
Abstract
The purpose of this study was to test tenets of both minority stress and lesbian feminist/sexual identity development theories by examining the potential moderating and mediating roles of individual coping styles (i.e., problem-solving and avoidant coping) in the relationship between internalized heterosexism and lesbian and bisexual (sexual minority) women's psychological distress. Participants included 323 sexual minority women who completed an Internet survey. Results revealed that avoidant coping partially mediated the relationship between internalized heterosexism and psychological distress. No support was found for the mediating role of problem-solving coping or for the moderating roles of problem-solving and avoidant coping in the link between internalized heterosexism and psychological distress. Feminist strategies that may be useful for clinicians working with clients to reduce internalized heterosexism are provided.
Lesbian, gay, and bisexual (LGB) individuals can be targets of others’ discrimination as well as their own internalized prejudices. Heterosexism refers to the ideological system that serves to stigmatize and reject any nonheterosexual identity or way of being (Herek, 2004), and internalized heterosexism refers to the process of internalizing negative messages from experiences of heterosexism (Szymanski, 2006). These terms developed in response to concerns that prior terminology (e.g., homophobia, homonegativity, internalized homophobia, and internalized homonegativity) inadequately described the external and internalized oppression experienced by LGB persons and/or focused on individual attitudes that did not recognize the institutionalized and pervasive nature of such beliefs in current culture (Szymanski, Kashubeck-West, & Meyer, in press a). Minority stress (e.g., Meyer, 1995, 2003) and lesbian feminist/sexual identity development theorists (e.g., Brown, 1988, 1994; Cass, 1979; Sophie, 1987; Szymanski, 2005a, b) all assert that internalized heterosexism can create mental health problems for sexual minority women. In support of this assertion, most research has found positive relationships between lesbian and bisexual women's internalized heterosexism and psychological distress (cf., Frock, 1999; McGregor et al., 2001; Szymanski, 2005b; Szymanski & Kashubeck-West, in press).
Now that direct relations between internalized heterosexism and mental health have been demonstrated, it is important for research to move beyond the basic question of “Does internalized heterosexism predict psychological distress?” to an examination of theory-driven moderators and mediators of these relationships. Moderators address “for whom” or “when” a variable most strongly predicts an outcome variable, whereas mediators address the questions of “why” or “how” one variable predicts an outcome variable (Frazier, Tix, & Barron, 2004). Minority stress theorists and lesbian feminist/sexual identity development theorists diverge in their explanations concerning the relationship between internalized heterosexism and psychological distress, with minority stress theorists proposing moderating roles and lesbian feminist/sexual identity development theorists proposing mediating roles. Thus, the purpose of this study was to examine the potential moderating and mediating roles of coping styles in the link between internalized heterosexism and sexual minority women's mental health.
Specifically, two types of coping strategies were examined: problem-solving and avoidant coping. Problem-solving coping strategies are actions taken to change the source of stress, such as planning, taking direct action, and focusing on the current problem (Carver, Scheier, & Weintraub, 1989). Avoidant coping strategies include denial, giving up, and distraction or mental disengagement. Research with various populations has shown that individuals who use more problem-solving coping strategies have lower psychological distress and that individuals who use avoidant coping have higher levels of distress (e.g., Lefkowitz, 2003; Mytko et al., 1996; Nyamathi, Wayment, & Dunkel-Schetter, 1993; Penedo et al., 2003).
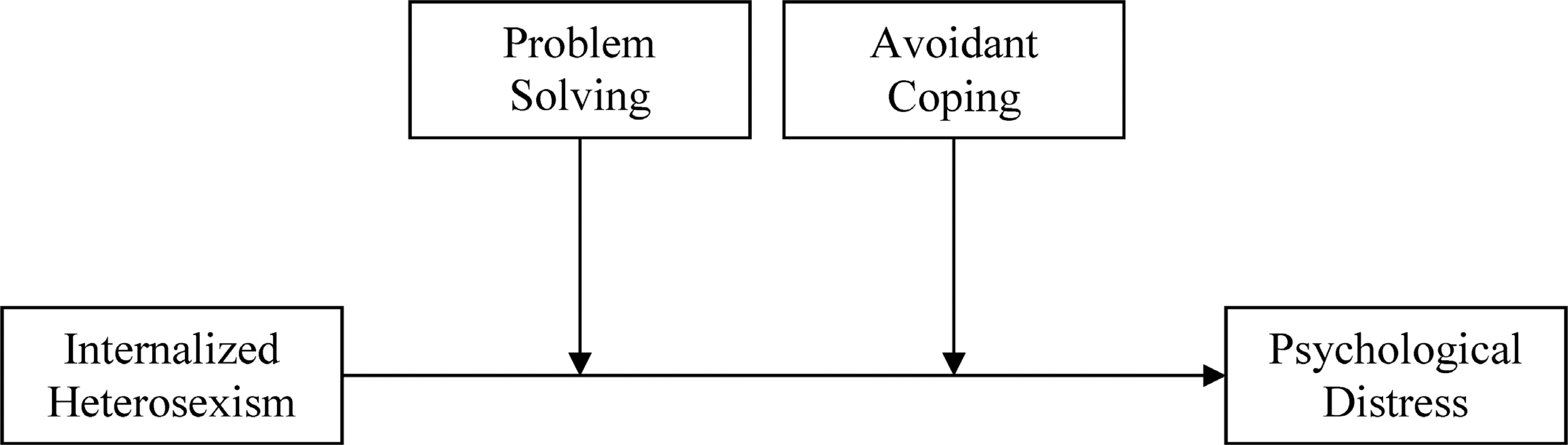
Hypothesized moderating roles of problem solving and avoidant coping in the link between internalized heterosexism and psychological distress.
