
Abstract
Trust is a key component in the creation and maintenance of social capital, which has been linked to neighborhood capacity to respond to environmental challenges as well as physical and mental well–being of individuals. This article investigates the significance of this component of social capital for the health and well–being of African American residents of various types of neighborhoods. Using data collected from a sample of residents of neighborhoods characterized by differing levels of racial and economic segregation in a midsized southern city (N= 310), a psychosocial resources model of distress is employed to explore the role of trust as a critical resource mediating the impact of stress in the form of racial and economic segregation on residents’ well–being. Results show that minority saturation is a more important predictor of well–being than economic segregation, and that, though no mediating influence is found, generalized trust is an important predictor of well–being.
Research examining well–being issues specific to minority populations has tended to focus on the differences between Blacks and Whites, using explanations based on racial differences in demographic characteristics, socioeconomic status, or stress–related factors (Williams, Takeuchi, and Adair, 1992). Considering that systems of shared knowledge, beliefs, and patterns of social relations have often been shaped from the experiences of having minority status within the larger society (Schulz et al., 2000), it is surprising that few studies focus exclusively on minority groups and factors of specific salience to social and cultural experiences of minority populations. Likewise, few contemporary studies examine the effects of racial residential segregation on the well–being of minority–group members, focusing instead on the equally important topic of why racial residential segregation still exists (Krysan and Farley, 2002). Much segregation research assumes that racial residential segregation has negative consequences for ethnic minorities (Timberlake, 2002), but examinations of the effects have been mixed (Farley and Frey, 1994; Ovadia, 2003). While the persistence of racial residential segregation tends to elicit images of injustice and inequality in mainstream society, research has shown that the residential preferences of African Americans play a significant role in maintaining segregation, with preservation of black institutions accompanied by racial pride playing a lead role in influencing preference (Krysan and Farley, 2002). The current literature, then, may suggest that African American residents of segregated neighborhoods are experiencing a high degree of social cohesion and social embeddedness.
Examination of linkages between social embeddedness and individual well–being has historical significance in the sociological discipline (Durkheim, [1897] 1964). Currently, the dynamic study of social capital, an amplified perspective of social embeddedness, has gained momentum and popularity in urban and community studies, as well as in medical sociology. The majority of social capital research examines this resource at and above the community level (Portes, 1998; Putnam, 2000; Wilson, 1997). Social capital has been defined as the connections among individuals; more specifically as the social networks and norms of trustworthiness that arise from those connections (Mitchell and LaGory, 2002; Putnam, 2000). To understand the resource more thoroughly, current researchers are also focusing on these individual components of social capital, generally social support and social networks (Browning and Cagney, 2002; Mitchell and LaGory, 2002; Schieman, 2005). However, few contemporary studies have examined the impact of other individual components of social capital on the individual. Considering the previous studies of social capital and its components, their achievements and their challenges, this study examines one crucial component of this important resource: trust, and its effects on the well–being of individuals. As important as is the concept of social capital itself, the recognition of the necessity of trust in creating this resource should be a focus of social capital research.
The utility of social capital as a critical social resource is in its ability to create reciprocal binding and bridging network ties between members of a group (Mitchell and LaGory, 2002; Putnam, 2000; Schieman, 2005). Individuals can be civically engaged; they can be members of a vast number of voluntary organizations; they can be attuned to and concerned with the problems and needs of those around them and of their communities; they can have countless associations with others within and outside of their immediate environment, but without trust in others and the expectations and mutual obligations that trust carries, the positive effects of social capital cannot be realized.
This study examines these issues to address discrepancies apparent in the previous research on African American well–being. Considering the mixed results of segregation studies mentioned previously, I employ a traditional view of economic and racial residential segregation as an indicator of concentrated disadvantage (Ovadia, 2003). Utilizing a sample of 310 African American residents of several neighborhoods across the Birmingham, Alabama, Metropolitan Statistical Area, I examine the effects of this concentrated disadvantage on African American physical and mental well–being. I include levels of trust in others as a potential resource. Is residential segregation in the inner city a chronic stressor, as much previous research has implicitly and explicitly assumed it to be? Does the concentration of impoverishment and ethnic minorities within a neighborhood affect individual levels of trust in others? I also examine trust in others as a resource that can be used to mediate the potential negative effects of concentrated disadvantage on well–being.
Stress and Well–Being
The most consistently argued influence on individual well–being is the experience of stressors (Fitzpatrick and LaGory, 2000). Stressors are defined by Thoits (1995) as environmental, social, or individual circumstances that lead to stress. Aneshensel (1992) described this distress process as a state of arousal resulting either from the presence of socioenvironmental demands that tax the adaptive capacity of an individual or from the absence of the means to attain sought–after ends. Lin and Ensel (1989) focused on general external stimuli that might generate physiological and mental responses. Within the distress process, a stressor is any environmental, social, or internal demand that requires the individual to readjust usual behavior patterns or implement coping strategies. If the individual is not able to readjust behavior or cope with the stressor, there is a probability that illness, injury, disease, or psychological distress will follow (Thoits, 1995).
There are two major types of stressors recognized in studies of the distress process: life events and chronic strains (Pearlin, 1989). Life events may be positive or negative and include experiences like divorce, marriage, loss of a job, or the death of a loved one (Cockerham, 1998). Chronic strains are persistent or recurrent demands that require readjustments over prolonged periods of time (Thoits, 1995). Some major sources of chronic strains are physical disability, excessive or inadequate environmental demand, and social and economic impoverishment (Aneshensel, 1992). As a chronic strain, adverse socioeconomic circumstances in particular have the potential for long–lasting psychological and emotional damage (Fitzpatrick and LaGory, 2000). These stressors and their outcomes have been found to be influenced by the structural arrangements in which individuals are embedded (Pearlin, 1989; Turner, Lloyd, and Wheaton, 1995), and chronic stressors are most apparent in the lives of low–income African American residents of inner cities, who often experience a concentration of disadvantage.
