
Abstract
Fredrickson and Roberts (1997) proposed objectification theory as an integrative framework for understanding how women's socialization and experiences of sexual objectification are translated into mental health problems. This article reviews the past decade of research grounded in objectification theory and highlights needed directions for future scholarship in this area. Specifically, this article reviews research organized according to the following themes: (a) self-objectification and its proposed consequences, (b) sexual objectification experiences as a proposed precursor, and (c) disconnections from bodily functions. An overview of emerging objectification theory research with men is also provided. The review concludes with needed directions for future theoretical and research efforts aimed to advance the psychology of women.
Fredrickson and Roberts (1997) proposed objectification theory as an integrative framework for understanding how women's socialization and experiences of sexual objectification are translated into mental health problems: mainly, eating disorders, depression, and sexual dysfunction, each of which is more prevalent among women than among men. Since the publication of this influential theory, research on its tenets has resulted in important advances in understanding women's experiences and mental health. At this decade milestone, researchers and practitioners committed to the psychology of women can benefit from a consolidation of existing knowledge and articulation of needed directions for future research on objectification theory. To this end, this article provides an integrative review of extant research grounded in this framework and highlights needed directions for future scholarship to advance the psychology of women. An overview of the theory and its key constructs is provided next, followed by a review of the literature and recommendations for future research.
OBJECTIFICATION THEORY AND ITS KEY CONSTRUCTS
Objectification theory posits that women's life experiences and gender socialization routinely include experiences of sexual objectification. According to Bartky (1990):
Sexual objectification occurs when a woman's sexual parts or functions are separated out from her person, reduced to status of mere instruments, or else regarded as if they were capable of representing her. To be dealt with in this way is to have one's entire being identified with the body… (p. 35).
An example of sexual objectification is the objectifying gaze that can occur in interpersonal encounters and media representations of women (Fredrickson & Roberts, 1997; Goffman, 1979; Kilbourne & Jhally, 2000). Diary studies support the routine occurrence of sexual objectification as a dimension of daily experiences of sexism, and, as posited in objectification theory, women report more sexual objectification experiences than do men (Swim, Hyers, Cohen, & Ferguson, 2001).
Within the framework of objectification theory, sexual objectification experiences are thought to socialize girls and women to treat themselves as objects to be looked upon and evaluated based upon bodily appearance (Fredrickson & Roberts, 1997). This internalization of an observer's perspective upon one's own body is called self-objectification. Self-objectification is manifested by persistent body surveillance, or the act of “habitual monitoring of the body's outward appearance” (Fredrickson & Roberts, 1997, p. 180). Appearance-focused self-objectification and manifest body surveillance parallel McKinley and Hyde's (1996) earlier conceptualization of body surveillance as a component of objectified body consciousness. Self-objectification and manifest body surveillance are posited to promote body shame and anxiety and reduce or disrupt awareness of internal bodily states and flow experiences (Fredrickson & Roberts, 1997). Body shame is the emotion that can result from measuring oneself against an internalized or cultural standard and perceiving oneself as failing to meet that standard. Anxiety includes the anticipation of threats and fear about when and how one's body will be evaluated. Peak motivational states, or what Csikszentmihalyi (1982, 1990) called flow, are “rare moments during which we feel we are truly living, uncontrolled by others, creative and joyful” (Fredrickson & Roberts, 1997, p. 183). Awareness of internal bodily states is the ability to detect and accurately interpret physiological sensations, such as stomach contractions and physiological sexual arousal.
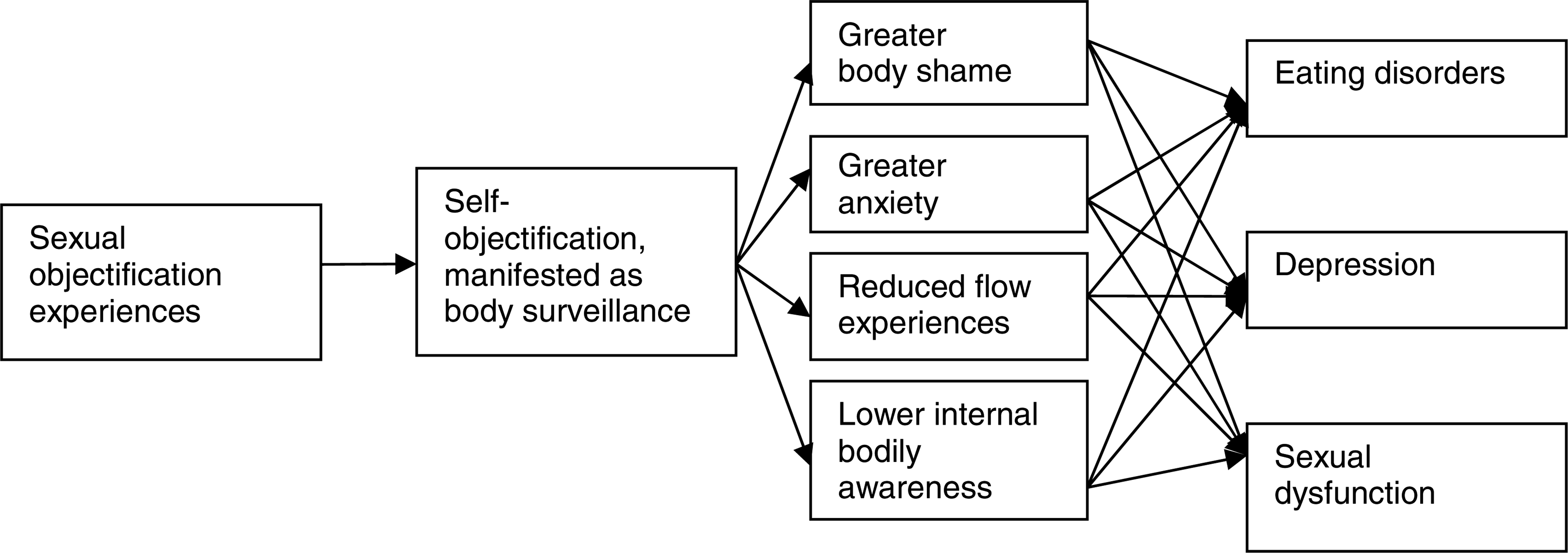
Objectification theory framework.
Objectification theory posits that women's gender-role socialization and sexual objectification experiences promote self-objectification and body surveillance. Self-objectification and body surveillance, in turn, promote body shame and anxiety and reduce or interfere with flow and awareness of internal bodily states. This chain of relations ultimately contributes to women's risk for depression, sexual dysfunction, and eating disorders (Fredrickson & Roberts, 1997). This framework (see Figure 1) has resulted in a proliferation of psychological research and advancements in understanding women's experiences and mental health. We review the past decade of research on objectification theory in this article. To set the stage for this review, we first discuss two important considerations: approaches for operationalizing self-objectification and within-group similarities and differences among women on objectification theory variables. The discussion of these considerations is followed by a review of the literature.
State and Trait Self-Objectification
Prior literature reflects two approaches to operationalizing self-objectification. One approach is to manipulate the level of self-objectification by exposing participants to a sexually objectifying or control situation and then evaluate the impact of this manipulation on criterion variables. As will be described in the proceeding sections, a number of manipulations have been effective in heightening women's body shape and size cognitions, which are typically assessed with Fredrickson, Roberts, Noll, Quinn, and Twenge's (1998) sentence completion task. Such experimentally heightened self-objectification has been referred to as state self-objectification.
The second approach to operationalizing self-objectification is to assess self-reported levels of self-objectification or body surveillance. Self-objectification is typically measured with Noll and Fredrickson's (1998) Self-Objectification Questionnaire (SOQ), which operationalizes the construct as the difference between participants' perceived importance of appearance versus competence-based body attributes. Another typical approach is to use the Body Surveillance subscale of McKinley and Hyde's (1996) Objectified Body Consciousness scale (OBC) or its adolescent version (OBC-Youth; Lindberg, Hyde, & McKinley, 2006) to assess level of reported habitual body monitoring. Such self-reports of self-objectification, or its manifestation as body surveillance, have been referred to as trait self-objectification. SOQ and OBC scores have demonstrated acceptable reliability and validity; however, an important consideration is that, when self-objectification and body surveillance are considered together, body surveillance typically emerges as uniquely related to criterion variables and self-objectification does not (e.g., Greenleaf & McGreer, 2006; Szymanski & Henning, 2007; Tiggemann & Kuring, 2004; Tiggemann & Lynch, 2001; Tiggemann & Slater, 2001). This pattern of results suggests that body surveillance subsumes the relations of general self-objectification with other variables. Thus, body surveillance seems important to assess and include in objectification theory research.
Another important consideration is the use of trait and state terminology in discussing self-objectification. Specifically, use of the terms “state” and “trait” self-objectification helps to distinguish contextually heightened self-objectification from intrapersonal individual differences in self-objectification. An important limitation to this terminology, however, is that the term “trait” has been used traditionally to define characteristics that are viewed as stable across time and situations; these characteristics are potentially biologically based and thus are difficult to modify (e.g., Block, 1995; John & Srivastava, 1999). As such, referring to self-objectification as a trait perpetuates the impression that it is innate, enduring, and resistant to interventions, rather than an experience that is sustained by and sensitive to contextual experiences of sexual objectification. A trait view also contradicts data pointing to the temporal instability of body surveillance (McKinley, 2006b). Thus, to circumvent the limitations of implying that self-objectification is a trait that is innate and difficult to modify, we refer to self-reported and experimentally heightened, rather than trait or state, self-objectification and body surveillance.