Minority stress theory postulates that individuals from stigmatized social categories experience excess stress and negative life events because of their minority status (Brooks, 1981; Meyer, 1995, 2003). Internalized heterosexism is viewed as an internal or proximal stressor that can lead to negative mental health outcomes. From this perspective, coping is seen as a variable that can alter the strength of the association between stress and distress. Minority stress theory posits that individual coping and social support (e.g., resilience, hardiness, coping styles and strategies, social support systems) and LGB community coping and support (e.g., LGB social groups, services of an LGB affirmative church, LGB social activism activities) can help ameliorate the negative effects of minority stress (Meyer, 2003). Thus, minority stress theory suggests a moderator or interaction effect where the level of psychological distress depends on the interaction between internalized heterosexism and problem-solving and/or avoidant coping strategies (see Figure 1). In a moderated model, individuals’ coping strategies exist independently from the experience of a stressor (i.e., internalized heterosexism) to influence the relationship between a stressful event and an outcome (i.e., psychological distress). This moderated model implies that practitioners working with clients with high degrees of internalized heterosexism should help them to develop better coping strategies and social supports as a way to mute the unfavorable impact of their internalized heterosexism on their psychological well-being. Given the popularity of minority stress theory in LGB psychology (e.g., Bos, van Balen, van den Boom, & Sandfort, 2004; Diplacido, 1998; Kimmel & Mahalik, 2005; Waldo, 1999; Williamson, 2000), it is surprising that no studies have examined the moderating roles suggested by this theory.
In contrast to minority stress theory, lesbian feminist/sexual identity theorists (Cass, 1979; Sophie, 1987; Szymanski et al., in press a) posit that these same individual and community social supports and coping strategies are likely to mediate, rather than moderate, the relationship between internalized heterosexism and sexual minority women's psychological distress. In a mediated model, coping strategies are understood to be accessed and used as a function of the stressor (internalized heterosexism) and, in turn, to influence the outcome (i.e., psychological distress). Lesbian feminist/sexual identity theorists postulate that individuals with high internalized heterosexism may be more likely to engage in avoidant coping strategies, such as inhibiting same-sex behavior, denying personal relevance of information regarding LGB persons, restricting awareness of or exposure to information regarding LGB persons and culture, passing or pretending heterosexuality, and living a double life with a secret sexual minority self (Cass, 1979; Sophie, 1987; Szymanski et al., in press a). In addition, they posit that reducing internalized heterosexism is an important precursor to developing proactive and problem-solving coping strategies, coming out to others, and increasing one's social support network. It seems likely that individuals with low levels of internalized heterosexism may be more likely to engage in problem-solving coping strategies to eliminate the source of stress and actively confront heterosexism through a variety of means (e.g., confronting heterosexist behaviors of others; heightening awareness of heterosexism among family, peers, and communities; challenging biased policies of businesses and organizations; supporting LGB-friendly businesses and organizations; and fighting to change laws and institutions that discriminate against LGB individuals; Kashubeck-West, Szymanski, & Meyer, in press).
Szymanski et al. (in press a) asserted that internalized heterosexism is likely to limit an LGB person's access to individual and community social support systems, negatively impact one's personal coping resources, and lead to the use of fewer problem-solving and more avoidant coping styles, which, in turn, will lead to greater psychological distress. Coping strategies would therefore play a mediating role if internalized heterosexism leads to the use of less problem-solving coping strategies and/or more avoidant coping strategies, which create greater levels of psychological distress (see Figure 2). In contrast to minority stress theory, the mediated model suggested by Szymanski et al. (in press a) directs practitioners’ efforts toward reducing clients’ internalization of heterosexism as the root cause of both distress and dysfunctional coping.