Concentrated Disadvantage and Well–Being
A large amount of research has identified contextual neighborhood factors that are relevant in the study of health and well–being. Physical characteristics of place, like neighborhood disorder or maintenance of infrastructure, can be healthy or unhealthy for the individuals residing in that place (Fitzpatrick and LaGory, 2000). Contextual stressors, along with the neighborhood disorganization common in many poor, inner–city communities (Laveist, 1993), leave residents alienated from societal institutions that promote appropriate health and illness behaviors. This isolation leads to a decline in both physical health status and mental and emotional well–being (Fitzpatrick and LaGory, 2000). Although support for the concept of unhealthy places should be evident in this article, the goal of this research is not to show that the physical contexts of disadvantaged neighborhoods are unhealthy for their residents; the accumulation of literature convincingly supports this thesis. Rather, this study focuses on the effects of concentrated disadvantage in the form of economic and racial segregation of African Americans in the inner city. As mentioned previously, chronic stressors of inner–city minority residents, and their outcomes, are influenced by the structural arrangements in which individuals are embedded (Pearlin, 1989; Turner, Lloyd, and Wheaton, 1995). Therefore, I examine the sociostructural arrangement of the inner–city neighborhood as a potential stressor.
Concentrated disadvantage is conceptualized here as the extent of both racial and economic segregation of residential neighborhoods. Racial residential segregation remains a characteristic feature of life in the United States, with little change from 1960 to 2000 (Emerson, Yancey, and Chai, 2001; Logan, Stults, and Farley, 2004; Timberlake, 2002), and is often recognized as a distinct form of deprivation and inequality (Farley and Frey, 1994; Lee and Ousey, 2005; Logan et al., 1996; Ovadia, 2003; Timberlake, 2002). Because of the interrelated nature of neighborhood racial characteristics and socioeconomic context, Robert (1999) calls for exploration of the role of racial residential segregation in affecting the health of individuals. A majority of previous research assumes that racial segregation is unhealthy for ethnic minorities (Ovadia, 2003; Timberlake, 2002). Cities characterized by segregation have been found to also have high levels of other forms of racial inequality and discrimination (Ovadia, 2003), higher levels of economic segregation and perpetuation of poverty (Logan et al., 1996; Timberlake, 2002), increased levels of isolation from mainstream societal influences on social organization and social control (Lee and Ousey, 2005), higher levels of occupational segregation along with joblessness, welfare dependency and barriers to labor force participation (Lee and Ousey, 2005; Ovadia, 2003), unequal political representation, public service levels, tax burdens, schools, and exposure to crime (Lee and Ousey, 2005; Logan et al., 1996; Ovadia, 2003). In his study of ethnic residential stratification, Timberlake (2002, p. 261) concludes concisely, “Segregation is especially bad for minorities if they are also poor.”
In addition to the negative consequences of racial and economic segregation discussed earlier, which directly affect individual and community levels of stress and well–being, researchers have found negative effects of this concentrated disadvantage on individual– and community–level coping resources. In the impoverished and segregated minority neighborhood in particular, aspects of the impoverished existence may inhibit the formation of black consciousness, fostering fragmentation and mistrust in the community. In addition, the level of community destabilization found in neighborhoods with concentrated disadvantage breaks down feelings of racial group solidarity and community efficacy (Cohen and Dawson, 1993), which greatly influences a decrease in social capital. Although individuals may develop alternate strategies of social support that focus on kin networks, particularly in impoverished African American communities (Schieman, 2005), the density of obligations and expectations necessary to strengthen neighborhood social cohesion are lacking (Mitchell and LaGory, 2002). Residents in these communities with low levels or nonexistent social capital are also less likely to come to the aid of their neighbors, and have fewer people they can turn to for social support (Rankin and Quane, 2000). Within integrated communities, on the other hand, African Americans are less likely to face societal isolation, racial discrimination, or barriers to achievement, and have greater access to human, physical, cultural, and social capital (Lee and Ousey, 2005).
Although a majority of research on racial residential segregation has depicted negative consequences, few studies have found positive effects of segregation or no effects at all (Browning and Cagney, 2002; Ovadia, 2003; Timberlake, 2002). Ross, Mirowsky, and Pribesh (2001) found that the concentration of minority residents in a community, along with other indicators of concentrated disadvantage, correlated with mistrust, but that this correlation became nonsignificant when adjusting for the concentration of poor and mother–headed households in the community. Browning and Cagney (2002) found that ethnic heterogeneity in the community can impede rather than strengthen communication among neighbors, complicating efforts to implement shared goals in the community. Mitchell (2001) found that within impoverished segregated communities, minorities are significantly more likely to participate in neighborhood activities than are White residents in the same communities, and that this minority participation is higher in segregated communities than in more diverse communities. Similarly, Schieman (2005) discovered that African American women over the age of 65, residing in impoverished neighborhoods, receive and donate high levels of social support, helping to maximize network resources within the impoverished community. However, both of the previous studies found constraints on the utility of resource diffusion among poor minority residents—overcapitalization (Mitchell, 2001) and residential instability (Schieman, 2005).
Trust and Well–Being
Variations in the previously mentioned coping resources by racial dissimilarity of community members may be attributed to levels of trust in neighbors. Trust and trustworthiness, themselves, are seen as coping resources in the social capital literature. Trust in neighbors, an integral aspect of social capital (Schieman, 2005), was found to be disproportionately high in an economically and racially segregated neighborhood studied, compared to national levels of trust in neighbors reported by African Americans (Mitchell, 2001). This variation between the trust levels of African Americans in high–poverty neighborhoods and the national trust level suggests that racial homogeneity in a community leads to higher levels of trust and perhaps higher levels of participation. That is not to say that all high–minority, high–poverty areas will have such levels of trust. Pipkin, LaGory, and Blau (1983) suggested that the level of income and ethnic diversity in an area will be highly related to trust levels. Krysan and Farley (2002) have found that residential preferences of African Americans play an important role in maintaining neighborhood segregation. Preferences for residential racial homogeneity are related to in–group attraction and out–group avoidance. Both attraction and avoidance are influenced by the extent of trust the individual has in others.