Within-Group Comparisons Among Women
Within-group comparisons suggest a number of subgroup similarities on objectification theory variables. Specifically, White and non-White women report similar levels of sexual objectification experiences, self-objectification, body surveillance, and body shame (Harrison & Fredrickson, 2003; Kozee, Tylka, Augustus-Horvath, & Denchik, 2007; Moradi, Dirks, & Matteson, 2005). Similarities have also emerged between heterosexual and sexual orientation minority women on levels of sexual objectification experiences, body shame, and internal bodily awareness (Downs, James, & Cowan, 2006; Kozee & Tylka, 2006). Nevertheless, in more specific group comparisons, some differences have emerged on body surveillance. For example, in a sample of low-income women, body surveillance was higher among European American women than among Latina or African American women and was higher among United States-born Latina women than among Latina women who moved to the United States at a later age (Breitkopft, Littleton, & Berenson, 2007). Body surveillance was higher also among lesbian women than among heterosexual women in one study (Kozee & Tylka, 2006) but similar between heterosexual and bisexual exotic dancers in another study (Downs et al., 2006). When women and men were considered together, self-objectification was higher among Hispanic participants and lower among African American participants than among other groups (Hebl, King, & Lin, 2004).
Taken together, group comparisons point to many similarities on key objectification theory constructs, but some group differences have emerged as well. Mixed results of group comparisons should be interpreted in light of the fact that samples were sometimes small and typically composed of college students. Also, some studies conflated group membership with other factors such as recruitment method. Future group comparisons can build on these studies by articulating and evaluating the underlying reason for hypothesized group comparisons. For instance, if minority women are hypothesized to exhibit lower levels of self-objectification because they are thought to engage in less internalization of majority cultural ideals of beauty, it is important that such internalization be assessed and that its link with self-objectification across groups be examined.
REVIEW OF THE LITERATURE
This review focuses on published research on women's experiences and mental health that is grounded in objectification theory. We identified the research to be reviewed by searching the PsycInfo database for records that cited Fredrickson and Roberts (1997) or included “self-objectification” or “objectification theory.” We focused on published research because the unpublished work that we identified (e.g., dissertations, conference presentations) overlapped substantially with the published literature. Three broad themes emerged from our review of objectification theory research about women's experiences, and the following sections are organized according to these themes. First, we review research on self-objectification and its consequences because this research has served as groundwork for other areas of objectification theory research. Next, we review research on sexual objectification experiences as the proposed precursor to other objectification theory constructs. This research grew from the research on self-objectification and its consequences and examines the role of sexual objectification experiences. Third, we review research on the links of objectification theory variables with disconnections from the body and its functions. In these three sections, we focus primarily on the application of objectification theory to women. In addition, we include a fourth section to introduce emerging research on the application of objectification theory to men. The review of literature is followed by a discussion of directions for future research on objectification theory.
Self-Objectification and Proposed Consequences
Experimental Findings Regarding Self-Objectification and Proposed Consequences
Body image and eating-related consequences. A number of studies have examined causal links between self-objectification and its proposed body-image and eating-related consequences. Most of these studies manipulated the salience of self-objectification by having some women try on a swimsuit (i.e., heightened self-objectification) and others try on a sweater (i.e., control) in front of a full-length mirror. Consistent with tenets of objectification theory, in such studies, heightened self-objectification raised women's levels of body shame, general shame, and body-related thoughts (Fredrickson et al., 1998; Quinn, Kallen, & Cathey, 2006). Furthermore, the impact of heightened self-objectification on body shame was stronger for women with high levels of reported self-objectification than for women with low levels of reported self-objectification, and body shame and reported self-objectification each were linked with restrained eating of cookies and chocolate (Fredrickson et al., 1998). Importantly, Fredrickson et al. (1998) assessed the criterion variables while participants were wearing the swimsuit, whereas Quinn, Kallen, and Cathey (2006) assessed the criterion variables after participants redressed. Thus, Quinn, Kallen, and Cathey's (2006) findings demonstrate that the impact of heightened self-objectification lasts beyond the immediate objectifying situation. Although participants in these samples were predominantly White or of unknown racial/ethnic composition, experimentally heightened self-objectification has also increased body-related thoughts and body shame in racially/ethnically diverse college women (Hebl et al., 2004; Quinn, Kallen, Twenge, & Fredrickson, 2006). In Hebl et al.'s (2004) sample, however, heightened self-objectification did not impact state self-esteem or amount of chocolate eaten.
In two additional studies with predominantly White participants, self-objectification was heightened by using sentence priming to elicit objectifying words (Roberts & Gettman, 2004) or by leading women to believe that they were going to interact with a male stranger (Calogero, 2004). These studies replicated the impact of heightened self-objectification on body shame and also found that heightened self-objectification increased appearance anxiety. However, heightened self-objectification was not associated with reported intent to diet (Calogero, 2004). Thus, experimental findings with predominantly White and racially/ethnically diverse women link heightened self-objectification with body shame, but not consistently with eating restraint.
Performance consequences. In addition to examining body and eating-related criterion variables, several studies have examined the impact of self-objectification on performance-related variables, used as a proxy for concentration or flow. For example, Fredrickson et al. (1998) found that, with baseline math ability controlled, women in the swimsuit condition performed worse on a math test than did women in the sweater condition. Parallel results emerged in math performance with racially/ethnically diverse college women and men (Hebl et al., 2004), and in a color-naming task with racially/ethnically diverse college women (Quinn, Kallen, Twenge et al., 2006). In a quasi-experimental study in which self-objectification was not manipulated, Fredrickson and Harrison (2005) found that racially/ethnically diverse high school girls' reported level of self-objectification was related negatively with quality of softball throwing, after controlling for prior sports and softball experience, age, and Anglo American status. Overall, findings of this set of studies suggest that self-objectification may hinder task performance.
In contrast to these findings, however, with racially/ ethnically diverse college women, Gapinski, Brownell, and LaFrance (2003) found that heightened self-objectification through overhearing objectifying comments or through wearing a swimsuit did not impact motivation, self-efficacy, or cognitive task performance; however, women in the swimsuit condition did report more unpleasant emotions than did women in the sweater condition. Despite the lack of expected self-objectification effects, Gapinski et al. (2003) presented findings suggesting that reported self-objectification may interact with situationally heightened self-objectification to impact performance, but small sample sizes and elimination of one-third of the sample in these analyses make interpretations of these results tentative.
Other findings point to situational and intrapersonal intervening variables in the self-objectification-performance link. Specifically, with a sample of White college women, Kiefer, Sekaquaptewa, and Barczyk (2006) found a significant interaction of solo status by appearance stigmatization, such that solo women (led to believe that they were the only woman in the group) with stigmatized appearance (led to believe a widened picture of them was being shown to other group members) scored lower on a recall test than did all other groups. However, stigmatized versus neutral appearance did not impact the performance of women with nonsolo status, and solo versus nonsolo status did not impact the performance of women in the neutral appearance condition. Additional analyses suggested that the effects of solo status and stigmatized appearance on performance were mediated by the extent to which participants reported feeling that their performance could confirm negative stereotypes about women. Thus, Kiefer et al.'s (2006) findings point to solo status and threat of confirming anti-woman stereotypes as important intervening variables that can shape the link of self-objectification with performance outcomes.
Summary of experimental findings. Taken together, findings of experimental studies are consistent with a primary tenet of objectification theory regarding the positive association between self-objectification and body shame. Specifically, the data suggest that heightened self-objectification promotes body shame in primarily White and racially/ethnically diverse samples of women. Also, heightened self-objectification has been shown to increase appearance anxiety and negative affect, but these relations have not been submitted to as many experimental tests as has the link between self-objectification and body shame. Furthermore, data generally suggest that heightened self-objectification hinders task performance, although intermediary variables, such as solo status and threat of confirming anti-woman stereotypes, might shape the relation between self-objectification and performance. Finally, experimental findings raise questions about the association between situational self-objectification and eating behaviors.
Importantly, experimental studies differed in whether they considered covariates in their design and analyses. If experimental studies intend to isolate the effects of situationally heightened self-objectification, then controlling for covariates such as body mass index (BMI) and preex-perimental levels of self-objectification seems important. In addition, mixed findings regarding eating behavior may have been shaped by differences across studies in the size of food offered (e.g., full-sized chocolate bar versus M&Ms) and whether food restriction was operationalized categorically (e.g., less that one chocolate bar versus one or more chocolate bars) or continuously (e.g., number of M&Ms eaten). Notably, restricted eating of cookies and candy is not equivalent to unhealthy food restriction that is characteristic of eating disorders, and objectification theory posits a number of intervening processes in the translation of sexual objectification and self-objectification into eating problems. Correlational studies, reviewed next, examine such direct and indirect relations with mental health indicators.
Correlational Findings Regarding Self-Objectification and Proposed Consequences
Links with body image and eating problems. Correlational studies link objectification theory variables with body image concerns. For instance, predominantly White college women's body shame was linked with propensity to change their body through weight change or cosmetic surgery (Forbes, Jobe, & Revak, 2006; Henderson-King & Henderson-King, 2005). In these studies, body surveillance was also associated with desired change in body weight, but not with interest in cosmetic surgery. This pattern is consistent with the posited proximal role of body shame in links with criterion variables, but also highlights the need to explore indirect relations of self-objectification or body surveillance, through body shame, with criterion variables.
Focusing more directly on eating disorder symptoms, two studies with Australian women who were White or whose race/ethnicity was not reported, linked self-objectification, body surveillance, and body shame with such symptoms (Burney & Irwin, 2000; Prichard & Tiggemann, 2005). A third study with a racially/ethnically diverse sample of Canadian women found that a composite variable comprised of body surveillance, body shame, and the belief that one can control one's body shape and size accounted for unique variance in eating pathology above and beyond the tendency to suppress negative affect (Piran & Cormier, 2005). In this study, however, collapsing body surveillance and body shame into a single variable masked the potentially distinctive roles of these variables posited in objectification theory.
In a noteworthy study with African American college women, Buchanan, Fischer, Tokar, and Yoder (2008) considered both general and group-specific manifestations of body surveillance and body dissatisfaction. Their results supported a model in which skin tone surveillance was linked uniquely and positively with skin tone dissatisfaction and body shame. Beyond the role of skin tone surveillance, body shape and size surveillance was linked uniquely and positively with body shame, but not with skin tone dissatisfaction. Also, beyond skin tone and body surveillance, self-objectification was not related to body shame, pointing to the importance of the surveillance variables. Thus, in this study, skin tone surveillance was a unique correlate of African American women's skin tone dissatisfaction and body shame, highlighting the need to consider group-specific manifestations of body surveillance in future research.