Consistent with lesbian feminist/sexual identity development theorists’ assertions, researchers have found that greater internalized heterosexism is related to more conflict concerning sexual orientation, greater frequency of passing as a heterosexual, lower overall social support, less satisfaction with social support, lower utilization of problem-solving coping, and higher use of avoidant coping among lesbian and bisexual women (see Szymanski, Kashubeck-West, & Meyer, in press b, for a review). In addition, findings from two research studies (McGregor et al., 2001; Szymanski & Kashubeck-West, in press) were consistent with the notion that internalized heterosexism among sexual minority women leads to psychological distress through less social support. However, no studies have examined the potential mediating role of individual coping styles in the link between internalized heterosexism and sexual minority women's psychological distress.
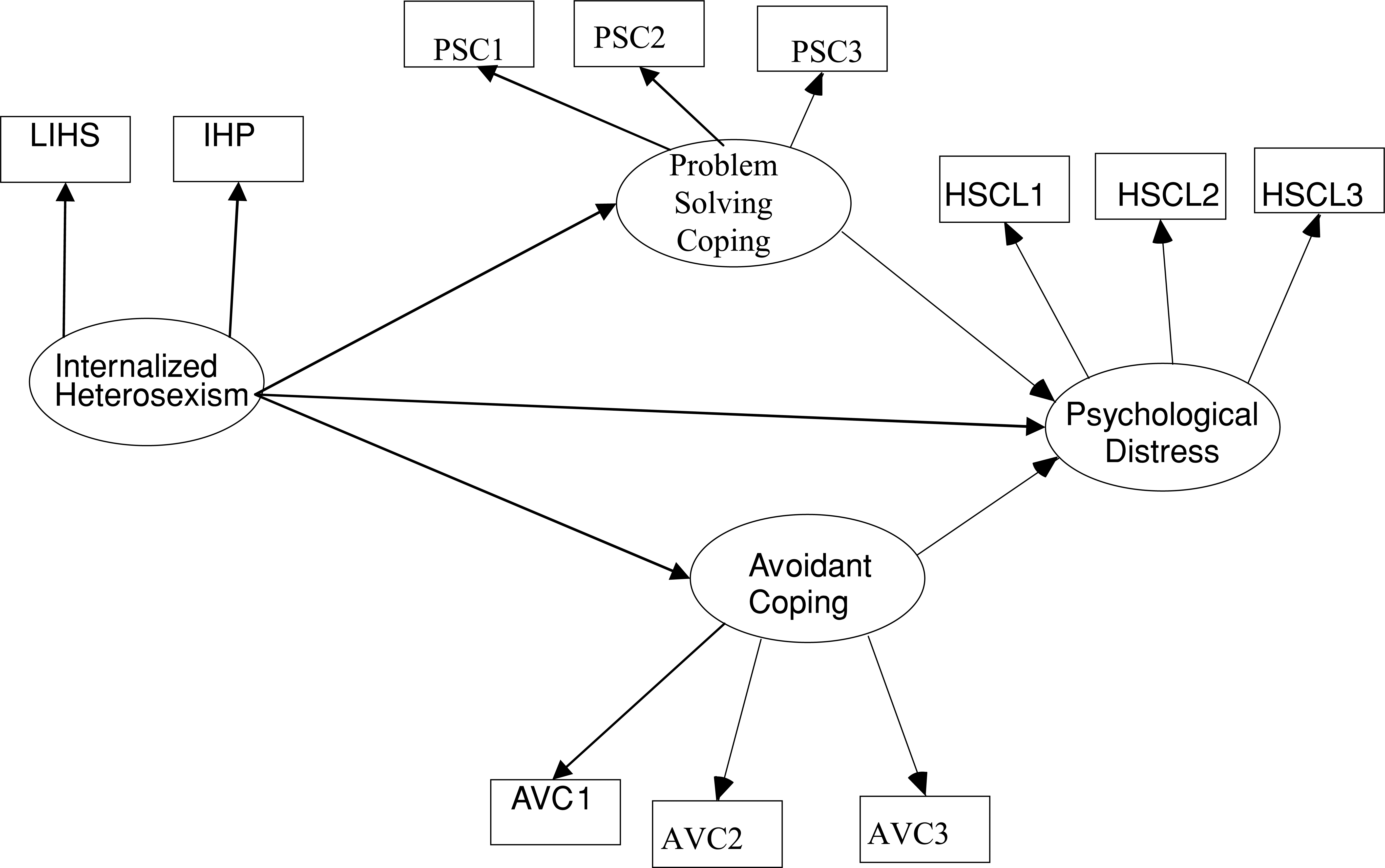
Hypothesized partially mediated model (all lines) and fully mediated model (all lines except for the direct path between internalized heterosexism and psychological distress). Note: Rectangles indicate measured variables, and ovals indicate latent constructs. LIHS = Lesbian Internalized Homophobia Scale; IHP = Internalized Homophobia Scale; PSC1, PSC2, and PSC3 = COPE Inventory problem solving subscales (i.e., Active Coping, Planning, and Suppression of Competing Activities); AVC1, AVC2, AVC3 = COPE Inventory Avoidant coping subscales (Denial, Behavioral Disengagement, and Mental Disengagement). HSCL1, HSCL2, and HSCL3 = parcels of test items assessing psychological distress.
In sum, the purpose of our study was to test competing hypotheses from minority stress and lesbian feminist/sexual identity development theories by examining the potential moderating and mediating roles of individual coping styles (i.e., problem-solving and avoidant coping) in the relationship between internalized heterosexism and lesbian and bisexual women's psychological distress. Based on minority stress theory, we examined whether the interactions of internalized heterosexism and problem-solving and avoidant coping styles accounted for significant variance beyond their individual links in psychological distress (see Figure 1). Based on lesbian feminist/sexual identity development models, we also examined whether problem-solving and avoidant coping styles mediate (either partially or fully) the relationship between internalized heterosexism and psychological distress (see Figure 2).
METHOD
Participants
The initial sample comprised 334 women who completed an online survey. Eleven participants with substantial missing data (more than 10% of one measure) were eliminated from the data set, resulting in a final sample of 323 participants. Of the participants in the final sample, 61% identified themselves as lesbian, 32% as bisexual, and 7% as not sure. Consistent with their self-identification, participants’ descriptions of their current feelings of romantic/sexual attraction on a 7-point Likert scale ranging from 0 to 6 were: 28% attracted only to women (0), 50% attracted more to women than men (1 and 2), 10% attracted equally to both sexes (3), 12% attracted more to men than women (4 and 5), and 0% attracted only to men (6). Participants ranged in age from 18 to 69 years, with a median age of 29 years (SD = 11.15). The sample was 81% White, 8% Asian American/Pacific Islander, 2% African American/Black, 3% Hispanic/Latina, 1% Native American, and 5% Multiracial. Participants resided in the Midwest (35%), Northeast (23%), West (23%), South (15%), and outside the United States (4%). Twenty percent of the participants had earned a high school diploma, 10% had attended a 2-year college, 30% attended a 4-year college, and 40% attended graduate/professional school. Participants’ total household income included 39% under $29,999, 26% between $30,000 and $59,999, 17% between $60,000 and $89,999, and 18% earning $90,000 or more.
Measures
Internalized heterosexism. Internalized heterosexism was assessed using Piggot's (2004) short form of the Lesbian Internalized Homophobia Scale (LIHS; Szymanski & Chung, 2001) and the short form of the Internalized Homophobia scale (IHP; Herek, Cogan, & Gillis, 2000; Martin & Dean, 1987). The LIHS short form consists of 39 theoretically and factorially derived items reflecting internalized negative attitudes concerning lesbianism across five dimensions: personal feelings about being a lesbian, public identification as a lesbian, attitudes toward other lesbians, connection with the lesbian community–interaction, and connection with the lesbian community–knowledge of resources. We modified several of the LIHS items to be bisexual inclusive. Examples of items (with modifications in italics) include, “If I could change my sexual orientation and become heterosexual, I would” and “Being a lesbian/bisexual woman makes my future look bleak and hopeless.” Each item is rated on a 7-point Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree). Higher mean scores indicate greater internalized heterosexism. Piggot reported Cronbach's α for scores on the LIHS-Short full scale of .93. Validity was supported by exploratory factor analysis and correlating the LIHS with measures of self-esteem, depression, and psychosexual adjustment (Piggot, 2004). Cronbach's α for the current sample was .94.