Trust is the cornerstone of productive social capital. To build and reap the benefits of social capital, individuals must be involved, formally or informally, with other people. From this social capital perspective, the ability to form positive social relationships depends on trust, allowing pairs of individuals to establish cooperative relationships whenever doing so is mutually beneficial. Trusting individuals expect that they can depend on others, they believe in the integrity of other people, and they have faith and confidence in those around them (Ross, Mirowsky, and Pribesh, 2001). Trust and satisfaction are bound together, supporting mass participation and democratic governance, and are bound together within interpersonal relationships (Scheufele and Shah, 2000). Membership in social groups and the maintenance of social ties, coupled with trust, allow people access to resources and opportunities.
Dekker and Uslaner (2001) identified two types of trusters. A “particularized truster” is someone who has faith only in her or his own kind. This is the type of truster who would experience the in–group attraction and/or the out–group avoidance found to influence residential preferences of African Americans (Krysan and Farley, 2002). Particularized trusters are also likely to experience high levels of bonding social capital: the healthy networks among similar others that can strengthen collective efficacy and social cohesion (Mitchell and LaGory, 2002; Putnam, 2000). A “generalized truster,” on the other hand, places confidence in strangers, including dissimilar others (Dekker and Uslaner, 2001). The latter truster will experience the key benefits of trust and is willing to take risks in a social context based on the confidence that others will act in mutually supportive ways (Onyx and Bullen, 2001). This generalized trust in others leads to bridging social capital, which increases opportunities for diverse resource diffusion (Putnam, 2000). In addition to influencing resource diffusion and acquisition, both particularized and generalized trust lead to simple satisfaction and comfort within a community. Theoretically, the more diverse the social groups and ties bound by trust in a community, the more diverse are the resources and opportunities accessible to the individual, therefore, the more healthy the individual.
Concentrated Disadvantage, Trust, and Well–Being
Among the risks to well–being connected with inner–city residence are a high prevalence of contextual stressors and concentrated disadvantage (Andrulis, 1997; Fitzpatrick and LaGory, 2000; Ross, Mirowsky, and Pribesh, 2001; Ross, Reynolds, and Geis, 2000; Schulz et al., 2000). The distress process associated with neighborhood context is a substantial area of study within medical sociology and social epidemiology, and urban sociology also has a long history of stress–related research (Faris and Dunham, 1939; Srole et al., 1962). However, little work has focused on the linkages between concentrated disadvantage, social capital or trust alone, and well–being of the individual (Schieman, 2005). One of the central assertions of the social capital perspective is that the health of a community is determined in part by the level of civic engagement of its residents. This assertion suggests that the components of social capital, then, should certainly be viewed as useful individual resources; an individual's integration into their neighborhood is positively related to their mental and physical health (Fitzpatrick and LaGory, 2000; Putnam, 2000; Scheufele and Shah, 2000).
Much of the stress research in sociology utilizes a psychosocial resources model to examine the relationship between stressors, psychological and social resources, and well–being (Lin, Dean, and Ensel, 1986). This model posits that all life events are potentially stressful and, if unbuffered, will have detrimental effects on health. Individual psychological attributes, constitutional features, social factors, and other contextual variables can affect the impact of life events and chronic stressors on the occurrence of distress. Psychosocial resources were conceptualized by Ensel and Lin (1991) as reactive elements in the stress process. These resources can be drawn upon or mobilized in order to mediate or buffer the harmful consequences of stressors. Psychosocial resources, like stressors, are elements in the internal and external environments. They can either directly enhance well–being by deterring distress or mediate or counter the consequences of stressful conditions or situations (Ensel and Lin, 1991). These coping resources are frequently studied in sociology, with concentrations on psychological resources (Thoits, 1995). Psychological resources are personality characteristics such as mastery and self–esteem (Fitzpatrick and LaGory, 2000; Lin and Ensel, 1989). Social resources are elements within a person's social network that serve specific needs such as social support (Fitzpatrick and LaGory, 2000).
This study presents a psychosocial resources model examining the extent of concentrated disadvantage within inner–city neighborhoods as a chronic stressor of individuals residing in those neighborhoods. Previous research has shown the deleterious effects of concentrated disadvantage on individual well–being, highlighting the potential for long–lasting psychological and physical damage (Aneshensel, 1992; Brooks–Gunn and Aber, 1997; Ross and Mirowsky, 2001; Ross, Mirowsky, and Pribesh, 2001; Schulz et al., 2000). As an indicator of concentrated disadvantage (Lee and Ousey, 2005), economic and racial residential segregation may be a particularly powerful source of stress for minority residents who are already at a disadvantage in urban areas. Disadvantaged individuals tend to live in disadvantaged neighborhoods, and often lack resources that may be utilized to combat the effects of the disadvantage on well–being (Ross, Mirowsky, and Pribesh, 2001; Schieman, 2005).
As previously stated, psychosocial resources are conceptualized as reactive elements in the stress process that can be mobilized to mediate stressors’ harmful consequences (Ensel and Lin, 1991). Both psychological and social resources have been found to be inversely distributed by social status (Aneshensel, 1992; Thoits, 1995). Trust in others, the integral component of social capital, has been found to increase general happiness and satisfaction (Scheufele and Shah, 2000), to achieve beneficial community outcomes (Browning and Cagney, 2002), and to be the predominant value on which productive social capital rests (Wilson, 1997). Thus, trust is conceptualized here as an important psychosocial resource, influenced by both psychological and social elements of an individual's experiences and environment, which may serve as a mediating force in the stress process.
Diener (1984) reported that for decades scientists have ignored positive subjective well–being, focusing instead on human unhappiness. The majority of current research on mental health supports this assertion, using negative indicators such as depression and anxiety to examine well–being. Mental and emotional well–being consists of happy, hopeful, and energetic feelings (Ross, Mirowsky, and Goldsteen, 1990); consequently, this paper examines positive indicators of well–being in the forms of self–reported happiness and physical health, rather than negative indicators.
