationships with fathers compared to mothers, t(687) = 9.48, p < .0001 for unavailability; t (686) = 3.23, p < .005 for inconsistency. Correlations between unavailability and inconsistency were high within the same relationship (r = .59, p < .0001 for mothers; r = .55, p < .0001 for fathers). Across relationship figures, correlations were statistically significant yet generally small (maternal and paternal unavailability, r = .13, p < .01; maternal and paternal inconsistency, r = .17, p < .001). In other words, participants held fairly distinct views of each parental figure. Correlations between caregiving variables did not differ significantly by age group.
Age Group Differences in Parental Caregiving History, Prenatal Support, and Depressive Symptoms
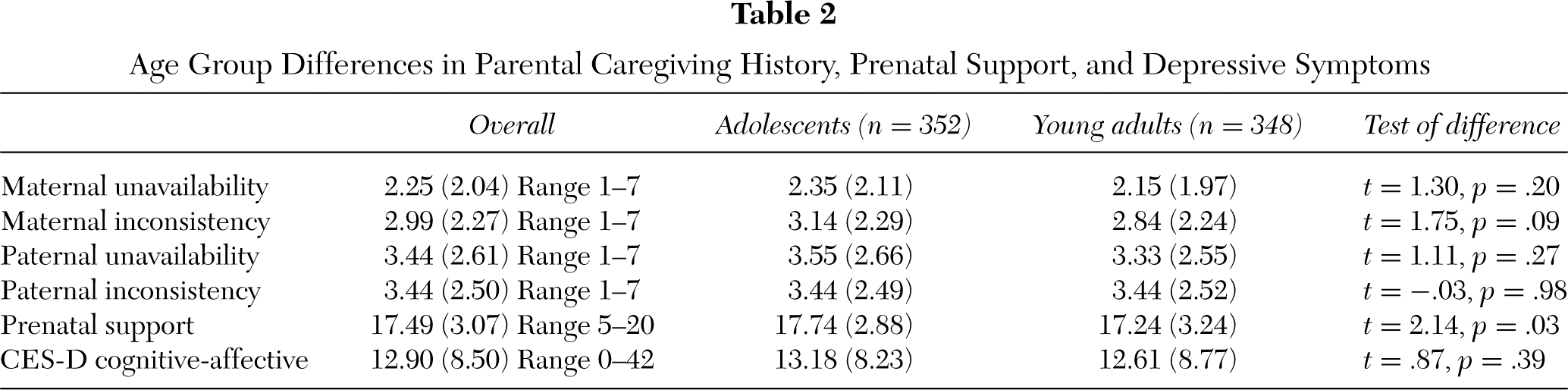
As shown in Table 2, mean differences on the four caregiving history items and depressive symptoms did not differ by age. In contrast, there was a small but significant group difference in prenatal support, with pregnant adolescents reporting more support than pregnant young women (Cohen's d = .19). In both groups, approximately one third of the sample reported levels of depression that would be above established cutoff scores on the CES-D that are used to denote “probable depression” in research on community samples (i.e., scores greater than 16; McDowell & Newell, 1996).
Caregiving History and Depression: Moderator Effects
Multivariate tests of normality in SEM were conducted prior to testing for moderation and mediation. Initial tests of multivariate normality indicated a critical ratio of z = 2.68, p < 05; however, log transformations of the caregiving variables resulted in acceptable indicators of multivariate normality (z = 1.41, p > .05). Log transformed variables were used in the presented models.
Next, a SEM multigroup comparison was used to examine group differences in the effects of caregiving history on depression, as described in the Method section. Parameter estimates showing caregiving history variables predicting depressive symptoms by age group are presented in Figure 1. Significant group differences were found for maternal unavailability (z = 1.96, p < .05) and maternal inconsistency (z = 2.66, p < .01). Maternal unavailability significantly predicted depressive symptoms among adolescents but not adults (β = .17, p < .01 for adolescents; β = .03, p = .64 for adults). In contrast, maternal inconsistency significantly predicted depressive symptoms among young adults but not adolescents (β = .26, p < .001 for young adults; β = .05, p = .42 for adolescents). No significant age-group differences were found for paternal caretaking variables. For both age groups, paternal unavailability predicted depressive symptoms although paternal inconsistency did not. The final model, in which maternal caretaking parameters were free to vary across age groups but paternal caretaking parameters were constrained to be equal, provided a good fit to the data (χ 2 = 6.87, df = 8, CFI = 1.00, RMSEA = .00).