The second measure of internalized heterosexism, the IHP short form, consists of five items that were originally derived from the diagnostic criteria for ego-dystonic homosexuality contained in the third edition of the Diagnostic and Statistical Manual for Mental Disorders (American Psychiatric Association, 1980). Example items include “I feel that being lesbian/bisexual is a personal shortcoming for me” and “I would like to get professional help in order to change my sexual orientation from lesbian/bisexual to straight.” Each item is rated on a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Higher mean scores indicate greater internalized heterosexism. The reported α for scores on the 9-item IHP with a lesbian/bisexual female sample was .71 (Herek, Cogan, Gillis, & Glunt, 1998). Validity was supported by correlating the IHP short form with the 9-item long form and with measures assessing connection with and feelings toward the LGB community, perceived stigma related to being LGB, degree of outness, self-esteem, and depression (Herek et al., 1998, 2000). Cronbach's α for the current sample using the five-item measure was .82.
Coping styles. Individual coping styles were assessed using the problem-solving and avoidant coping factors of the COPE Inventory–dispositional form (Carver et al., 1989), which consists of 12 items representing the three subscales (i.e., Active Coping, Planning, and Suppression of Competing Activities) of the problem-solving coping factor and 12 items representing the three subscales (i.e., Denial, Behavioral Disengagement, and Mental Disengagement) of the avoidant coping factor. Example items of problem-solving coping include “I try to come up with a strategy about what to do” and “I do what has to be done, one step at a time.” Example items of avoidant coping include “I say to myself this isn't real” and “I sleep more than usual.” Participants indicated what they generally do and feel when they experience stressful events using a 4-point Likert scale ranging from 1 (I usually don't do this at all) to 4 (I usually do this a lot). Higher mean scores indicate greater problem-solving coping and less avoidant coping. Reported α's for scores on the Active Coping, Planning, Suppression of Competing Activities, Denial, Behavioral Disengagement, and Mental Disengagement subscales were .62, .80, .68, .71, .63, and .45, respectively. Validity was supported by correlating the COPE subscale scores with measures of hardiness, optimism, anxiety, self-esteem, and Type A personality (Carver et al., 1989). For the current sample α were .89 (Problem Solving factor), .81 (Active Coping subscale), .85 (Planning subscale), .67 (Suppression of Competing Activities subscale), .82 (Avoidant Coping factor), .85 (Denial subscale), .74 (Behavioral Disengagement subscale), and .59 (Mental Disengagement subscale).
Psychological distress. Psychological distress was assessed using the Hopkins Symptom Checklist (HSCL; Derogatis, Lipman, Rickets, Uhlenhuth, & Covi, 1974), which consists of 58 items reflecting psychological distress across five symptom dimensions: depression, anxiety, interpersonal sensitivity, obsessive compulsive symptoms, and somatization. Examples of items include “Crying easily” and “Worrying or stewing about things.” Participants indicated how often they had felt each symptom during the past several days using a 4-point Likert scale ranging from 1 (not at all) to 4 (extremely). Higher mean scores indicate greater psychological distress. Reported α's for total scores on the HSCL ranged from .84 to .87. Test-retest reliability ranged from .75 to .84. Validity of the HSCL was supported by studies reflecting the factorial invariance of HSCL symptom dimensions, between group differences, and the HSCL's sensitivity to the use of psychotherapeutic drugs (Derogatis et al., 1974). For HSCL full-scale scores for the current sample, α was .96. For scores on the three HSCL item parcels used in the structural equation modeling (SEM) analyses, α's were .88 (HSCL1), .90 (HSCL2), and .90 (HSCL3).
Procedure
An Internet survey was used to collect the data. As an incentive to participate, all participants were given the chance to enter a raffle awarding $100 each to three randomly selected participants. Procedures for this Web site survey were based on published suggestions (Buchanan & Smith, 1999; Michalak & Szabo, 1998; Schmidt, 1997). Methods for protecting confidentiality included having participants access the research survey via a hypertext link rather than e-mail to ensure participant anonymity and the use of a separate raffle database so there was no way to connect a person's online raffle submission with her submitted survey. Methods used for ensuring data integrity included the use of a secure server protected with a firewall to prevent tampering with data and programs and inadvertent access to confidential information by research participants. Cookies were used to identify problems associated with multiple submissions of data from the same computer. Research has shown that results from Internet studies are consistent with findings obtained from traditional pencil-and-paper methods; Internet samples of LGB persons compare well with data from national LGB samples; Internet studies are not adversely affected by nonserious or repeat responders; and demographic characteristics of respondents to Internet surveys are virtually indistinguishable from nonresponders (Gosling, Vazire, Srivastava, & John, 2004; Koch & Emrey, 2001).
An e-mail announcement of the study was sent to a variety of general lesbian and/or bisexual related listserves, groups, and organizations primarily found through Internet searches of Yahoo Groups, Gayyellowpages.com, and university and community LGBT centers. The e-mail announcement stated that the researchers were conducting an empirical study examining attitudes, feelings, and experiences associated with being a lesbian, bisexual, or questioning (unsure of sexual identity) woman. Potential participants used a hypertext link to access the survey Web site. After reading an informed consent, participants were instructed to complete the online survey, which included the aforementioned measures. We were able to determine that 580 potential participants visited the Web site cover page, 476 advanced to the survey page, and 334 completed the survey. Thus, 58% of participants who visited the Web site cover page completed the survey.
RESULTS
Means, standard deviations, and intercorrelations among all continuous variables assessed in this study are shown in Table 1.
Moderator Analyses
To test the moderator hypothesis suggested by minority stress theory, we conducted two multiple regression analyses. For both regressions, main effects were entered at Step 1 and interaction effects at Step 2. Aiken and West (1991) reported sample power analyses suggesting that when (a) the moderator and independent variables are correlated with each other at r = .50, (b) the block of variables entered prior to the interaction variable accounts for 20% of the variance, and (c) moderator and predictor variables are measured with perfect reliability, sample sizes of 55 and 392 are needed to achieve statistical power of .80 in detecting an interaction for moderate and small effect sizes, respectively. Thus, our sample size of 323 was large enough to detect an interaction of moderate effect size and just under what is needed to detect a small effect size. Prior to the analyses, scores for both measures of internalized heterosexism (i.e., LIHS and IHP) and coping styles (i.e., problem solving and avoidant) were centered to reduce potential multicollinearity problems.