Hypotheses
Given the review of the literature, this research proposes to test the following hypotheses for a sample of African American residents living in various types of neighborhoods in the Birmingham, Alabama, Metropolitan Statistical Area:
The extent of concentrated disadvantage in a resident's neighborhood is inversely related to the individual's level of happiness.
The individual's level of trust is positively related to the individual's level of happiness.
The effect of concentrated disadvantage in a resident's neighborhood on the level of happiness of the individual is mediated by the individual's level of trust.
The extent of concentrated disadvantage of a resident's neighborhood is inversely related to the individual's self–reported health status.
The individual's level of trust is positively related to the individual's self–reported health status.
The effect of concentrated disadvantage in a resident's neighborhood on the self–reported health status of the individual is mediated by the individual's level of trust.
Data and Methods
To explore this study's research questions, data from two separate research projects are examined. The first study targeted a neighborhood in Birmingham, Alabama, which is composed of mostly minority, low–income households. The data were collected with a face–to–face household decision–maker survey conducted from October 2000 through February 2001. The survey used a random, multistage cluster sample of 222 households in this inner–city neighborhood. This survey employed questions derived from the Social Capital Community Benchmark Survey (Saguaro Seminar, 2000) as well as standard assessments of well–being and personal and place–related stressors. Portions of the questionnaire were designed to reflect the special needs and concerns of the neighborhood as determined by consultation, focus groups, and pretesting with community leaders. The refusal rate for participation in the study was only 4 percent.
The second set of data used in this project is the Social Capital Community Benchmark Survey (Saguaro Seminar, 2000), conducted to assess the civic behaviors of various communities. The survey was designed by the Saguaro Seminar: Civic Engagement in America, a project at the John F. Kennedy School of Government at Harvard University. The questionnaire averaged 26 minutes and was administered via telephone using random–digit dialing from July to November 2000. The Alabama portion of this survey included 500 cases from a variety of neighborhoods in the Birmingham metropolitan area. The response rate for this study was 32 percent. Although low, this response rate was above average for the 40 communities sampled nationwide, whose response rates ranged from 29 to 34 percent. The Alabama sample was demographically representative of the Birmingham metropolitan area. Both data sets contain geographic identifiers that are linked to 2000 U.S. Census tract–level data in order to establish measurable neighborhood indicators. The data include only respondents who identified themselves as African American or Black, resulting in a final sample of 310 African American respondents from various communities across the Birmingham, Alabama, Metropolitan Statistical Area.
Measurement
Stressor
Census tracts are used as a proxy for neighborhoods, with tract–level data attached to the survey data to indicate neighborhood–level variations. The Census Summary Tape file 3 from the 2000 Census of Population and Housing provides independent assessments of disadvantage in the contextual units. The percentages of households below the poverty line and mother–only households are common measures of neighborhood disadvantage (Ross, 2000; Ross, Mirowsky, and Pribesh, 2001). The percentage of minority residents or of White residents is also often used in neighborhood context measures (Alba, Logan, and Stults, 2000; Browning and Cagney, 2002; Fernandez and Kulik, 1981; Logan et al., 1996; Ovadia, 2003) to assess racial concentration and segregation. Concentrated Disadvantage, conceptualized here as the extent of economic and racial segregation within a neighborhood, and a potential chronic stressor, is measured with an index summing the percentage minority, the percentage of households with incomes below the federal poverty line, and the percentage of female–headed households with children within each respondent's census tract. The range of the index is 9.04–192.79, with a mean of 125. Higher scores on the concentrated disadvantage index indicate higher percentages of economic and racial concentration of a neighborhood, which is used to simulate economic and racial segregation of the neighborhood. After completing preliminary analyses, I also separate the stressor variable into two components: minority saturation, measured by the percentage minority within the census tract, and neighborhood poverty, indicated by the percentages of households below the poverty line and single–mother households within the census tract.
Resources
Two different measures of trust were available for this analysis. These two measures of trust have a Pearson Correlation of 0.344, significant at the 0.01 level. Both measures of trust are used as the psychosocial resources in this model. Particularized trust, defined by Dekker and Uslaner (2001) as trust in similar others, is assessed with the item “In general, do you feel you can trust your neighbors?” Response choices are “You can't be too careful” (0) and “I can trust my neighbors” (1). Sixty–four percent of the respondents reported that they can trust their neighbors. The particularized truster is the individual most likely to experience bonding social ties.
Generalized trust, defined by Dekker and Uslaner (2001) as trust in strangers and dissimilar others, is assessed with the item “In general, do you feel you can trust most people?” Response choices are “You can't be too careful” (0) and “I can trust most people” (1). Only 33 percent of the respondents reported that most people can be trusted. The generalized truster is more likely to experience the benefits of trust (Onyx and Bullen, 2001), as generalized trust in others leads to bridging social ties, which increase opportunity for diverse resource diffusion (Putnam, 2000).
Well–Being
Mental well–being is assessed with the item “In general, how happy would you say you are?” Response choices are “not happy at all” (1), “not very happy” (2), “happy” (3), and “very happy” (4). Physical well–being is assessed with the item “How would you describe your overall state of health these days?” Response choices are “poor” (1), “fair” (2), “good” (3), “very good” (4), and “excellent” (5).
Control Variables
Control variables included in the analysis are gender, age, level of income, level of education, employment status, and marital status—all characteristics found to affect health and well–being outcomes. Length of residence in the neighborhood is also included as a control variable. Little past research has taken into account length of residence in a neighborhood (Rankin and Quane, 2000). This measure is used here to control for exposure to the ecological setting of each neighborhood.
For gender male is coded 0, female is coded 1. Age is the age in years of respondents at the time of interview. Level of income is operationalized as total household income for 1999 and includes five categories: “$20,000 or less” (1), “$21,000–$29,000” (2), “$30,000–$49,000” (3), “$50,000–$74,000” (4), and “$75,000 or greater” (5). Level of education includes seven categories: “less than high school” (1), “high school diploma or GED” (2), “some college” (3), “associate's degree or technical degree” (4), “bachelor's degree” (5), “some graduate training” (6), and “graduate or professional degree” (7).