Caregiving History: Mediating Effects
The next set of analyses tested whether the relation between caregiving history variables and prenatal depressive symptoms was mediated by prenatal support using SEM approaches to mediation, as described in the Method section. Paternal inconsistency was not related to depressive symptoms in either group in previous analyses, and thus, it was not included in tests of mediation. Paternal unavailability was related to depressive symptoms in both groups in previous analyses; however, it was not significantly correlated with prenatal support for either age group. Paternal unavailability was therefore included in the model as a predictor of depressive symptoms, yet mediation tests focused only on maternal caregiving variables.
Using nested model comparisons, two models (i.e., mediation in adolescents, mediation in young adults) were tested against a base model in which the correlations between caregiving variables and the path from paternal unavailability to depressive symptoms were constrained to be equal for adolescents and young adults, and all other paths were freely estimated. This base model provided a good fit to the data (χ 2 = 4.25, df = 8, CFI = 1.00, RMSEA = .00). As shown in Table 3, the model testing mediation in adolescents (i.e., a model in which direct effects of caregiving variables are constrained to 0 when prenatal social support is included in the model) resulted in a significantly worse fit to the data relative to the base model. In other words, for adolescents, the direct effect of maternal unavailability on depressive symptoms was not mediated by prenatal support. Instead, both maternal unavailability and prenatal support were independent, significant predictors of prenatal depressive symptoms.
In contrast, the mediation model did not provide a significantly worse fit to the data for young adult women, suggesting the association between maternal inconsistency and depressive symptoms is mediated by prenatal social support in this age group. That is, the significant direct path between maternal inconsistency and depressive symptoms became nonsignificant when prenatal support was included as a mediator (i.e., the path was reduced from β = .26, p < .001 to β = .10, p = .25), with prenatal support acting as a strong predictor of depressive symptoms (β = −.39, p < .001). In addition, the indirect effect of maternal inconsistency on depressive symptoms among young women was statistically significant in Sobel tests (indirect effect = .19, z = 5.16, p < .001). Pairwise comparisons also indicated that the path from maternal inconsistency to prenatal support was significantly larger in young women relative to adolescents (z = −3.33, p < .001). Parameter estimates for the mediation models for adolescents and young adults are presented in Figure 2.
Test of Mediating Effects of Prenatal Support on Relation Between Maternal Caregiving History and Depression in Adolescent and Young Adult Women
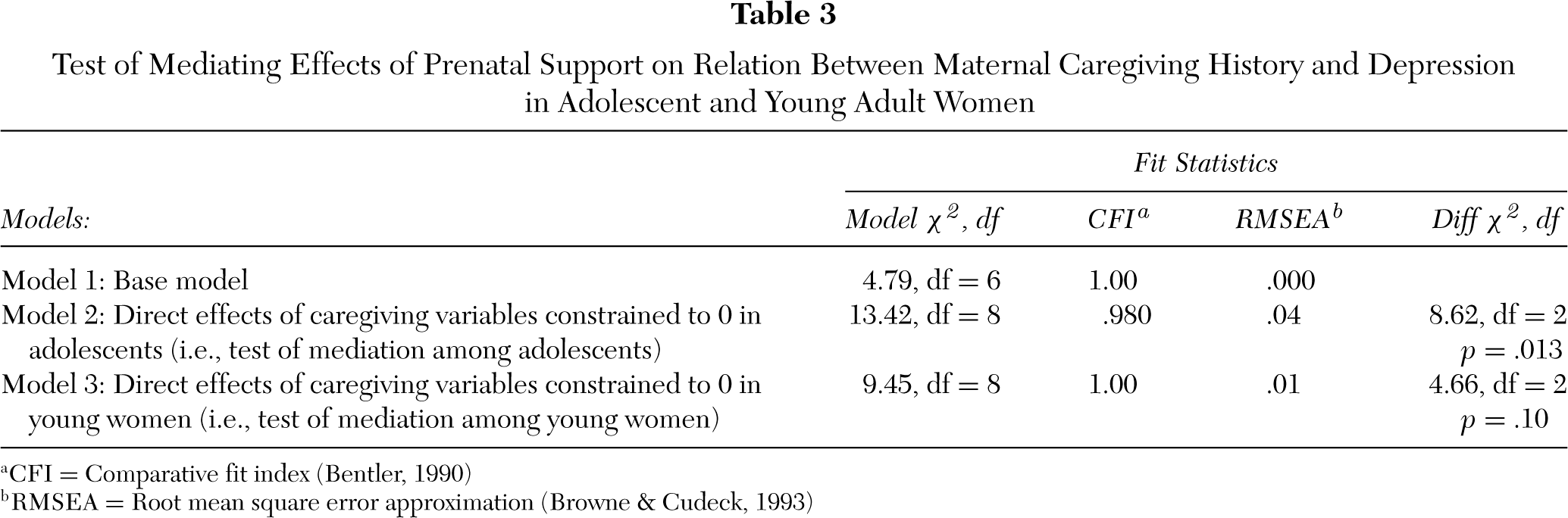
aCFI = Comparative fit index (Bentler, 1990)
bRMSEA = Root mean square error approximation (Browne & Cudeck, 1993)