Most correlational objectification theory studies on body image and eating disorder variables have been cross-sectional, but some longitudinal data are available as well. For instance, McKinley gathered data from a cohort of predominantly White college students and their middle-age mothers in 1993 and again 10 years later (McKinley, 1998, 1999, 2006a, 2006b; McKinley & Hyde, 1996). Comparisons of levels of body surveillance and body shame across groups and data collection waves yielded notable patterns. Specifically, at Wave 1, college women reported higher levels of body surveillance and body shame than did middle-age women (McKinley, 2006b) and college men (McKinley, 2006a). At Wave 2, gender differences in body surveillance and body shame persisted (McKinley, 2006a), but the cohort differences between college and middle-age women disappeared, due to significant reductions in college women's body surveillance and body shame across data collection waves (McKinley, 2006b).
In these longitudinal studies, notable patterns also emerged in the relations among objectification theory variables. Specifically, at Wave 1 of data collection, body surveillance and body shame were correlated negatively with body esteem for college women and men, but only body shame was correlated with body esteem for middle-age women (McKinley, 1998, 1999, 2006a, 2006b; McKinley & Hyde, 1996). At Wave 2, the negative correlations of body surveillance and body shame with body esteem persisted for college women, but only body shame was correlated with body esteem for college men and middle-age women (McKinley, 2006a, 2006b). This pattern of findings points to body surveillance and body shame as stable correlates of body esteem for young women. For young men and middle-age women, however, body shame may be a more stable correlate of body esteem than is body surveillance. This may be because body shame clearly has a negative valence for all groups and as such is conceptually similar to body esteem. However, body surveillance may be more neutral in valence for young men and middle-age women than it is for young women. Indeed, correlations between body surveillance and body shame were higher for young women than they were for young men and middle-age women (McKinley, 2006a, 2006b). Importantly, despite the longitudinal nature of the data in these studies, interpretations regarding directionality of relations cannot be made. Cross-lagged relations, which compare the magnitude of prospective predictor-criterion and criterion-predictor relations while controlling for baseline covariation, are needed to elucidate directional relations of body surveillance and body shame with criterion variables.
Longitudinal data are also available from a 2-month study with a small group of predominantly White women in yoga classes (Impett, Daubenmier, & Hirschman, 2006). Reasoning that yoga practice might reduce self-objectification, Impett, Daubenmeier, & Hirschman (2006) found that body surveillance decreased from pre- to post-study; however, levels of awareness of and responsiveness to bodily sensations did not change. Impett, Daubenmeier, & Hirschman (2006) used hierarchical linear modeling to examine associations among intraindividual changes in body surveillance, bodily awareness and responsiveness, and psychological well-being over the 2-month period. The overall pattern of results from these analyses did not suggest significant relations among the variables. These null findings should be interpreted cautiously, however, because sample sizes for these analyses were 19 or smaller.
Additional studies have examined the roles of self-objectification and its proposed consequences in the co-occurrence of eating problems and smoking. Specifically, levels of body surveillance and body shame were higher for smoking than for nonsmoking groups of predominantly White college women (Fiissel & Lafreniere, 2006; Harrell, Fredrickson, Pomerleau, & Nolen-Hoeksema, 2006). Also, self-objectification, body surveillance, and body shame were linked positively with body dissatisfaction and eating disorder symptoms across smoker and nonsmoker groups (Fiissel & Lafreniere, 2006; Harrell et al., 2006). Importantly, body shame accounted for unique variance in weight control motives for smoking (Fiissel & Lafreniere, 2006), and self-objectification significantly mediated the positive link between smoking and eating disorder symptoms (Harrell et al., 2006). Thus, self-objectification and body shame may play a role in the co-occurrence of smoking with body image and eating problems.
Links with depressive symptoms. In addition to body image and eating pathology, depressive symptoms are another posited mental health outcome in the objectification theory framework and have received some research attention. Specifically, a number of studies point to unique relations of objectification theory variables with depressive symptoms, beyond other relevant constructs. For example, studies with racially/ethnically diverse samples of adolescent girls found that self-objectification was uniquely linked with body shame, eating disorder symptoms, depressive symptoms, and lower self-esteem when demographic characteristics were considered concomitantly (Harrison & Fredrickson, 2003; Tolman, Impett, Tracy, & Michael, 2006). Similarly, in a sample of predominantly White college women, with body dissatisfaction and personality factors controlled, a self-objectification and body surveillance composite variable accounted for unique variance in a depression composite variable that also included body shame (Miner-Rubino, Twenge, & Fredrickson, 2002). Also with predominantly White college women, a body surveillance and body shame composite was related uniquely to depression, restrictive eating, and bulimia symptoms when level of emotional awareness was considered concomitantly (Muehlenkamp & Saris-Baglama, 2002). Important to highlight is that body shame was subsumed in the depression composite in Miner-Rubino et al.'s (2002) study but was subsumed in the body surveillance composite in Muehlenkamp and Saris-Baglama's (2002) study. This inconsistency raises concern about construct contamination and leaves unexamined the posited mediating role of body shame.
Links with psychological well-being. Additional studies have examined the relation of objectification theory variables to indicators of psychological well-being. For example, body surveillance and body shame were found to correlate negatively with predominantly White college women's self-esteem and health-promoting behaviors (Aubrey, 2006b; Befort et al., 2001; Fiissel & Lafreniere, 2006; Hayman et al., 2007; Lowery et al., 2005). Similarly, findings in both data collection waves of McKinley's (2006a, 2006b) studies supported expected negative associations of body surveillance and body shame with positive self-appraisal for young cohorts of women and men, but only body shame was correlated consistently with self-esteem for middle-age women. Directional relations among these variables remain unclear, however, because cross-lagged relations were not examined in the longitudinal data.
In contrast to the former studies, results regarding the relations of body surveillance and body shame with self-esteem were mixed with racially/ethnically diverse college women and exotic dancers (Downs et al., 2006). Specifically, with age controlled, body surveillance and body shame were not correlated significantly with self-esteem for college women, but were correlated negatively with self-esteem for exotic dancers, who reported significantly higher levels of body surveillance and body shame than did college women. Importantly, nearly half of the exotic dancers, compared to one-quarter of the student sample, were White. Thus, examining the role of race/ethnicity may have been important in light of consistent findings of racial/ethnic group differences on self-esteem (e.g., Gray-Little & Hafdahl, 2000; Twenge & Crocker, 2002).
Whereas the previous studies focused on self-esteem or positive self-appraisal, Sinclair and Myers (2004) assessed psychological well-being multidimensionally. They found that White college women's reports of body surveillance and body shame were correlated negatively with coping well-being (self-worth, leisure, and stress management), and body shame was correlated negatively with creative well-being (sense of control, thinking, emotions, humor, and work). However, body shame and body surveillance were not correlated with interpersonal or physical well-being. Surprisingly, body surveillance was correlated positively with “essential self,” which encompasses spirituality, self-care, gender, and cultural identity. This last finding should be interpreted cautiously because, based on data challenging the construct validity of essential self, this construct has been revised to reflect only spiritual well-being (Myers, Luecht, & Sweeney, 2004), and body surveillance and body shame were not correlated significantly with predominantly White college women's spirituality (Hayman et al., 2007).
The pattern of findings in Sinclair and Myers's (2004) study, and in the self-esteem-focused studies, links body surveillance and body shame with lower self-worth for mostly White college women. Results are mixed, however, with racially/ethnically diverse samples and when other dimensions of psychological well-being are considered. Importantly, low sense of self-worth is a central aspect of depression, whereas other aspects of well-being (e.g., creative well-being) may be associated with but are not directly reflective of depression. Thus, the fact that body surveillance and body shame are linked more consistently with self-worth than with other aspects of well-being fits with objectification theory's focus on depressive symptomatology.
Summary of correlational findings. Taken together, findings of correlational studies support the posited links of self-objectification, body surveillance, and body shame with indicators of women's mental health, including eating disorder symptoms, depressive symptoms, and self-esteem; however, links with sexual dysfunction remain to be examined. Furthermore, body shame's association with weight control motives for smoking and self-objectification's mediation of the link between smoking and eating disorder symptoms suggest that self-objectification and body shame may be underlying factors in the co-occurrence of eating pathology and smoking among women. Also, Buchanan et al.'s (2008) findings point to the importance of considering the relations of group-specific manifestations of surveillance (e.g., skin tone surveillance) with body shame and dissatisfaction. Across these studies, however, assumptions about direction of causality cannot be made due to the correlational nature of the data and lack of cross-lagged analyses in longitudinal data. Another important limitation in some correlational studies is that collapsing body surveillance with body shame into single composite indicators might have obscured the separate roles that objectification theory posits for these variables. Indeed, studies that examine mediated relations (reviewed next) yield results that are consistent with the separate roles of body surveillance and body shame posited in objectification theory.
Proposed Mediational Relations
Objectification theory posits a number of mediated relations, from sexual objectification experiences, through self-objectification or body surveillance and its emotional correlates, to mental health risks. Research on these proposed mediations is accumulating. Due to the cross-sectional nature of these studies, however, assumptions about direction of causality cannot be made. However, the data can be interpreted with regard to their consistency or inconsistency with the mediated relations posited in objectification theory.
Eating disorder symptoms as the criterion. Much of the research on mediated relations has focused on the role of body shame in the relations of self-objectification or body surveillance with eating disorder symptoms. In samples of predominantly White and racially/ethnically diverse college women, Noll and Fredrickson (1998) found that body shame partially mediated the link of self-objectification with eating disorder symptoms, such that self-objectification was related to greater body shame, which in turn was related to more eating disorder symptoms. These findings emerged with BMI controlled and when bulimia or anorexia symptoms were examined. Evidence consistent with the mediating role of body shame in the relation of self-objectification or body surveillance with eating disorder symptoms has emerged in other samples of adolescent and adult women; ballet dancers and nondancers; and women diagnosed with eating disorders who were White, predominantly White, or of unreported race/ethnicity (e.g., Calogero, Davis, & Thompson, 2005; Greenleaf, 2005; Slater & Tiggemann, 2002; Tiggemann & Kuring, 2004; Tiggemann & Slater, 2001).