Employment status categories originally included employed, unemployed, retired, temporarily laid off, student, homemaker, and disabled. Less than 10 percent of respondents reported in many of the categories (student, homemaker, disabled, and laid off). While there was a moderate number of retirees (almost 18 percent), there were no significant differences in any relationships with study variables between retirees and the unemployed. After a thorough examination of potential variations between retired and unemployed respondents, these two categories were combined. Thus, employment status is coded 1 for working for pay and 0 for not working for pay.
Marital status is coded 1 for married or cohabitating and 0 for not married or cohabitating. Length of residence in the neighborhood contains two categories: residence in the neighborhood for 5 years or less (0) and residence in the neighborhood for more than 5 years (1).
Analytic Strategy
The psychosocial resources models of well–being are tested using progressive adjustment, multiple regression analysis to measure the relationships between concentrated disadvantage, trust, and mental and physical well–being. First, the associations between concentrated disadvantage and well–being are determined without the sociodemographic control variables, these background characteristics are then added to the model to adjust the effects of concentrated disadvantage in the neighborhood by individual–level factors. The presence of mediation is then ascertained by assessing whether the addition of the psychosocial resource of trust into the model reduces the value of the stressor coefficient.
Results
table 1 reports descriptive statistics for variables in the analysis. Respondents were predominantly female and middle–aged, with over half in the workforce at the time of the survey. Over one third of the respondents had a household income in 1999 of less than $20,000, and almost 20 percent had a household income of $50,000 or more. Almost 16 percent had not finished high school, 33 percent had a high school degree or GED, while 16 percent had some type of post–high school training or degree. Over one third of the respondents were married or cohabitating at the time of the survey. Sixty percent of the respondents have lived in their neighborhood for over 5 years.
Descriptive Data for Variables in the Analysis
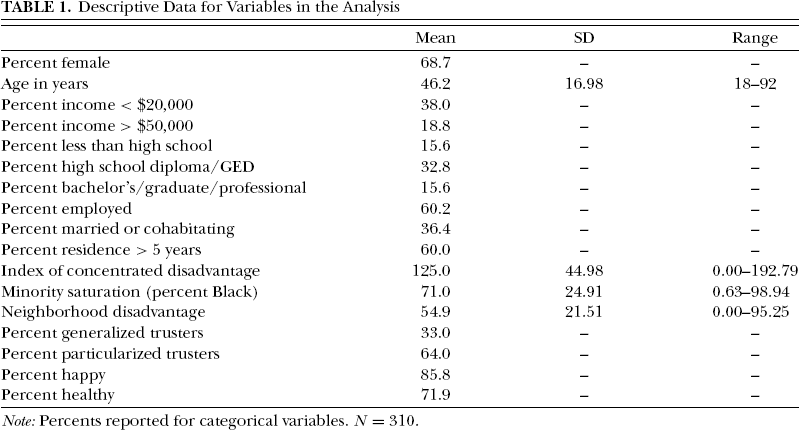
Note: Percents reported for categorical variables. N= 310.
The descriptive data of neighborhood disadvantage measurements are striking. The index of concentrated disadvantage, which is the summation of percent minority, percent households below the federal poverty line, and percent mother–only households within census tracts, ranges from 0 to approximately 193, with a mean of 125. The significant contributor to this skewed distribution is the percent minority, which ranges from 0.63 to 98.94 percent, with a mean of 71 percent. Mitchell (2001) found that minority saturation as a stressor became a significant predictor of well–being when the saturation exceeds 85 percent minority within a census tract. Almost one third of respondents in this study reside in tracts with over 85 percent minority. The measurement of neighborhood disadvantage includes percentages of households below the poverty line and mother–only households, with a range of 0–95.25, and a mean of 54.9.
The percentages of respondents reporting generalized and particularized trust are not surprising, with a much higher percentage reporting particularized trust (in neighbors), at 64 percent, than those reporting generalized trust (in most people), at 33 percent. With the high minority saturation within these neighborhoods, we can expect higher levels of in–group trust and lower levels of out–group trust. The high percentages of respondents reporting happiness and good health are surprising considering the relatively high concentrated disadvantage scores and the findings of previous research on neighborhood distress and well–being. Almost 86 percent of respondents reported being happy or very happy. Approximately 72 percent of respondents reported their health to be good, very good, or excellent.
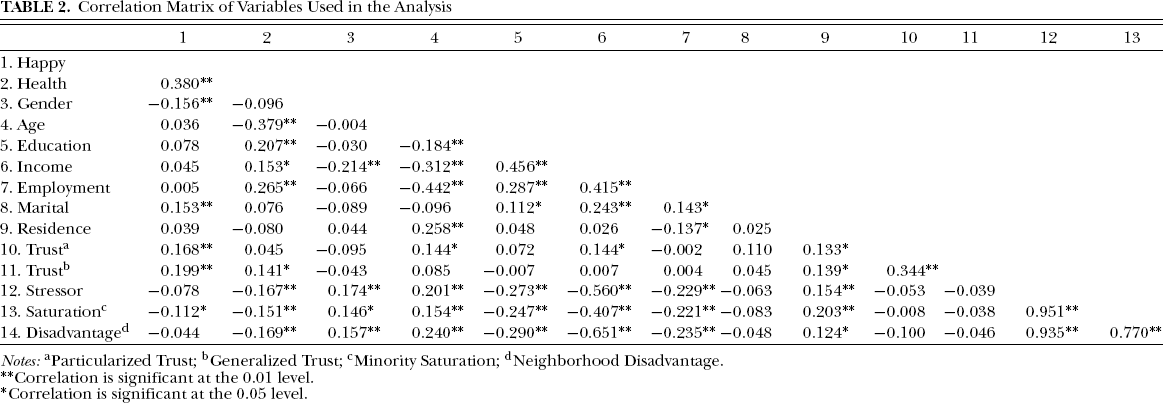
table 2 reports zero–order correlations between variables used in the analysis. These data show that women, older people, unemployed persons, and those with lower education and income are more likely to live in neighborhoods with higher levels of concentrated disadvantage. There is also a positive relationship between length of residence and concentrated disadvantage. A significant, negative relationship between health status and concentrated disadvantage supports Hypothesis 4: the extent of concentrated disadvantage of a resident's neighborhood is inversely related to the individual's self–reported health status. These results do not, however, support the first hypothesis: the extent of concentrated disadvantage of a resident's neighborhood is inversely related to the individual's level of happiness. Although there is a negative association between the stressor and happiness, this relationship is not significant.