In tests of mediation, alternative models are also often conceptually feasible, particularly when using cross-sectional data. Specifically, given reciprocal relations between depressive symptoms and social support (Joiner, 2002), it is possible that a negative caretaking history may lead to depressive symptoms, which in turn reduces perceptions of available or actual support from others. This alternative mediation model (i.e., depression mediating associations between caregiving history and prenatal support) was also tested; the model was a worse fit to the data based on multiple fit indices (χ 2/df =3.99, CFI = .94, RMSEA = .066). Because the present study was guided by attachment theory tenets, in which early childhood experiences influence later psychosocial functioning, we did not test models in which caretaking variables acted as endogenous variables.
DISCUSSION
Prenatal depressive symptoms are heightened among young, unmarried, low-income women. In the current study, approximately one third of participants reported symptom levels above the cutoffs generally used to denote probable depression in research settings. These estimates are consistent with other studies of low-income pregnant women (e.g., Deal & Holt, 1998) and suggest that the prevalence of elevated depressive symptoms in this population is high. Prevention and intervention efforts are therefore warranted. In light of this need, the current study aimed to better understand the interpersonal nature of prenatal depressive symptoms by elaborating on the role of caregiving history among young women of color.
Across the sample, correlations between reports of maternal and paternal unavailability and inconsistency were quite small. That is, participants tended to have distinct perceptions of the quality of caregiving received from their mother versus the quality of caregiving received from their father. Regardless of age, maternal and paternal caregiving variables independently predicted depressive symptoms. In particular, women who recollected their fathers as being unavailable or hostile during childhood reported higher levels of prenatal depression, independent of associations with maternal caregiving history. Although most research on caregiving history has focused on maternal relationships, our findings are consistent with studies that have included recollections of both parental figures (e.g., Matthey et al., 2000), which suggest paternal relationships may have independent effects on women's mental health during the transition to motherhood.
A primary goal of this article was to examine whether age differences existed in the associations between caregiving history and prenatal depressive symptoms. For both adolescents and young adult women, perceptions of maternal caregiving were related to depressive symptoms; however, the nature of these associations differed by age. For adolescents, perceptions of maternal unavailability significantly predicted prenatal depressive symptoms, and perceptions of maternal inconsistency did not. The opposite pattern emerged for young adults. That is, maternal inconsistency significantly predicted elevated depression, and maternal unavailability did not. It is important to note that participants' reports of maternal unavailability, inconsistency, and depressive symptoms did not differ by age; rather, it was the relation between these variables that differed by age.