Means, Standard Deviations, and Correlations for All Study Variables
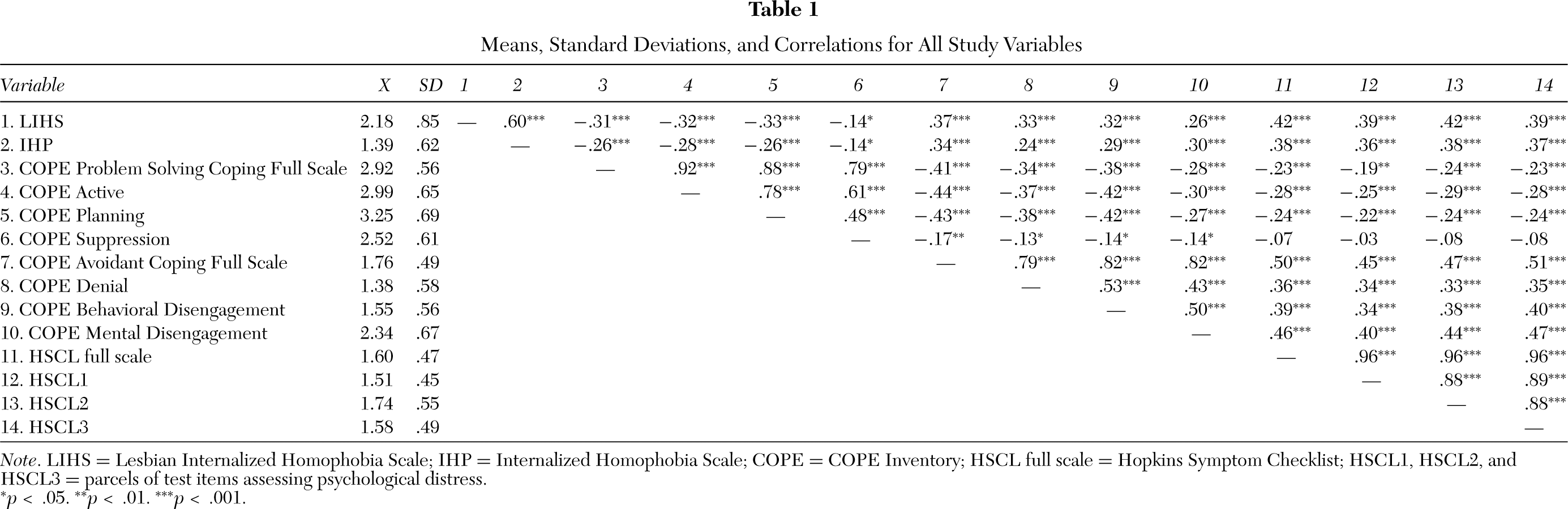
Note. LIHS = Lesbian Internalized Homophobia Scale; IHP = Internalized Homophobia Scale; COPE = COPE Inventory; HSCL full scale = Hopkins Symptom Checklist; HSCL1, HSCL2, and HSCL3 = parcels of test items assessing psychological distress.
∗p < .05. ∗∗p < .01. ∗∗∗p < .001.
The First regression used the LIHS, along with problem-solving and avoidant coping, to predict psychological distress. Absolute values of correlations between predictor variables (range = .22 to .67), variance inflation factors (range = 1.17 to 1.21), and condition index values (range = 1.00 to 2.87) were examined, and multicollinearity was deemed not problematic (Myers, 1990; Tabachnick & Fidell, 2001). The results of this analysis were significant, R2 = .32, F(5, 317) = 29.47, p < .001. Internalized heterosexism, as assessed by the LIHS, and avoidant coping were the only significant predictors of sexual minority women's psychological distress (see Table 2). Problem-solving coping and the interactions between the LIHS and both problem-solving and avoidant coping were not significant predictors of psychological distress, indicating that there were no moderating effects of internalized heterosexism, as assessed by the LIHS, and coping styles in predicting psychological distress.
The second regression used the IHP, along with problem-solving and avoidant coping, to predict psychological distress. Absolute values of correlations between predictor variables (range = .20 to .70), variance inflation factors (range = 1.26 to 1.42), and condition index values (range = 1.00 to 3.05) were examined, and multicollinearity was deemed not problematic (Myers, 1990; Tabachnick & Fidell, 2001). The results of this analysis were significant, R2 = .30, F(5, 317) = 27.72, p < .001. Internalized heterosexism, as assessed by the IHP, and avoidant coping were the only significant predictors of sexual minority women's psychological distress (see Table 2). Problem-solving coping and the interactions between the IHP and both problem-solving and avoidant coping were not significant predictors of psychological distress, again indicating that there were no moderating effects of internalized heterosexism and coping styles in predicting psychological distress.
Mediated Analyses
SEM was used to test the mediator hypothesis suggested by lesbian feminist/sexual identity development theorists. Following Tabachnick and Fidell's (2001) recommendation for a two-step approach to analysis, we used the Amos 5.0.1 program to estimate parameters for the measurement model via confirmatory factor analysis and for the later simultaneous estimation of the measurement and SEM. Our sample size of 323 was in the recommended range of 10–20 observations per estimated parameter (Weston & Gore, 2006). To check for univariate non-normality, we evaluated skewness and kurtosis for each measure/subscale/parcel used in the SEM analyses based on West, Finch, and Curran's (1995) criteria. No variable was skewed greater than 2 and no variable had a kurtosis greater than 7; thus, we determined that no substantial violations existed and no measures required transformation. To check for multivariate non-normality, we evaluated Mardia's coefficient of multivariate kurtosis. Although Mardia's coefficient of multivariate kurtosis indicated some degree of non-normality (obtained value = 43.73; critical ratio = 23.24), Lei and Lomax (2005) have found that parameter estimates and most model fit indices are robust to non-normality given maximum-likelihood estimation and a sample size of 100 or more participants. Thus, we proceeded with our analyses using maximum-likelihood estimation.