In a test of objectification theory with predominantly White Deaf women, Moradi and Rottenstein (2007) replicated the proposed mediating role of body shame. They also considered the additional role of marginal Deaf cultural identity attitudes, which reflect participants' experience of tension and conflict between Deaf and hearing cultures and identities. Results of a path analysis that tested direct and indirect relations indicated that body shame mediated the links of body surveillance and internalization of cultural standards of beauty with eating disorder symptoms. In addition, marginal Deaf identity attitudes were linked indirectly with greater body surveillance, body shame, and eating disorder symptoms through internalization of cultural standards of beauty. There was also a positive direct link between marginal Deaf identity attitudes and eating disorder symptoms in this model. Like Buchanan et al.'s (in press) findings, Moardi and Rotten-stein's (2007) findings point to the importance of considering group-specific experiences within the objectification theory framework and also suggest that the posited roles of body surveillance and body shame are generalizable to Deaf women.
Whereas available data are consistent with the mediating role of body shame, studies that examined the proposed mediating roles of appearance anxiety, awareness of internal bodily states, and flow have yielded mixed support for mediation. For example, appearance anxiety was related uniquely to eating disorder symptoms in a racially/ethnically diverse sample of college women and Australian samples of young to older adult women whose race/ethnicity was not reported (Greenleaf & McGreer, 2006; Tiggemann & Kuring, 2004; Tiggemann & Lynch, 2001). By contrast, appearance anxiety was not related uniquely with eating disorder symptoms (i.e., it did not meet a precondition for mediation), in adolescent, adult, and college women who were White, predominantly White, or of unreported racial/ethnic background (Slater & Tiggemann, 2002; Tiggemann & Slater, 2001). Available data also are not consistent with the mediating roles of awareness of internal bodily states or flow experiences in the links of self-objectification or body surveillance with eating disorder symptoms in samples of women who were racially/ethnically diverse, predominantly or exclusively White, or of unknown race/ethnicity (Daubenmier, 2005; Greenleaf, 2005; Greenleaf & McGreer, 2006; Tiggemann & Kuring, 2004; Tiggemann & Slater, 2001). Importantly, Daubenmier (2005) assessed both awareness of and responsiveness to bodily messages and found that only responsiveness to bodily messages mediated the positive association between self-objectification and eating disorder symptoms. Thus, being unresponsive to bodily messages, rather than lack of awareness of such messages, may serve as a mediator.
Depressive symptoms as the criterion. As with eating disorder symptoms, when depressive symptoms are considered as the criterion variable in the objectification theory framework, data are generally consistent with the mediating role of body shame in the relations of self-objectification or body surveillance with eating disorder symptoms. Specifically, in samples of women who were predominantly White or of unknown racial/ethnic background, data were consistent with the mediating role of body shame in the positive relation of body surveillance with depressive symptoms (Muehlenkamp, Swanson, & Brausch, 2005; Szymanski & Henning, 2007; Tiggemann & Kuring, 2004). Support for this pattern emerged in a 2-year longitudinal study with predominantly White girls as well (Grabe, Hyde, & Lindberg, 2007). Muehlenkamp et al. (2005) also examined, but did not find support for, parallel chains of relations with sex- and drug-related risk behaviors or self-harm behaviors as the criterion variables. In addition to the mediating role of body shame, data from two studies were consistent with a potential mediating role of appearance anxiety, contradicted the mediating role of awareness of internal bodily states, and were mixed regarding the mediating role of flow, in the relation of body surveillance with depressive symptoms (Tiggemann & Kuring, 2004; Szymanski & Henning, 2007).
Summary and methodological caveats. Available findings are consistent with the posited mediating role of body shame in the relations of self-objectification or body surveillance with eating disorder and depressive symptoms. In contrast, most available findings raise questions about additional unique relations of awareness of internal bodily states, flow, and appearance anxiety with eating disorder or depressive symptoms. This pattern of findings should be interpreted with a number of caveats in mind. First, most studies on proposed mediations have been conducted with predominantly White samples, and research with women from diverse backgrounds is needed to evaluate the generalizability of extant findings. Second, many studies did not test the significance of mediation. Instead, mediation was interpreted based on a series of significant unique relations or a reduction in the predictor-criterion relation after the mediator was accounted. These practices have been critiqued, and preferred procedures for testing the significance of mediation have been outlined (Frazier, Tix, & Barron, 2004; Mallinckrodt, Abraham, Wei, & Russell, 2006). These preferred procedures should be used in objectification theory research. Third, most objectification theory research on mediation is cross-sectional, and longitudinal research is needed to examine temporal directions in proposed mediations.
Finally, there are notable consistencies in the measurement of most variables included in mediation studies, but there is inconsistency in measurement of flow. Specifically, self-objectification and body surveillance typically were assessed with the Self-Objectification Questionnaire (Noll & Fredrickson, 1998) and the Body Surveillance subscale (McKinley & Hyde, 1996), respectively. Body shame typically was assessed with the Body Shame subscale (McKinley & Hyde, 1996) or, sometimes, with the Body Shame Phenomenology scale (Fredrickson et al., 1998). Appearance anxiety typically was assessed with the Appearance Anxiety Scale (Dion, Dion, & Keelan, 1990) or the Social Physique Anxiety Scale (Hart, Leary, & Rejeski, 1989). Awareness of internal bodily states typically was assessed with the Body Awareness Questionnaire (Shields, Mallory, & Simon, 1989) or the Private Body Consciousness Scale (Miller, Murphy, & Buss, 1981). By contrast, approaches to operationalizing flow have varied. Some authors used selected subscales of the Flow State Scale (Jackson & Marsh, 1996), some used the Flow Trait Scale (Jackson, Kimiecik, Ford, & Marsh, 1998), some developed study-specific measures (e.g., Tiggemann & Slater, 2001), and Szymanski and Henning (2007) developed a new measure. The breadth of these measures ranges from a narrow focus on concentration to assessing multiple dimensions that include concentration, loss of self-consciousness, balance between challenge and skills, goal clarity, and other aspects of flow. Importantly, the only study that supported the unique link of flow with depressive symptoms assessed intense concentration, loss of self-consciousness, and sense of skill development and goal accomplishment (Szymanski & Henning, 2007). All three dimensions of flow were correlated with self-objectification and body surveillance, but only loss of self-consciousness and sense of skill development/goal accomplishment were correlated with depression. Thus, concentration was unrelated to the criterion variable in objectification theory's proposed chain of mediation. In light of these findings, future tests of mediation should consider potentially distinctive roles of various dimensions of flow in the objectification theory framework.
Sexual Objectification Experiences as Proposed Precursor
A growing number of studies have attended to sexual objectification experiences as the proposed precursor to self-objectification or body surveillance and their correlates within the objectification theory framework. Some of this research is informed by work on objectified body consciousness (McKinley, 1998, 1999; McKinley & Hyde, 1996), which closely parallels self-objectification in that it is defined as the tendency to view oneself as an object, includes body surveillance and body shame components, and is posited to result from sexual objectification experiences and promote eating problems. The research on sexual objectification experiences also builds on broader literature that links body image and eating problems with specific forms of sexual objectification, such as thinness pressures, sexual harassment, sexual abuse, and subtle and covert sexual objectification (e.g., Connor-Greene, Striegel-Moore, & Cronan, 1994; Field, Camargo, Taylor, Berkey, & Colditz, 1999; Groesz, Levine, & Murnen, 2002; Jacobi, Hayward, de Zwann, Kraemer, & Agras, 2004; Larkin, Rice, & Russell, 1996; Murnen & Smolak, 2000; Piran, 1998; Stice, 2002; Weiner & Thompson, 1997). Studies grounded in objectification theory build on this important prior work to elucidate the intervening variables through which sexual objectification experiences may be linked with body image and eating problems.
Links of Sexual Objectification Experiences With Objectification Theory Variables
Sexual objectification experiences are those experiences that reduce a girl or woman to her sexual body parts or body functions (Bartky, 1990). Examples of sexual objectification experiences include the objectifying gaze that can occur in interpersonal encounters, as well as appearance evaluations, cat calls, or inappropriate sexual comments (Fredrickson & Roberts, 1997; Goffman, 1979; Kilbourne, 2000; Swim et al., 2001). Researchers have used experimental exposure to a specific manifestation of heightened sexual objectification or gathered self-reported perceptions of sexual objectification experiences to examine the direct and indirect relations of this variable with other objectification theory constructs.
As described previously, different experimental manipulations have been effective in heightening self-objectification in women. Because many of these manipulations involve exposing women to appearance pressures that can heighten sexual objectification, the findings of these studies can be interpreted as tests of the consequences of inducing sexual objectification. For instance, the typically used manipulation of wearing a swimsuit in front of a mirror clearly heightens appearance pressure. Similarly, exposure to men's gaze (Calogero, 2004) and overhearing objectifying comments (Gapinski et al., 2003), each of which are identified as manifestations of sexual objectification (Fredrickson & Roberts, 1997; Swim et al., 2001), also have been manipulated in experimental studies. As such, the previously reviewed impact of such experimental manipulations on self-objectification and its proposed consequences can be interpreted as support for the notion that inducing sexual objectification through appearance pressures promotes self-objectification as posited in objectification theory.