Age differences also emerged in examining the potential mediating role of prenatal support in the relation between caregiving history and depression during pregnancy. For adolescents, the association between maternal caregiving history (i.e., maternal unavailability) and depressive symptoms was not mediated by prenatal support. Rather, both maternal unavailability and prenatal support independently predicted differences in depressive symptoms. In contrast, for young women, the association between maternal care-giving history (i.e., maternal inconsistency) and depressive symptoms was mediated by differences in prenatal support.
These findings, in conjunction with the generally higher levels of prenatal social support reported by adolescents, suggests that pregnant adolescents may receive pregnancy-related support from their mother, even if that relationship is perceived in a less than ideal way. By nature of their age, adolescents are likely to have considerable involvement from maternal figures in day-to-day life (e.g., through cohabitation, transportation needs). This involvement may result in additional pragmatic support from maternal figures, regardless of adolescents' perceptions of the emotional quality of the relationship. Further, mothers may feel a greater responsibility to provide support to pregnant adolescent daughters as opposed to older daughters. For adolescents then, negative perceptions of maternal care-giving may relate to feelings of depression only in more severe cases, in which a maternal figure is viewed as outright hostile and generally unavailable.
The relation between perceptions of maternal inconsistency and depressive symptoms found among young adult women in this sample is consistent with existing research. In studies of adults, anxiety about relationships with attachment figures, which putatively arises from experiences of parental inconsistency, has been found to be more predictive of increases in depression during the prenatal and post-partum period than attachment avoidance, which putatively arises from experiences of parental unavailability (Simpson, Rholes, Campbell, Tran, & Wilson, 2003). More generally, among young women, in secure attachments to parents characterized by anxiety pose a greater risk for depression than insecure attachments characterized by avoidance (Burge, Hammen, Davila, & Daley, 1997). Theoretically, in situations in which a parent is often inconsistent in how they treat their child, that child must deal with uncertainty about whether the parent will provide comfort during times of stress. Individuals who receive this form of parenting are believed to become more preoccupied and anxious about relationships, and they may develop a sense of self-worth that is contingent on the current standing of relationships. This contingent sense of self-worth in turn creates a vulnerability to subsequent depression (Crocker & Wolfe, 2001).
Parameter estimates from full mediation models for pregnant adolescents (n = 352; first model) and pregnant young adult women (n = 348; second model). Correlations between caregiving variables were included in the model and constrained to be equal across groups. These correlations are omitted in the figure for presentation. ∗ p < .05. ∗∗ p < .01. ∗∗∗ p < .001.
Although adolescents and young women reported similar levels of maternal inconsistency, the implications of maternal inconsistency differed. For young adults but not adolescents, higher maternal inconsistency was associated with perceptions of lower prenatal support, which in turn was predictive of heightened depressive symptoms. This same pattern was not evident in adolescents. There may be developmental reasons for this difference. Specifically, it may be normative for some adolescents to perceive their mothers as inconsistent or erratic, without these perceptions having the same negative implications for mental health. If such perceptions continue into adulthood, however, they may reflect a more stable or potentially negative view of childhood relationships. Thus, it may be only after the transition to adulthood that perceptions of maternal figures as inconsistent become a risk factor for depression. The nature of mother–daughter relationships changes from adolescence to early adulthood for pragmatic and developmental reasons; consequently, the meaning and importance of perceptions of these relationships may also change.
Our finding that prenatal support mediates the relation between maternal inconsistency and depressive symptoms provides preliminary insight into why maternal inconsistency may be a risk factor for young pregnant women. In general, mothers are a primary source of support for young, unmarried pregnant women. Although speculative, pregnant young women with a history of maternal inconsistency may continue to rely on their mother for emotional and pragmatic support during pregnancy, although their mothers may not provide consistent or adequate support. Such inconsistencies may in turn contribute to disappointment, awareness of unmet needs, or feelings of isolation, which in turn increase the likelihood for heightened depressive symptoms. In contrast, pregnant young women with a caregiving history characterized by maternal unavailability or rejection may have developed alternative sources of support (e.g., boyfriends, friends, siblings) in anticipation that their mother will not provide support or may have developed strategies for dealing with stressful life events in ways that minimize the need to rely on others (Mikulincer, Shaver, & Pereg, 2003).