Because the χ2 statistic and goodness of fit indexes such as the goodness of fit index and normed fit index are easily distorted by factors extrinsic to actual model misspecification (e.g., number of indicators per factor, sample size), the adequacy of the measurement and structural model fit was based on the following goodness-of-fit indexes that minimize the effect of extrinsic factors: comparative fit index (CFI), Tucker–Lewis index (TLI), incremental fit index (IFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR) (Martens, 2005). Models with CFI, TLI, and IFI goodness of fit indexes greater than .95 and RMSEA values below .06 indicate a good-fitting model (Hu & Bentler, 1999).
In the confirmatory model, the two internalized heterosexism scales (LIHS and IHP) were constrained to load onto the Internalized Heterosexism factor, the three subscales of problem-solving coping (i.e., Active Coping [PSC1], Planning [PSC2], and Suppression of Competing Activities [PSC3]) were constrained to load on the Problem Solving factor, and the three subscales of avoidant coping, Denial (AVC1), Behavioral Disengagement (AVC2), and Mental Disengagement (AVC3), were constrained to load on the Avoidant Coping factor. The items from the psychological distress measure were randomly distributed into three item parcels (HSCL1, HSCL2, and HSCL3) and were constrained to load on the Psychological Distress factor. The four factors were permitted to correlate with one another. Fit statistics for the measurement model indicated an excellent fit of the data: CFI = .99, TLI = .98, IFI = .99, RMSEA = .05, and SRMR = .02. In addition, each measure significantly loaded on its intended latent factor (absolute factor loadings ranged from .62 to .97). Therefore, we moved to the next stage of the analysis: examination of the structural model and its fit to the data.
To establish mediation, Holmbeck (1997) asserted that one must first show that there is a relationship between the variables for which a mediator is predicted. Internalized heterosexism (β = .53) was a significant predictor at the p < .05 level in a SEM model predicting psychological distress. Next, two SEM analyses were conducted for partial and fully mediated models predicting psychological distress (see Figure 2). The first model was a partially mediated model that included an estimate of the direct effect between internalized heterosexism and psychological distress, as well as the mediated paths from internalized heterosexism to psychological distress via problem-solving and avoidant coping. Next, the fully mediated model was tested with the direct path between internalized heterosexism and psychological distress constrained to zero. The two nested models were then compared to see if including the direct paths from internalized heterosexism to psychological distress improved the fit of the model to the data (Holmbeck, 1997).
Summary of Hierarchical Regressions Predicting Psychological Distress
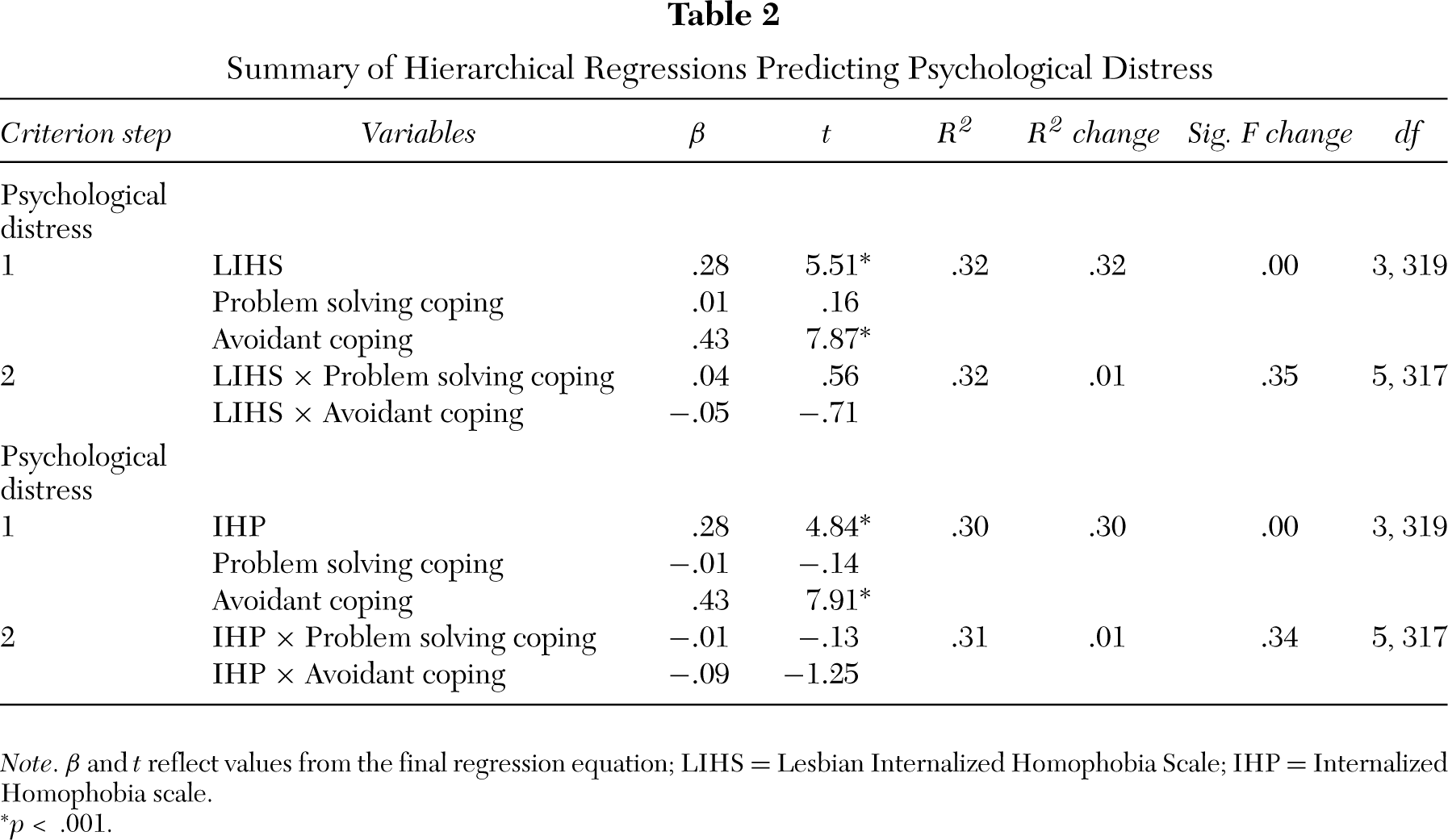
Note. β and t reflect values from the final regression equation; LIHS = Lesbian Internalized Homophobia Scale; IHP = Internalized Homophobia scale.