Additional studies have assessed girls' and women's reported experiences of pressures to be thin as a specific manifestation of sexual objectification experiences. Data from these studies indicate that reported experiences of weight-related criticism, thinness pressures, and sexual and appearance-related harassment are associated positively with body surveillance and body shame in samples of predominantly White college women and young girls (Befort et al., 2001; Lindberg et al., 2006; Lindberg, Grabe, & Hyde, 2007; Tylka & Hill, 2004). Furthermore, data with predominantly White women and girls suggest that reported experiences of appearance pressure are linked indirectly, through body surveillance, with greater body shame (Lindberg et al., 2007; Tylka & Hill, 2004). In addition to these links, Tylka and Hill (2004) found that body surveillance and body shame each were related to lower awareness of internal bodily states and that body shame and lower awareness, in turn, were related to greater eating disorder symptoms. Thus, as posited in objectification theory, studies that assess thinness-related pressures and harassment link such experiences with greater body surveillance and body shame and with lower bodily awareness. Also, experiences of appearance pressures may be related indirectly to eating disorder symptoms through body surveillance, body shame, and low internal bodily awareness.
In addition to studies that focus on thinness pressures, a number of studies have examined type of sports participation as a proxy for sexual objectification experiences. For example, Parsons and Betz (2001) calculated sports objectification scores that reflected participants' level of sports participation weighted by the appearance and femininity focus of the sports. With a sample of predominantly White college women, they found that, when body surveillance, indicators of perceived personal agency, and perceived control over one's body and weight were accounted for, body shame was related uniquely and positively to sports objectification scores. Similarly, with a sample of racially/ethnically diverse adolescent girls, Harrison and Fredrickson (2003) found that participation in lean sports (i.e., sports that emphasize weight and appearance) was related positively with self-objectification and eating disorder symptoms after controlling for grade in school, racial/ethnic minority status, and BMI. By contrast, nonlean sports participation was related negatively with self-objectification and was unrelated to eating disorder symptoms. Taken together, these studies suggest that appearance-focused sports participation may be linked with greater self-objectification, body surveillance, body shame, and eating disorder symptoms. To the extent that appearance-focused sports promote exposure to sexual objectification, this pattern of findings is consistent with the posited role of sexual objectification experiences within the objectification theory.
Exposure to sexually objectifying media also has been linked positively with self-objectification, body surveillance, body shame, and appearance anxiety in samples of college women and men who were predominantly White or whose race/ethnicity was not reported (Aubrey, 2007; Monro & Huon, 2005). Furthermore, body surveillance mediated the positive links of objectifying media exposure with body shame and appearance anxiety (Aubrey, 2007). Retrospective data suggest that childhood media exposure might be particularly important (Slater & Tiggemann, 2006), but this possibility requires longitudinal examination. In fact, longitudinal data point to a bidirectional relation between exposure to objectifying media content and self-objectification for predominantly White women and men, suggesting that exposure to objectifying media can promote self-objectification, and self-objectification can promote future avoidance of objectifying media (Aubrey, 2006a, 2006b). Similarly, data with predominantly White women suggest that high body shame may promote future avoidance of objectifying media (Aubrey, 2006b). When body surveillance was considered instead of general self-objectification, however, only prospective links from objectifying media exposure to body surveillance were found (Aubrey, 2006a). Thus, the link of objectifying media exposure with general self-objectification might be bidirectiononal, but the link of objectifying media exposure to body surveillance may be prospective.
Notably, the type of exposure that impacts self-objectification may be shaped by targets' racial/ethnic status. Specifically, Harrison and Fredrickson (2003) compared White girls with non-White girls of various racial/ethnic minority backgrounds and found that, among White girls, self-objectification was higher for those who viewed a women's lean sports video compared to those who viewed videos of men's sports or women's nonlean sports. However, among non-White girls (most of whom were African American/Black), self-objectification was higher for those who viewed women's nonlean sports videos compared to those who viewed videos of women's lean sports or men's sports. As such, the extent to which images of women's lean and nonlean sports were experienced as sexually objectifying may have differed between White and non-White girls. Perhaps images in women's lean sports were self-relevant to White girls and images in nonlean sports were self-relevant to the mostly African American/Black non-White girls due to trends of higher average BMI for African American/Black women than for White women (e.g., Seo & Torabi, 2006).
The research reviewed thus far links various manifestations of sexual objectification experiences (i.e., experimentally heightened and self-reported appearance pressures, appearance-focused sports participation, and exposure to objectifying media) with self-objectification or body surveillance and their correlates. Accumulating data also suggest that internalization of cultural standards of beauty, or the extent to which one adopts cultural standards of beauty as one's own, is an important intervening variable to consider in the relations of sexual objectification experiences with other objectification theory constructs. Specifically, studies have supported unique associations of internalization of cultural standards of beauty with self-objectification, body surveillance, body shame, body dissatisfaction, and eating disorder symptomatology in samples of college women who were predominantly White or whose race/ethnicity was not reported and in predominantly White women diagnosed with eating disorders (Calogero et al., 2005; Morry & Staska, 2001; Sinclair, 2006; Myers & Crowther, 2007). Also, when considered together, sexual objectification experiences and internalization both accounted for unique positive variance in body shame, and internalization also accounted for unique positive variance in body surveillance (Sinclair, 2006). Similarly, exposure to or awareness of objectifying media was linked with greater internalization of cultural standards of beauty, and internalization in turn was linked with greater self-objectification, body dissatisfaction, and eating disorder symptomatology (Morry & Staska, 2001; Myers & Crowther, 2007). In addition, type of exercise motivation (i.e., exercising for beauty rather than fitness or enjoyment reasons) mediated the relation of self-objectification with body satisfaction and self-esteem in samples of Australian women who were White or whose race/ethnicity was not reported (Strelan & Hargreaves, 2005a; Strelan, Mehaffey, & Tiggemann, 2003). Thus, internalization of cultural standards of beauty appears to be an important correlate of self-objectification, body surveillance, body shame, and eating problems and may play an important role in the objectification theory framework.
Building on such findings, Moradi et al. (2005) examined the role of internalization of cultural beauty standards in testing objectification theory with a sample of predominantly White college women. They assessed self-reports of sexual objectification experiences identified in Swim et al.'s (2001) diary studies and found that internalization mediated links of sexual objectification experiences with body surveillance, body shame, and eating disorder symptoms. In addition, body surveillance mediated the link of sexual objectification experiences with body shame, and body shame in turn mediated the links of internalization and body surveillance with eating disorder symptoms. With another sample of predominantly White college women, Myers and Crowther (2007) found that internalization of cultural standards of beauty mediated the link of awareness of objectifying media with body dissatisfaction, and self-objectification mediated the link of internalization with body dissatisfaction. These patterns are consistent with the chain of mediations proposed in objectification theory among sexual objectification experiences, body surveillance, body shame, and eating disorder symptoms. These findings also point to internalization of cultural beauty standards as an additional mediator of the relation of sexual objectification experiences with body surveillance, body shame, and eating disorder symptoms.
Finally, Kozee et al. (2007) advanced measurement of sexual objectification experiences by developing the Interpersonal Sexual Objectification Scale (ISOS), which assesses women's experiences of sexual objectification in interactions with partners, family, or friends. With two samples of predominantly White college women, Kozee et al. (2007) found that interpersonal sexual objectification experiences reflected two major factors: body evaluation and unwanted explicit sexual advances. In another sample of predominantly White college women, these sexual objectification experiences accounted for unique variance in body surveillance and internalization of the thin ideal, and a body surveillance and internalization composite variable mediated the link of sexual objectification experiences with body shame (Kozee et al., 2007). Furthermore, using the ISOS with samples of lesbian and heterosexual college women who were predominantly White, Kozee and Tylka (2006) found support for the posited chain of relations among sexual objectification experiences, body surveillance, body shame, internal awareness of bodily states, and eating disorder symptoms. Among lesbian women, significant direct links of sexual objectification experiences with body shame, internal awareness, and eating disorder symptoms also were found that did not emerge for heterosexual women. Thus, the direct and indirect relations of sexual objectification experiences with body image and eating disorder symptoms appear to vary across some subgroups of women. Overall, findings from this series of studies by Kozee and her colleagues provide support for the posited role of sexual objectification experiences in objectification theory and support the generalizability of the framework to lesbian women.
Although most of the studies reviewed thus far focused on negative experiences and outcomes, a unique study by Avalos and Tylka (2006) explored the relations among experiences of body acceptance from others, body surveillance, and healthy intuitive eating. These authors found that body surveillance significantly mediated the link between experiencing body acceptance and intuitive eating, such that acceptance by others was linked negatively with body surveillance, which in turn was linked negatively with intuitive eating. Thus, in addition to its observed role in body image and eating problems, body surveillance may also play a role in the relations of positive body-related experiences with healthy body image and eating.
Taken together, available data about sexual objectification experiences suggest that self-objectification, body surveillance, and internalization of cultural beauty standards mediate the links of sexual objectification experiences with psychological risk factors and eating disorder symptoms. These data are largely cross-sectional and were drawn predominantly from White women. Thus, longitudinal research and studies with diverse samples are needed to test the directional role of sexual objectification experiences and the observed mediators. Research also is needed to test the relations of sexual objectification experiences with depressive symptoms and sexual dysfunction.
Evidence of Moderation
Additional studies suggest that self-objectification or body surveillance may intensify the link of sexual objectification exposure with criterion variables. For example, with predominantly White college women, Henderson-King, Henderson-King, and Hoffman (2001) found that high self-objectifiers exposed to idealized images reported poorer body image than did high self-objectifiers exposed to neutral images, but low self-objectifiers exposed to idealized or neutral images did not differ. Also, a three-way interaction indicated that, among those exposed to idealized images, high self-objectifiers who overheard a conversation critical of another women's appearance reported lower state self-esteem compared to high self-objectifiers who overheard a neutral conversation; parallel differences did not emerge among low self-objectifiers. Thus, exposure to sexually objectifying images and conversations may have greater impact on high self-objectifiers than on low self-objectifiers.