Correlation Matrix of Variables Used in the Analysis
Notes:
Particularized Trust;
Generalized Trust;
Minority Saturation;
Neighborhood Disadvantage.
Correlation is significant at the 0.01 level.
Correlation is significant at the 0.05 level.
Turning to the minority saturation and neighborhood poverty measures, there are significant inverse associations between the percentage of Black residents within the neighborhood and levels of health and happiness. While the concentration of poverty and mother–only households within the neighborhood does not appear to be related to individual level of happiness, the concentration of minority residents does. Neighborhood disadvantage, measured as concentration of poverty and mother–only households, does, however, appear to have an inverse relationship with health status. These results further support Hypothesis 4, reinforcing the relationship between concentrated disadvantage and health status, and offer partial support for Hypothesis 1: the extent of concentrated disadvantage (although only through minority saturation) in a resident's neighborhood is inversely related to the individual's level of happiness.
The results in table 2 show no relationships between the stressor variables and either measure of trust. While the associations between the particularized and generalized trust variables, and the concentrated disadvantage stressor variable, are negative, neither is significant. Likewise, neither concentrated poverty nor minority saturation shows significant association with trust. Particularized trust (trust in neighbors) shows significant, positive associations with happiness, age, level of income, and length of residence. Generalized trust (trust in most people) shows significant, positive associations with both happiness and health, and length of residence. These results support Hypotheses 2 and 5: the individual's level of trust is positively related to the individual's levels of happiness and health, respectively. The differences in the relationships between well–being and the trust measures offer support of previous social capital literature. That trust in neighbors is positively associated with happiness may lend support to the idea that bonding social capital builds social cohesion and increases comfort level in a neighborhood. The associations between trust in most people and both happiness and health may lend support to the idea that bridging social capital increases resource diffusion, which can affect health outcomes of both individual and community.
Tables 3 and 4 present the results of the well–being outcomes regressed on stressors, sociodemographic controls, and generalized trust (trust in most people). I have tested the equations using three separate models. The original intent of this research was to examine the effects of concentrated disadvantage, conceptualized as the summation of percent minority, percent households below the federal poverty line, and percent mother–only households within each census tract. Because the results of the original analysis were questionable, as can be seen in Tables 3 and 4, I have added a regression model using minority saturation alone as a potential stressor, and another using neighborhood disadvantage, conceptualized as the percentages of households below the poverty line and mother–only households in each census tract, as a potential stressor. The rationale behind separating the components of the original concentrated disadvantage stressor is to examine any potential confounding effects of the combination of minority saturation and poverty measurements upon each other, which was considered a possible reason for the weak results of the original analysis. I have also removed particularized trust (trust in neighbors) from the psychosocial resource model, as it consistently had no predictive or moderating power over well–being outcomes or stressors. Recall that trust in neighbors did have a positive relationship with level of happiness in the bivariate correlations presented above; however, this particularized trust did not show any significant relationships with other variables throughout the remainder of the analyses.
Happiness Regressed on Stressor, Sociodemographic Controls, and Resource: Three Models
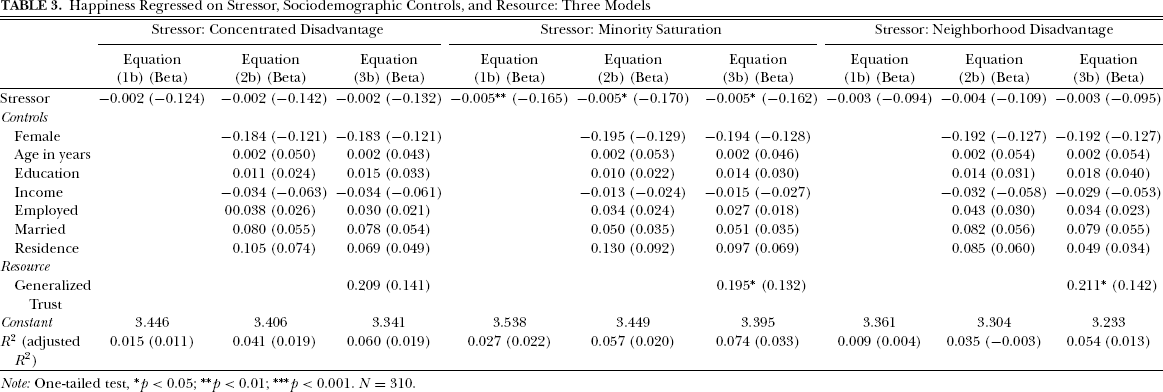
Note: One–tailed test,
p < 0.05;
p < 0.01;