∗p < .001.
Fit statistics for the partially mediated SEM model indicated a good fit of the data: CFI = .97, TLI = .96, IFI = .97, RMSEA = .07, and SRMR = .03. All paths were significant except for the path from problem-solving coping to psychological distress. Fit statistics for the fully mediated SEM model also indicated a good fit of the data: CFI = .96, TLI = .95, IFI = .96, RMSEA = .08, and SRMR = .03. All paths were significant except for the path from problem-solving coping to psychological distress. Nested model comparison of the partially mediated model to the fully mediated model indicated that they were significantly different (difference χ2 = 14.895, df = 1, p < .05). Thus, the partially mediated model was retained as a better fit to the data.
Partial mediation indicated that internalized heterosexism was both directly and indirectly (through avoidant coping) related to psychological distress. To test whether this indirect effect was significant we used a bootstrap analysis to create 10,000 bootstrap samples from our data set as recommended by Mallincrodt, Abraham, Wei, and Russell (2006). Results of our analysis using a bias corrected 95% confidence interval for indirect relations indicated that the indirect link was statistically significant at p < .05. The mean indirect (unstandardized) effect was .14; the standard error of the mean indirect effect was .09; and the 95% confidence interval for the mean indirect effect was .05 (lower limit) and .24 (upper limit). The standardized indirect effect of internalized heterosexism on psychological distress via avoidant coping was β = .24 (i.e., .61 x .39). The squared multiple correlation for psychological distress was .40, which indicated that the variables in the model accounted for more than one-third of the variance in psychological distress. The relationship among latent variables for the final model is shown in Figure 3.
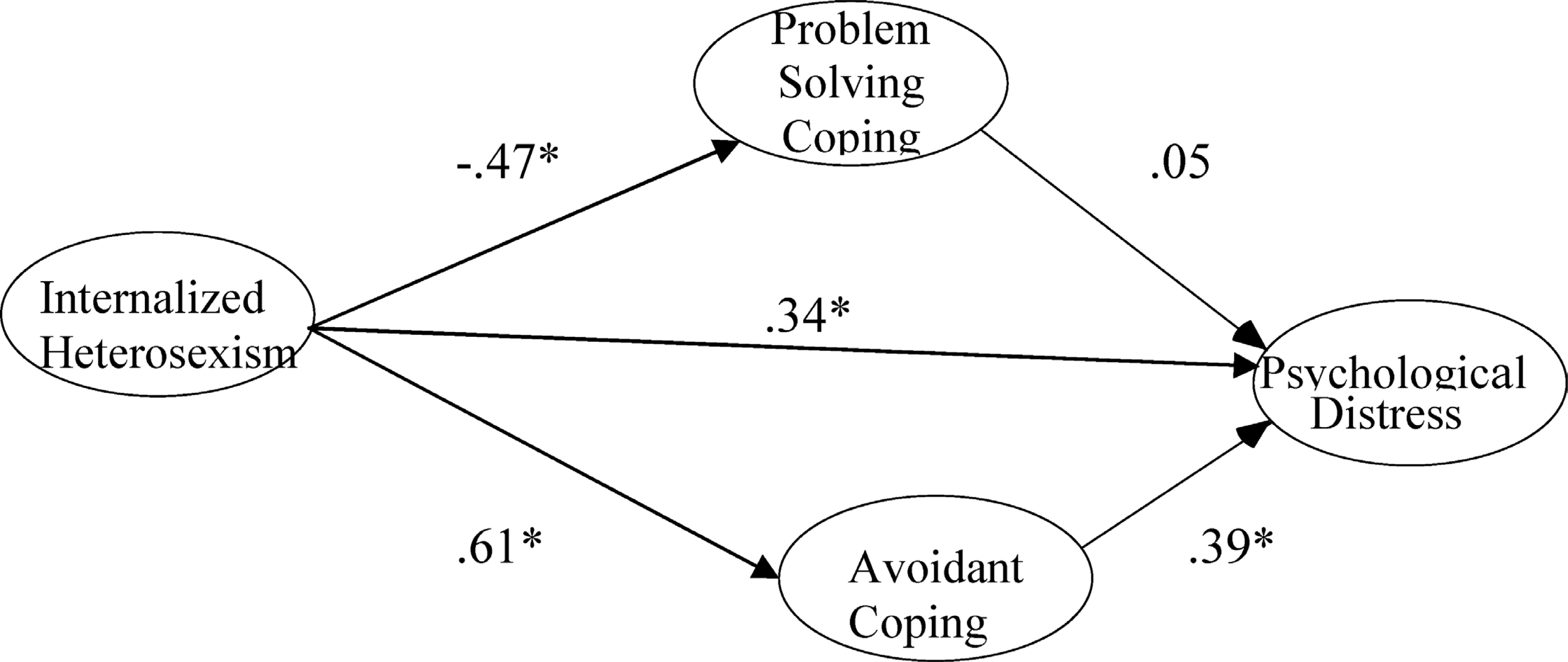
Relations among latent variables for the partially mediated model of internalized heterosexism to psychological distress. Note: All coefficients are standardized values. ∗p < .001.