Several additional studies point to the moderating role of self-objectification or body surveillance as well. For example, in a sample of predominantly White college women, body surveillance moderated the relation of body dissatisfaction with eating disorder symptoms, such that the link between body dissatisfaction and eating disorder symptoms was positive for those with high levels of body surveillance, but not significant for those with low levels of body surveillance (Tylka, 2004). Similarly, in a sample of college women whose race/ethnicity was not reported, exposure to idealized bodies resulted in greater pre- to postexposure increase in appearance anxiety for high self-objectifiers than it did for low self-objectifiers (Monro & Huon, 2005). But, in another study with a sample of White college women, exposure to appearance-related magazine images had the expected impact of decreasing pre- to poststudy body esteem regardless of level of body surveillance or body shame (Hamilton, Mintz, & Kashubeck-West, 2007). In another sample of predominantly White college women, high self-objectifiers who received positive evaluation of their character or appearance reported lower negative mood than did high self-objectifiers who received a neutral evaluation; no differences emerged among low self-objectifiers (Fea & Brannon, 2006). These findings suggest that high self-objectification may intensify the impact of positive evaluation on mood, whether that evaluation focuses on appearance or not.
Overall, the findings of this set of studies suggest that self-objectification or body surveillance may intensify the impact of sexual objectification exposure on body image and eating disorder symptoms. This pattern suggests a damaging cyclical process in which sexual objectification exposure promotes self-objectification and its proposed consequences, which in turn intensify the impact of future sexual objectification.
Self-Objectification and Disconnection From the Body and Its Functions
Building on the objectification theory perspective that self-objectification reflects a focus on body appearance over body function, Roberts and Waters (2004) argued that sexual objectification experiences and resultant self-objectification can lead women to separate themselves from their own bodily sensations and functions. As such, some studies have examined links between objectification theory constructs and disconnection from the body and its functions.
Sex, Menstruation, and Breast-Feeding
A number of studies have focused on the link of self-objectification with sexual behaviors and attitudes. For example, heightened self-objectification reduced predominantly White college women's interest in physical aspects of sex, such as genital contact (Roberts & Gettman, 2004). Furthermore, in a sample of predominantly White college women and men, body surveillance, but not self-objectification, mediated the relations of sexually objectifying media exposure with appearance concerns during sexual intimacy (Aubrey, 2007). Also with predominantly White women, body shame was associated with greater appearance concern during sexual intimacy and with lower reported sexual pleasure and arousability (Sanchez & Kiefer, 2007).
Additional studies have examined links between self-objectification and sex-related behaviors. For instance, in a racially/ethnically diverse sample of 12th-grade girls, self-objectification was correlated negatively with amount of sexual experience, sense of efficacy to act upon one's own sexual needs, and condom use (Impett, Schooler, & Tolman, 2006). Qualitative interviews with a subsample of six participants suggested that girls with lower levels of self-objectification were comfortable in discussing sexuality and had engaged in sexual experimentation, whereas girls with higher levels of self-objectification were less comfortable and expressed regret about having engaged in sex (Hirschman, Impett, & Schooler, 2006). Similarly, data from another sample of racially/ethnically diverse college women indicated that a relation between menstrual shame and lower sexual assertiveness was mediated by body shame, and the relation of body shame with greater sexual risk taking and lower sexual behavior was mediated by sexual assertiveness (Schooler, Ward, Merriwether, & Caruthers, 2005). Thus, findings across these studies link self-objectification and body shame with menstrual shame and with nonassertive and risky sexual behaviors.
Schooler et al.'s (2005) findings regarding menstrual shame were replicated in a sample of predominantly White premenopausal women. Specifically, with age controlled, Roberts (2004) found that body shame, body surveillance, and self-objectification were generally correlated with negative attitudes and feelings, and not with positive attitudes or feelings, toward menstruation. Despite such links with negative attitudes and feelings, however, body shame, body surveillance, and self-objectification were not related to a sample of predominantly White college women's interest in reducing or eliminating their own menstruation (Johnston-Robledo, Ball, Lauta, & Zekoll, 2003). Similar findings emerge in studies about breast feeding. Specifically, in samples of predominantly White college women and low-income pregnant women, body shame, self-objectification, and body surveillance generally were correlated positively with embarrassment about breast-feeding, but not with perceived benefits of or with future plans regarding breast feeding (Johnston-Robledo & Fred, 2008; Johnston-Robledo, Wares, Fricker, & Pasek, 2007). Findings across these studies suggest that self-objectification, body surveillance, and body shame are associated with negative attitudes and feelings about menstruation and breast-feeding, but are not related to interest in eliminating menstruation or breast feeding.
Additional evidence suggests that gender-schematic individuals' (i.e., those who describe themselves with gender stereotypic traits) objectification of women as a group may increase when menstruation is made salient. Specifically, with a sample of predominantly White college students, Roberts, Goldenberg, Power, and Pyszczynski (2002) manipulated the salience of menstruation by having a confederate woman accidentally pull out a tampon or a hair clip from her bag. They measured objectification of women by modifying the SOQ, originally designed to assess self-objectification, to assess the extent to which participants evaluated women's bodies in objectifying ways. Gender schematic participants exposed to the tampon condition objectified women more than did gender aschematic participants exposed to the tampon condition and participants exposed to the hair clip condition. Perhaps, menstruation is particularly threatening to gender schematic persons because they are invested in maintaining an objectified construal of women in which sexiness is prominent. Indeed, the sexual objectification of other women and men is linked with self-objectification for both women and men (Strelan & Hargreaves, 2005b), although stronger correlations are observed for women (r = .50s and .60s) than for men (r = .20s).
Mortality Salience and Out-of-Body Experiences
A few studies have used objectification theory as a framework for studying mortality salience and out-of-body experiences. Studies on mortality salience attempt to integrate objectification theory with terror management theory. Terror management theory posits that, when mortality is made salient, individuals are motivated to protect their cultural values and self-esteem in an effort to insulate themselves against the threat of mortality. Based on this theoretical assumption and the additional reasoning that self-objectification and objectification of women are dominant cultural values, clinging to self-objectification and objectification of women is posited to serve as a defense against the threat of mortality. What remains unclear in this reasoning is why protecting cultural values or self-esteem would protect against mortality salience or why adhering to self-objectification and objectification of women, rather than other more general core values, would be protective. Nevertheless, Grabe, Routledge, Cook, Andersen, and Arndt (2005) found that mortality salience increased women's self-objectification and objectification of other women and also intensified the link between self-objectification and self-worth value placed on attractiveness. The same pattern of findings was not observed when dental pain was made salient rather than mortality, suggesting that something unique about the salience of mortality underlies the pattern of observed findings. On the other hand, Goldenberg, McCoy, Pyszczynski, Greenberg, and Solomon (2000) found that high self-objectifiers with low body esteem actually reported lower body surveillance when mortality was made salient, reasoning that, for those who do not feel good about their bodies, body consciousness may not be protective when faced with mortality salience.
Although extant data generally support links between objectification theory constructs and disconnection from specific body functions, Murray and Fox (2005) examined, but did not find, links between objectification theory variables and more general body disconnection. Specifically, they found that individuals (race/ethnicity not described) who reported having had an out-of-body experience reported greater body dissatisfaction than those who did not report an out-of-body experience; but the two groups did not differ on body surveillance, body shame, or appearance anxiety. Thus, these findings support the distinctiveness of objectification theory constructs from general bodily dissociation.
Taken together, available data link objectification theory constructs with indicators of disconnection from bodily functions. Specifically, data suggest that heightened self-objectification reduces interest in sexual behavior and that body shame is associated with nonassertive and risky sexual behaviors, greater appearance concern during sexual intimacy, and lower reported sexual pleasure and arousability. Furthermore, self-objectification, body surveillance, and body shame are related to negative attitudes and feelings about menstruation. Also, reminders of menstruation might intensify gender schematic participants' objectification of women as a group, and reminders of mortality might intensify both objectification of women as a group and self-objectification. Notably, these findings point to self-objectification and its proposed consequences as important variables to consider in how women approach sexual and menstrual health. Clarifying the roles of objectification theory variables in women's behaviors related to sex and menstruation (e.g., condom use) can point to new targets for interventions aimed to promote women's health.
Objectification Theory and Men's Experiences
Much of the research on objectification theory has focused on women's experiences. Nevertheless, some research points to the promise of objectification theory for understanding men's experiences as well. In this section, we highlight some findings regarding the application of objectification theory to men. Importantly, most available data suggest that men and boys report lower self-objectification, body surveillance, and body shame than do women and girls (e.g., Aubrey, 2006a; Grabe et al., 2005; Hebl et al., 2004; Lindberg et al., 2006; Lowery et al., 2005; McKinley, 1998, 2006a). However, African American women and men did not differ in level of body shame, and Asian American men reported higher self-objectification than did Asian American women (Hebl et al., 2004). The general pattern of gender differences across studies, however, is consistent with objectification theory's focus on omnipresent sexual objectification of women and its internalization as self-objectification or body surveillance.
Although expected gender differences emerge in levels of self-objectification and related constructs, available data suggest gender similarities in relations of objectification theory constructs with some criterion variables. For example, consistent with the pattern of findings for women and girls, self-objectification, body surveillance, and body shame generally are correlated significantly and negatively with body esteem, self-esteem, and health-promoting behaviors for men and boys (Lindberg et al., 2006; Lowery et al., 2005; McKinley, 1998, 2006a; Strelan & Hargreaves, 2005a); and the correlation between body shame and body esteem persisted at a 10-year follow-up for both genders (McKinley, 2006a). Also, as with women and girls, men's body shame is linked with greater appearance concern during sexual intimacy and with lower reported sexual pleasure and arousability (Sanchez & Kiefer, 2007), and boys' sexual objectification exposure is linked with body surveillance and body shame (Lindberg et al., 2006; Lindberg et al., 2007). Gender similarities also are evident in proposed mediated relations. For instance, as with women, men's body surveillance significantly mediated the relations of objectifying media exposure with body shame, appearance anxiety, and appearance concerns during sexual intimacy (Aubrey, 2007). Also, consistent with findings with women, data with men suggested that body shame and appearance anxiety, but not flow or awareness of internal bodily states, might mediate the relation of body surveillance with eating disorder symptoms (Tiggemann & Kuring, 2004). Statistical comparison of effect sizes is typically not conducted in these studies, but visual inspection suggests that the magnitudes of relations are similar for women and men in most cases, somewhat higher for women in some cases (e.g., Lowerly et al., 2005; McKinley, 1998), and somewhat higher for men in a few cases (e.g., McKinley, 2006a).