***p < 0.001. N= 310.
Health Regressed on Stressor, Sociodemographic Controls, and Resource: Three Models
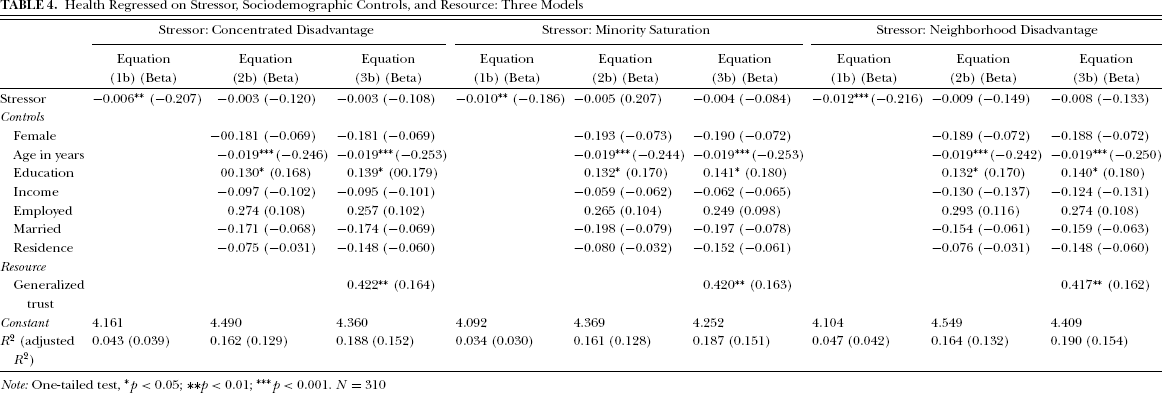
Note: One–tailed test
p < 0.05;
p < 0.01;
p < 0.001. N= 310
The regression models in table 3 examine the relationships in the psychosocial resources model with self–reported happiness as the endogenous variable. Three models are presented: the first uses concentrated disadvantage as the stressor variable; the second uses minority saturation as the stressor variable; and the third uses neighborhood disadvantage as the stressor variable. Equation (1) of each model regresses happiness on the stressor variable. Equation (2) of each model adds the control variables—gender, age, income, level of education, employment status, marital status, and length of residence in the community—to remove any individual–level influences from the relationship between the stressor and happiness. Equation (3) of each model adds generalized trust (trust in most people) to the model to test for influences on happiness as well as on the relationship between the stressor and happiness.
The first three equations in table 3 show the results of regressing happiness on concentrated disadvantage as a stressor, the sociodemographic controls, and generalized trust as a resource. Although the relationships do show the expected directionality, there are no significant relationships in this model. As mentioned previously, a concern with this initial analysis was that minority saturation may be confounding the results. Perhaps minorities living in neighborhoods with high numbers of other minorities will experience positive rather than negative benefits of this saturation, and these positive benefits will decrease the effects of concentrated poverty on well–being. Previous research has been mixed on this issue. The next set of equations show the results of regressing happiness on minority saturation, the sociodemographic controls, and the trust resource. Contrary to the expectation, minority saturation remains, through each equation, a weak but significant predictor of happiness. As minority saturation within the neighborhood increases, level of happiness decreases. Even with the inclusion of individual–level control variables, minority saturation does appear to be a stressor. The inclusion of generalized trust in the third equation does not affect the regression coefficient of minority saturation, offering no support for Hypothesis 3: the effect of concentrated disadvantage on happiness is mediated by individual level of trust. Generalized trust does show a significant positive relationship with happiness. The third set of equations regress happiness on neighborhood disadvantage, conceptualized as percentages of households below the federal poverty level and mother–only households, as the stressor, sociodemographic controls, and the trust resource. Like the first stressor, concentrated disadvantage, neighborhood disadvantage does not appear to have any predictive power of happiness. Generalized trust, however, does show a significant positive relationship with happiness.
The results of this analysis offer further support for Hypothesis 2; individual's level of trust is positively related to individual happiness. However, the lack of significant relationships between both concentrated disadvantage and neighborhood disadvantage and happiness leads to rejection of Hypotheses 1 and 3; concentrated disadvantage and happiness are inversely related, and trust mediates the effects of concentrated disadvantage on happiness. Minority saturation alone, however, does affect individual level of happiness.
The regression models in table 4 examine the relationships in the psychosocial resources model with self–reported physical health status as the endogenous variable. The three models, each using a different stressor, are presented in the same format as the models in table 3. An interesting similarity throughout these models, not seen in table 3, is the consistency of the stressor variables showing a significant inverse association with physical health prior to the addition of sociodemographic controls in the second equations of each model.
The first set of equations in table 4 regress health status on concentrated disadvantage as the stressor, sociodemographic controls, and generalized trust as a resource. Concentrated disadvantage has a weak but significant inverse association until the control variables are added to the model. Generalized trust has a fairly strong and significant relationship with health, supporting Hypothesis 5: level of trust is positively related to health status. The second set of equations uses minority saturation as the stressor variable and, again, it is a weak but significant predictor of physical health until the sociodemographic control variables are added in Equation (2). Generalized trust is significant here as well. In the third set of equations, neighborhood disadvantage is used as the stressor variable. This stressor has, as the others, a weak, but more significant, inverse relationship with health. Trust, again, is a significant predictor of health status.
Discussion and Conclusion
A psychosocial resource model of well–being was presented and analyzed to examine relationships between concentrated disadvantage of the neighborhood as a stressor, trust—an integral component of social capital, as a resource, and mental and physical well–being. Concentrated disadvantage was assessed using an index of neighborhood disadvantage that sums the percentages of minority residents, households below the poverty line, and single–mother households, using census tract as an approximation of neighborhood, across the Birmingham, Alabama, Metropolitan Statistical Area. This index was conceptualized as the extent of racial and economic segregation of a neighborhood. Two additional models were examined, breaking apart the concentrated disadvantage stressor into two separate potential stressors: minority saturation and neighborhood disadvantage. The psychosocial resource of trust was measured with a single–item indicator of generalized trust in “most people.” Mental well–being was measured with a single–item indicator of level of happiness, sometimes used interchangeably to measure quality of life, emotional well–being, or mental well–being. Physical health was measured using a single–item indicator of overall physical health status. Unlike a majority of studies focusing on urban context and well–being, this study focused on African American residents of various neighborhoods, to examine the psychosocial resource model based on variation of neighborhood stressors rather than variation of race.