DISCUSSION
This study aimed to test competing tenets of minority stress and lesbian feminist/sexual identity development theories by examining the potential moderating and mediating roles of individual coping styles (i.e., problem-solving and avoidant coping) in the relationship between internalized heterosexism and lesbian and bisexual women's psychological distress. The findings reveal that internalized heterosexism does not interact with problem-solving or avoidant coping in accounting for variance in psychological distress above and beyond their main effects. Our results suggest that, among lesbian and bisexual women, internalized heterosexism is negatively related to mental health regardless of an individual's coping styles. Thus, the moderated effect predicted by this aspect of minority stress theory is not supported.
Consistent with lesbian feminist/sexual identity development theories, our study found that avoidant coping partially mediates the relationship between internalized heterosexism and psychological distress. Thus, not only does internalized heterosexism directly affect psychological distress, it also appears that this relationship is partly based on internalized heterosexism's degradation of coping skills. Thus, individuals who experience high degrees of internalized heterosexism may be more likely to engage in avoidant coping strategies, which in turn results in poorer mental health. This finding suggests that interventions designed to decrease clients’ internalization of heterosexism may be important in helping to decrease both clients’ avoidant coping and their psychological distress.
Szymanski (2005a) and Kashubeck-West et al. (in press) describe several feminist strategies that may be useful for clinicians working with clients to reduce internalized heterosexism. These include (a) facilitating clients’ awareness of their internalized heterosexism by asking questions about their coming-out stories, their own thoughts and feelings about homosexuality, experiences with external heterosexism, self-disclosure of their sexual identity to others, and level of interaction with other LGB persons; (b) attending to the socio-cultural context and exploring the negative impact of heterosexism on the lives and presenting problems of lesbian and bisexual women clients; and (c) challenging internalized heterosexism by teaching clients cognitive methods to test the validity of their beliefs; using feminist analyses of heterosexual privilege, oppression, sexuality, and gender-role messages; providing factual information or affirmative readings about lesbianism/bisexuality; and identifying LGB role models.
Consistent with lesbian feminist/sexual identity development theories, we found that internalized heterosexism was related to less use of problem-solving coping. In the bivariate analyses, the full scale and two (active coping and planning) of the three subscales of problem-solving coping were negatively related to psychological distress; however, when internalized heterosexism, avoidant coping, and problem-solving coping were examined concurrently in predicting psychological distress, problem-solving coping was no longer related to psychological distress. In addition, no support was found for the mediating role of problem-solving coping in the link between internalized heterosexism and psychological distress. This pattern suggests that problem-focused coping styles may be less important than dysfunctional coping styles in contributing to psychological distress levels. It could also be that our sample as a whole scored higher on the scale of problem-solving coping compared to avoidant coping, and this range restriction may have attenuated the relationship between problem-solving coping and psychological distress in our study. Alternatively, other factors, such as community coping and social supports, may be more important than problem-solving coping strategies in predicting psychological distress levels. The method of Internet sampling also may have contributed to this finding, as individuals who have Internet access may be more connected to LGB social supports, which may in turn increase their use of problem-focused coping resources.
The correlational and cross-sectional nature of this study precludes definitive answers about the causal sequence proposed in our model. In addition, it is important to acknowledge that the mediational relationships found in this study might not have been evident if other variables that cause problem-solving coping, avoidant coping, and psychological distress had been included in the model. Longitudinal research is needed to establish a cause-and-effect relationship among internalized heterosexism, avoidant coping, and psychological distress. In addition, future research might examine other potential mediators, such as connection with feminist or women's communities and degree of outness, in the relationship between internalized heterosexism and psychological distress.
As is typical in research samples of LGB individuals, participants in this study were largely White, well educated, and willing to self-identify as lesbian or bisexual. Because participants are self-selected, those who responded may be more out in their communities and feel more connected with the LGB supports in their communities and therefore may have lower levels of distress and internalized heterosexism in general. Future research would benefit from including more diverse samples, not only in terms of race and ethnicity, but also with degree of outness and connectedness to the LGB community. Several strategies may help to increase diversity, such as use of non-Internet surveys that can be administered at local agencies offering LGB services, offering financial incentives to all participants for survey completion, and conducting targeted recruitment through community resources frequented by these groups. In addition, questions about internalized heterosexism might be included on a general survey of women's mental health. Recruiting participants from the general population, rather than through their association with the lesbian and bisexual communities or other sexual minority persons, might reach individuals who are less out (Szymanski, Chung, & Balsam, 2001). Finally, our study is limited by the low reliability for scores on the COPE Mental Disengagement subscale. Future research examining the mediational model proposed in the current study using different methods of assessing coping are needed.
Although there are many similarities among lesbian and bisexual women based on their gender and sexual minority statuses, there are also unique differences. For example, bisexual women need to acknowledge and affirm both the same-sex and heterosexual components of their identities (Fox, 2000). Furthermore, bisexual women must deal with external and internalized bisexism in addition to dealing with external and internalized heterosexism (Fox, 2000; Guidry, 1999). Thus, separate research is needed on bisexual women to address their unique identities and issues and to examine the impact of both bisexism and heterosexism on bisexual women's lives (Szymanski et al., in press a). The current study, as well as the studies by McGregor et al. (2001) and Szymanski and Kashubeck-West (in press) consisted of sexual minority female samples; therefore, results may not generalize to gay and bisexual men. Future research is needed to investigate whether avoidant coping styles, along with social support, also mediate the relationship between internalized heterosexism and psychological distress in gay and bisexual men. Finally, Meyer (2003) asserted that individual and group-level coping resources, although they may operate together to help an individual cope with minority stress, are not the same construct. Therefore, future research is needed to examine community coping and supports (e.g., sense of community with other LGBT individuals and involvement in anti-oppression activities) to further test these elements of minority stress theory. In addition, research using larger sample sizes to increase the statistical power of detecting interactions with small effect sizes is needed.
In conclusion, the current study provides one more step in the accumulating body of research that has examined the relationship between internalized heterosexism and mental health. Our study extends prior research by testing a more comprehensive, theoretically driven framework that included the potential moderating and mediating roles of individual coping styles in the link between internalized heterosexism and lesbian and bisexual women's psychological distress. Results supported a partially mediating but not a moderating role of avoidant coping in the relationship between internalized heterosexism and psychological distress.