Additional findings suggest that some relations observed with girls and women are not significant when examined with boys and men. For example, self-objectification was not related to men's body dissatisfaction (Strelan & Hargreaves, 2005b), and body surveillance was not related to body esteem at a 10-year follow-up (McKinley, 2006a) or to concurrent self-esteem (Lowery et al., 2005). Also, body surveillance was linked with body shame for both girls and boys, but body shame mediated the positive relation of body surveillance with depressive symptoms only for girls (Grabe et al., 2007). One caveat in interpreting some of these nonsignificant relations is that samples of men were substantially smaller than samples of women in some studies (i.e., Lowery et al., 2005; McKinley, 2006a), resulting in lower power to detect significant effects for men. This point is illustrated by Hayman et al.'s (2007) findings that correlations among body surveillance, body shame, self-esteem, and appearance dissatisfaction were generally similar in magnitude for women and men, but resulted in fewer significant correlations for men than for women.
By contrast, some notable links have emerged with men that have not emerged with women. Hayman et al. (2007) found that spirituality was correlated negatively with body surveillance and body shame for men, but the correlations were near zero and nonsignificant for women. Similarly, data were consistent with a possible mediating role of flow in the link of body surveillance with depressive symptoms for men but not for women (Tiggemann & Kuring, 2004). Spirituality and flow both have been conceptualized as components of or contributors to psychological well-being (e.g., Csikszentmihalyi, 1982, 1990; Hill & Pargament, 2003; Ryff, 1989). Thus, objectification theory constructs may be particularly important to explore in relation to men's psychological well-being.
Experimental findings regarding the impact of heightened self-objectification have yielded both gender similarities and differences. For example, in samples that were predominantly White or of unknown racial/ethnic composition, heightened self-objectification increased feelings of shame, disgust, appearance anxiety, and body-related thoughts and decreased math performance and appeal of sexual behavior for women but not for men (Fredrickson et al., 1998; Quinn, Kallen, & Cathey, 2006; Roberts & Gettman, 2004). Again, in some of these studies (i.e., Quinn, Kallen, & Cathey, 2006; Roberts & Gettman, 2004), sample sizes for men were smaller than for women. Furthermore, null findings with men may not generalize across racial/ethnic groups. Specifically, in a diverse sample of women and men, Hebl et al. (2004) found that, regardless of race or gender, those in the swimsuit condition had greater body shame and self-objectification and poorer math performance than did those in the sweater condition.
Also, null experimental findings for men should be interpreted in light of the possibility that situations that heighten self-objectification in women may not necessarily do so in men. Indeed, despite the null effect of the swimsuit condition on men's body shame, Fredrickson et al. (1998) found a positive link between men's reported self-objectification and body shame. Thus, self-objectification may be linked with body shame for men, but the type of situation that induces self-objectification may differ for women and men. Consistent with this possibility, Morry and Staska (2001) found that women's exposure to beauty magazines was linked with internalization of cultural standards of attractiveness, which in turn was linked to self-objectification, body dissatisfaction, and eating disorder symptoms. For men, however, exposure to fitness, but not beauty magazines, accounted for unique variance in internalization, which in turn accounted for unique variance in body dissatisfaction. Thus, beauty magazines may communicate cultural standards of desirability for women, whereas fitness magazines communicate such standards for men, and different standards may promote different manifestations of body surveillance and body shame (e.g., concern regarding thinness vs. muscular appearance).
Indeed, Hallsworth, Wade, and Tiggemann (2005) found that men who were bodybuilders scored higher on self-objectification compared to men who were weight lifters and to men who were neither bodybuilders nor weight lifters. Thus, appearance-focused bodybuilding may be associated with self-objectification for men. Hallsworth et al. (2005) also found that across participants in all groups, body surveillance was related uniquely and positively with appearance anxiety, but not with body shame. Both appearance anxiety and body shame were related uniquely and positively with depressive and bulimia symptoms, whereas appearance anxiety was related uniquely and positively with body dissatisfaction, and body shame was related uniquely and positively with drive for muscularity. Taken together, these findings are generally consistent with the objectification theory framework in that they link men's body surveillance, body shame, and appearance anxiety with indicators of eating disorder and depressive symptoms and also link men's self-objectification and body shame with pursuit of appearance-focused muscularity. Such findings highlight the need to attend to men's unhealthy pursuit of appearance-focused muscularity, and objectification theory provides a framework for such exploration.
Another promising area of investigation is application of objectification theory to gay and bisexual men. Such attention is important in light of data suggesting higher levels of body image concerns, eating disorder symptoms, and eating disorders among gay and bisexual men than among heterosexual men (e.g., Carlat, Camargo, & Herzog, 1997; Heffernan, 1994; Siever, 1994; Strong, Williamson, Netemeyer, & Geer, 2000). Indeed, with a sample of college men (race/ethnicity not reported), Martins, Tiggemann, and Kirkbride (2007) found that gay men reported higher levels of self-objectification, body surveillance, and body shame than did heterosexual men. Furthermore, body shame significantly mediated the relations of self-objectification with body dissatisfaction and drive for thinness but not drive for muscularity. However, mediated relations involving body surveillance were not examined. Overall, these data suggest that self-objectification, body surveillance, and body shame may be salient constructs for gay men, and the mediating role of body shame posited in objectification theory may generalize to gay men.
In an experimental study, Martins et al. (2007) found that manipulating self-objectification (i.e., wearing a Speedo or sweater) resulted in higher body surveillance for gay and heterosexual men in the heightened self-objectification condition than for those in the control condition. Also, body shame mediated the impact of experimental condition on gay men's dissatisfaction with lower body parts (e.g., stomach, pelvis, buttocks, thighs). Finally, gay men in the heightened self-objectification condition reported greater body shame and ate less Chex mix than did those in the control condition; heterosexual men in the two conditions did not differ on these criterion variables. The null findings regarding the impact of experimental condition on heterosexual men's body shame and eating behavior in this study parallel Fredrickson et al.'s (1998) findings that the swim-suit manipulation did not impact men of unknown sexual orientation's body shame or eating behavior. By contrast, Martins et al.'s (2007) findings with gay men parallel those with women in terms of levels of self-objectification, body surveillance, and body shame, the impact of heightened self-objectification, and the mediating role of body shame. Such similarities in findings with gay men and heterosexual women may reflect their shared experiences of anticipated or actual sexual objectification from men. Thus, attention to the role of sexual objectification experiences and their shared and unique manifestations for women and gay men seems important in future research.
Taken together, studies reviewed in this section highlight the promise of objectification theory for framing research on men's experiences. To this end, it is important to evaluate, rather than assume, construct equivalence for women and men. For example, research is needed to explore the nature of sexual objectification experiences for different groups of men and to identify unique experiences, such as drive for muscularity and internalized homophobia, that may need to be integrated into the framework. Research also is needed to evaluate aspects of the theory that remain unexamined with men, such as the roles of flow and appearance anxiety.
RECOMMENDATIONS AND FUTURE DIRECTIONS
The present review illustrates how research grounded in objectification theory has advanced psychology of women literature by elucidating links between women's sociocultural experiences, feelings about themselves and their bodies, and mental health outcomes. An overview of available findings is provided in Figure 2. This review highlights the rich body of research that has proliferated as a result of objectification theory and points to this framework as a critical paradigm in future scholarship on the psychology of women. Throughout this review we have discussed areas of research that need further attention and development. We highlight below recommendations that we view as particularly critical:
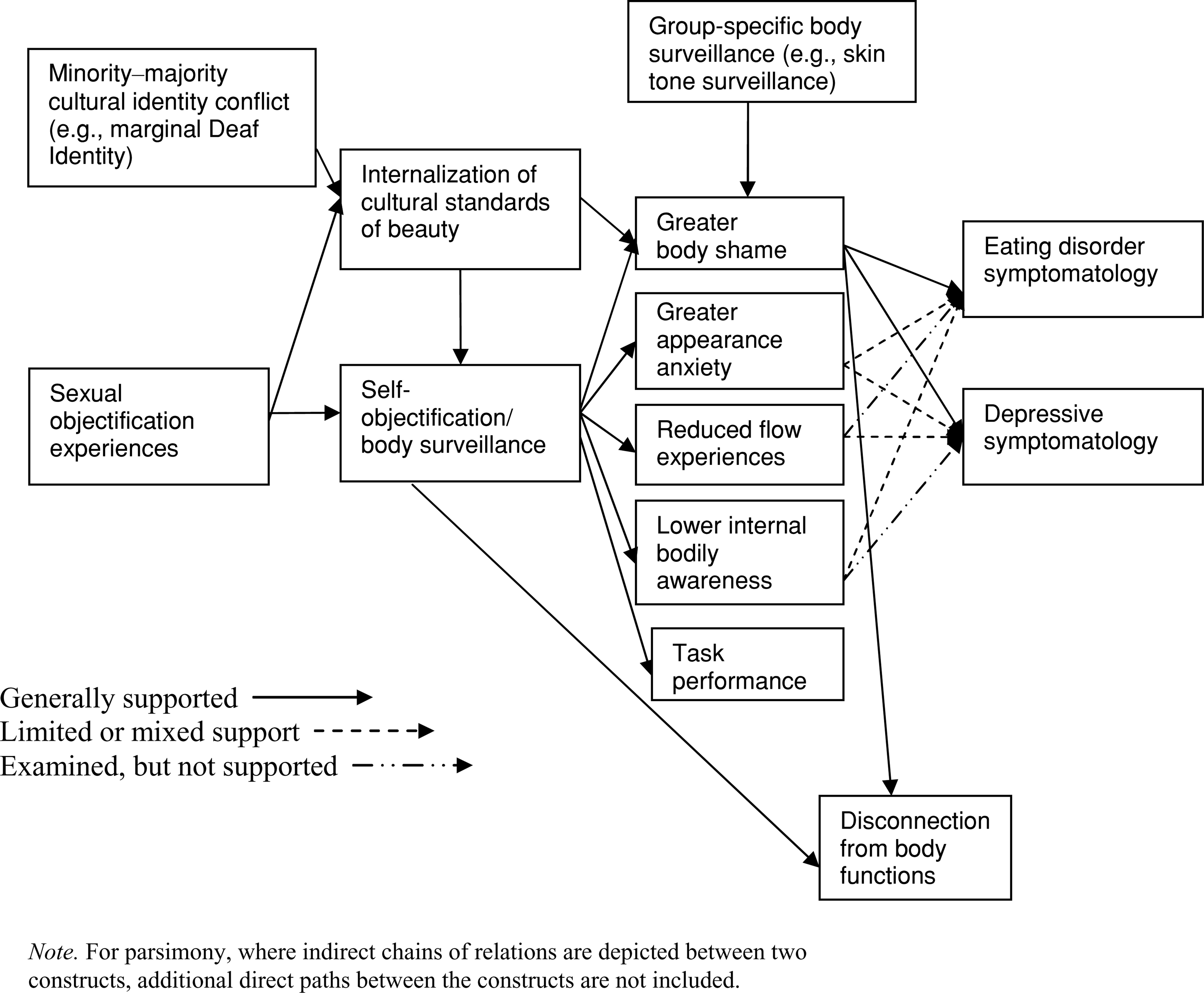
Overview of objectification theory relations examined in research with women.