Clinical Implication
Results from this study have three clinical implications. First, our findings on the distinct associations of maternal and paternal relationship history on prenatal depressive symptoms suggests that multiple relationships may influence mental health during the prenatal period. Thus, assessing women's caregiving history more broadly may facilitate better identification of young women most at risk for depression during pregnancy. Second, our results highlight the importance of considering developmental factors in designing programs to address prenatal depression. Within this sample, elevated depressive symptoms were found equally among adolescent and young adult women; however, the interpersonal context of symptoms differed by age. It is therefore important that services for pregnant adolescents consider these unique factors in identifying and treating those adolescents most likely to experience emotional difficulties during pregnancy.
Finally, our results suggest that young, unmarried women (i.e., age 20 to 24 years) may be underrecognized as a group in need of increased support and services during pregnancy. Relative to young adults, adolescents may receive more pragmatic and emotional support during pregnancy because of increased family involvement or targeted services (e.g., adolescent prenatal clinics, specialized high school programs). In contrast, young women, particularly those in the period of emerging adulthood with socioeconomic stressors, may have fewer available services and less family involvement. Developing programs that aim to increase emotional and pragmatic support in this age group may have beneficial effects on mental health. This might be accomplished through programs such as group prenatal care (Ickovics et al., 2003) or, for those young women most at risk, through more individualized programs targeting interpersonal risk factors (Spinelli & Endicott, 2003).
Limitations and Strengths
Results from this study must be interpreted in light of several limitations. First, this was a cross-sectional study involving retrospective reports about caregiving. Consequently, directionality of the relation between caregiving history, social support, and depression can only be hypothesized. In actuality, depressive symptoms and interpersonal difficulties likely have reciprocal effects (Joiner, 2002). Further, current depressive symptoms may lead individuals to report or recollect more negative past experiences. A second shortcoming of this study is the limited measurement of women's caregiving histories. The significant results suggest that this brief measure captures some aspect of individual differences in interpersonal risk factors; however, relationships with caregivers are complex and multidimensional, and the measure included in this study by no means captures this level of complexity. Although this type of abbreviated measure of perceptions of attachment relationships has clinical utility and documented validity (e.g., Holmes & Lyons-Ruth, 2006), a better understanding of the relation between caregiving history and prenatal depressive symptoms would be achieved with richer measures. Finally, the measure used to assess depressive symptoms in this study is a self-report, continuous scale, not a diagnostic tool. Because measurement and diagnosis of depression is particularly problematic in pregnancy, we chose to use a continuous scale in an effort to measure individual differences in depressive affect. However, the way in which depressive symptoms are measured and conceptualized (i.e., dimensional versus categorical) remains a heavily debated topic in clinical science research (e.g., Ruscio & Ruscio, 2000).
Despite these limitations, there are several strengths to this study. First, much of the research on the interpersonal context of depressive symptoms during pregnancy has not focused on women of color, despite the fact that cultural and economic factors influence the context of pregnancy and parenthood. Second, most studies on adolescent motherhood have not included comparison groups from similar socioeconomic backgrounds. As a result, our understanding of potential differences between pregnant adolescents and pregnant young women—independent of the socioeconomic factors that often co-occur with adolescent pregnancy—is limited. Results from this study and others (e.g., Deal & Holt, 1998; Milan et al., 2004) speak to the unique needs of both groups that must be considered in delivering developmentally and culturally relevant mental health interventions for pregnant women. Although our findings suggest interpersonal risk factors during pregnancy may differ depending on age, it is clear that heightened depressive symptoms are common among both adolescent and young adult pregnant women facing socioeconomic stressors. Consequently, efforts aimed at ameliorating the risk and consequences of prenatal depression in both groups are needed.