Empirical support has accumulated for the basic tenets of objectification theory with predominantly White college women of unspecified sexual orientation. The utility of the theory needs to be tested with women who vary on racial/ethnic identity, sexual orientation, age, socioeconomic status, relationship status, and other background variables. Furthermore, studies should routinely describe these characteristics of their samples to inform judgments about the generalizability of findings. In addition to diversifying samples in objectification theory research, research is needed to evaluate the extent to which current conceptualizations and measures of objectification theory constructs adequately capture experiences of women from diverse backgrounds. For example, sexual objectification experiences communicate beauty standards of thinness to all women, but also communicate idealization of Whiteness, heterosexuality, able-bodiedness, and other dominant cultural characteristics (e.g., Greene, 1994). Current conceptualizations of body surveillance and body shame do not capture valuation of factors such as skin tone, hair texture, facial features, and sexual appeal to men. A notable exception is Buchanan et al.'s (2008) study that included skin tone surveillance. Such attention to group-specific manifestations of objectification theory constructs is needed to expand the utility of the theory to diverse populations of women.
Future research should attend to group-specific variables that need to be integrated into the objectification theory framework to extend its utility across diverse groups of women. The integration of marginal Deaf identity in Moradi and Rottenstein's (2007) study is one such example. Similarly, experiences of racism, heterosexism, and other forms of prejudice may intersect with sexual objectification experiences and should be considered in future research.
Most objectification theory studies are with samples from the United States and Australia. Research is needed to examine cultures in which women's bodies are treated with more, less, and different manifestations of objectification. For example, hijab in Muslim women's attire has been conceptualized both as a sign of sexual objectification of women as well as a sign of freedom from such sexual objectification (e.g., Afshar, 2000). Research with Muslim women could explore links of internalization of hijab standards with objectification theory variables. Such research can examine the cross-cultural generalizability of objectification theory and also point to modifications that can increase its cross-cultural applicability.
Fredrickson and Roberts (1997) conceptualized anxiety to include appearance anxiety, as well as anxiety related to the anticipation of danger or threats to one's safety. We did not identify any study that examined the posited role of safety anxiety within the objectification theory framework. Thus, future research should attend to safety anxiety, including anxiety about physical and sexual violence.
Operationalization of flow in objectification theory research can be advanced by attention to the broader literature on flow. In the broader literature, flow is conceptualized as (a) experiences associated with task performance, such as focused concentration, losing track of time, and sense of curiosity and (b) the balance between challenge and skills involved in a task (e.g., Shin, 2006; MacDonald, Byrne, & Carlton, 2006). The experience of pleasure and enjoyment are also fundamental emotional aspects of flow (e.g., Csikszentmihalyi, 1982, 1990). Task performance, which has been used as a proxy for flow in objectification theory research, may reflect the concentration aspect of flow, but does not capture other important experiential dimensions, such as pleasure. Self-report measures of flow that are used in objectification theory research also need to be evaluated with regard to how completely they capture the construct, including its emotional manifestation as pleasure.
Among the intermediary variables in the objectification theory framework, more research has been focused on self-objectification, body surveillance, and body shame than on anxiety, flow, or internal bodily awareness. Also, more research has attended to body image and eating disorder symptoms than to depression and sexual dysfunction as outcomes in the objectification theory framework. Studies that examine the full set of predictor and outcome variables can elucidate the relative importance of objectification theory variables for mental health outcomes. Such data, in turn, can focus future research, prevention, and intervention efforts on the most relevant predictors for each mental health criterion.
Across studies that examined self-objectification and body surveillance together, body surveillance was linked uniquely and consistently with criterion variables (e.g., Greenleaf & McGreer, 2006; Slater & Tiggeman, 2002; Tiggemann & Kuring, 2004; Tiggemann & Lynch, 2001; Tiggemann & Slater, 2001), whereas general self-objectification was linked uniquely only to some criterion variables, in some subsamples, in some studies (Greenleaf & McGreer, 2006; Szymanski & Henning, 2007; Slater & Tiggeman, 2002). Thus, assessing body surveillance is particularly important in future research.
Emerging evidence points to the importance of considering internalization of sociocultural standards of beauty as an intervening variable, in addition to self-objectification and body surveillance, in the relation of sexual objectification experiences to body shame and eating disorder symptomatology (e.g., Moradi et al., 2005; Morry & Staska, 2001). These findings are consistent with Fredrickson and Roberts's (1997) original conceptualization that a sexually objectifying culture pressures women to adopt cultural standards of beauty as their own standards for self-objectification and body surveillance. To the extent that these standards are internalized and not met (because they are impossible to meet), they can promote body shame and eating problems. Thus, explicating the role of internalization of cultural standards of beauty within the objectification theory framework and in future research seems warranted (see Figure 2).
In terms of methodology, most experimental studies have manipulated self-objectification and assessed resultant changes in body shame, eating behaviors, and other outcomes. To advance understanding of other causal chains posited in objectification theory, research is needed to experimentally manipulate other posited causal variables in the objectification theory framework, such as body shame, appearance anxiety, and flow, and examine their impact on subsequent outcomes. Similarly, further research is needed on sexual objectification experiences as the causal root in the objectification theory framework.
Correlational studies have been useful in examining multiple objectification theory variables together, but cross-sectional designs preclude evaluation of temporal changes and predictive relations among variables. Longitudinal designs and analyses are needed to address this gap.
Testing the significance of mediation should be routine in mediation studies (see Frazier et al., 2004; Mallinckrodt et al., 2006).
Some studies, not specifically grounded in objectification theory, have used measures of constructs parallel to those in objectification theory. Examples include the Appearance Orientation (Cash, 2000) and the Objectified Relationship With Body (Tolman & Porche, 2000) subscales, which assess appearance focus and monitoring, and the Social Comparison to Models and Peers (Jones, 2001, 2004) and the Physical Appearance Comparison (Thompson, Heinberg, & Tantleff, 1991) scales, which assess appearance comparison. These measures may assess constructs closely linked to self-objectification and body surveillance. Similarly, the Body Image Guilt and Shame Scale (Markham, Thompson, & Bowling, 2005) and the Somatic Awareness Questionnaire (Van Wijk & Kolk, 1996) appear to assess body shame and awareness of internal bodily states, respectively. Evaluating construct and measurement overlap can help to reduce proliferation of redundant measures and promote research that is informed by the full integration of prior knowledge about the constructs of interest. To this end, measures of key objectification theory constructs can be consolidated by identifying and integrating the strongest available measures or developing improved measures when needed. Development of the ISOS (Kozee et al., 2007) to consolidate prior approaches to measuring sexual objectification experiences is an example of such efforts.
Psychometric information, such as structure, reliability, and validity data about measures of key objectification theory constructs are limited mostly to White heterosexual college students. Thus, measurement evaluation with women of diverse backgrounds is needed.
Objectification theory was originally grounded in women's experiences, but available data lay the groundwork for further evaluations of the theory with men. To this end, it is important to explore the group-specific meaning and manifestations of objectification theory constructs with men.
Accumulating support for the posited roles of sexual objectification experiences, self-objectification, body surveillance, and body shame can provide the basis for group- and individual-level interventions. For example, activities that encourage women to be attuned to how their body feels and functions, rather than how it looks, might reduce appearance-focused body surveillance, which in turn might reduce body shame and eating disorder and depressive symptoms. Cognitive-behavioral interventions may help women to identify and resist sexual objectification experiences, body surveillance, and body shame. Interestingly, Choma, Foster, and Radford (2007) found that, compared to exposure to a video on wildlife, exposure to a video critical of media depictions of women actually increased body shape and size cognitions in predominantly White college women. Although the authors controlled for reported self-objectification in this analysis, they did not examine whether the two video groups differed in reported self-objectification. Evaluating the effectiveness of such interventions in reducing the risk factors posited in objectification theory can guide theoretically and empirically informed practice aimed to improve women's mental health.
CONCLUSION
Although some aspects of objectification theory need further investigation, particularly with more diverse samples of women, objectification theory and its growing research literature provide a promising framework for understanding how some sociocultural and psychological risk factors and mediators work together to shape aspects of women's mental health. Consistent with feminist conceptualizations, objectification theory and its growing body of research point to changes needed at the societal level (e.g., reducing sexual objectification of women) and also highlight potentially useful strategies at the individual level (e.g., reducing self-objectification) to reduce women's psychological distress. As such, existing and future research on objectification theory can serve as groundwork for understanding and promoting women's mental health and well-being by encouraging and advocating for societal and personal change.