It was expected that residents of neighborhoods with higher scores on the index of concentrated disadvantage would experience lower levels of both happiness and physical health than residents of neighborhoods with lower scores on the index of concentrated disadvantage. The negative consequences of concentrated disadvantage resulting from racial and economic segregation on well–being have been repeatedly reported in the relevant literature. It was also expected that residents reporting higher levels of trust in those around them would experience higher levels of both happiness and physical health than residents reporting lower levels of trust in those around them. According to the social capital perspective, trust breeds reciprocity; exchange of resources; social, psychological, and physical support; empowerment; and collective efficacy and action, all of which have been found to increase various measures of quality of life including social, mental, and physical well–being. Trust was also expected to act as a mediator between the negative consequences of concentrated disadvantage and well–being outcomes.
The results of the analyses presented above only partially support these expectations. The extent of concentrated disadvantage resulting from racial and economic segregation does appear to be inversely related to both well–being outcome measures presented in the analyses. However, while the association between disadvantage and physical health is statistically significant, the association between disadvantage and level of happiness is not. In addition, the relationship between concentrated disadvantage and physical health becomes nonsignificant when sociodemographic variables are added to the analyses. Likewise, while the association between concentrated disadvantage and trust is negative, it is not statistically significant.
Examination of the two additional models shows surprising results. It was assumed that perhaps a high saturation of minority residents within a neighborhood would offer benefits to individuals in the form of stronger social cohesion, stronger support networks, increased bonding relationships, and the like. These resources have been repeatedly found to have positive influences on well–being. Previous research on consequences of racial residential segregation has had mixed results. The results presented here support previous findings that racial residential segregation is, in fact, unhealthy for residents. This racial segregation appears to be even more unhealthy than economic residential segregation for the minority resident. Neighborhood poverty, a contextual measure of disadvantage, loses its significant association with well–being when individual–level poverty factors are considered. Based on these results, further research on the effects of racial residential segregation is certainly called for.
The examination of trust as a psychosocial resource in the distress process showed more significant results than those found in the examination of the original stressor variable, concentrated disadvantage. The expectations that higher levels of generalized trust (trust in most people) are positively associated with mental and physical well–being were strongly supported by the analyses. As levels of this type of trust increase, so do levels of happiness and physical health. Conceptualized as an integral component of social capital, responsible for allowing the accumulation, proper functioning, and maintenance of social capital, generalized trust appears to be a very important resource for the individual regardless of the level of neighborhood disadvantage one experiences. That particularized trust (trust in neighbors) had no effect on well–being is an interesting finding as well. This type of trust is considered to be one of the important bonding agents within a community. Individuals who feel they can trust their neighbors and communities characterized by trusting relationships among neighbors should experience high levels of social cohesion and strong support networks. According to the social capital perspective, the benefits of these reciprocally bonding relationships include increased mental and physical health status, self–efficacy, and commitment to community. The results of these analyses raise questions about the utility of this resource in the impoverished minority community. Trust in neighbors should certainly be useful within any type of neighborhood. However, in the neighborhood with high concentrations of disadvantage, the supposed resources offered by bonding relationships do not appear to affect the consequences of that disadvantage.
The mediation models presented in the analyses showed fairly weak relationships. While generalized trust (trust in most people) did have significant positive effects on both well–being measures, the disadvantage itself was not a significant predictor of well–being outcomes in either model. The correlation coefficients presented earlier show a significant relationship between concentrated disadvantage and physical health, suggesting that the physical health of residents in high–stress neighborhoods is rated lower than the physical health of residents of lower–stress neighborhoods, but the extent of economic and racial segregation itself does not appear to cause significant variations in self–ratings of physical health.
A potential limitation of the mental well–being measurement used in this analysis that deserves mention is the relative difficulty often encountered when using positive subjective indicators of well–being, like happiness. First, it is likely to be easier for a respondent to recall negative indicators of well–being, like crying and sleeplessness, which may have occurred recently in their lives, than it is for them to recall specific instances of overall feelings of happiness. Negative indicators are easier to quantify than are many positive indicators. Second, respondents have a tendency to give the socially desirable response, particularly to questions regarding “general” feelings or attitudes, and this is most apparent in underrepresented or minority group members (Ross and Mirowsky, 1984). Thus, it is entirely possible that the measurement of happiness used in this analysis does not prove to be a valid measurement of mental well–being for this particular sample. A third possibility contrasts with the validity issue. Schuessler and Fisher (1985) contend that positive subjective indicators of well–being can be quantitatively measured with substantial validity, but impoverished populations may not show as much variation in these indicators as one would expect; lower expectations in life, influenced by personal experiences of marginality, may lead to satisfaction, or happiness, with less. More research in this area would be a very useful addition to well–being studies.
The research presented here assesses the strength of the impact of racial and economic segregation on individual well–being, with racial segregation and the psychosocial resource of generalized trust standing out as significant influences on both mental and physical well–being. The implications of these findings are significant. High degrees of minority saturation within a neighborhood are shown to be unhealthy for the minority resident. The influence of in–group and out–group trust on minority residential preference surely plays an important role here. The results here show that out–group trust has positive influence on both mental and physical well–being. Trust is the cornerstone of social capital. Generalized trust increases resource diffusion and increases expansion and maintenance of diverse social networks (Putnam, 2000). This research shows that this form of trust is also positively related to quality of life. In the context of marginalized neighborhoods, this finding can be used as an important tool in community development strategies. In–group trust is certainly not damaging here, and out–group trust has positive consequences for the individual. Development, whether coming from within the community or from an outside agent, should begin with strategies of assessing trusting relationships with and among the residents of the community. In addition, assumptions of the utility of individual social capital components should be treated with care; this research adds to a growing body of literature (Mitchell, 2001; Mitchell and LaGory, 2002; Schieman, 2005) finding that not all components of social capital are particularly healthy for the individual and some are, in fact, unhealthy.
Footnotes
Acknowledgment
This research was supported by grants from the Community Foundation of Greater Birmingham and Region 2020, and orchestrated by Mark LaGory at University of Alabama, Birmingham—to whom respect and thanks are due. The author would like to thank Anthony Orum and anonymous reviewers for their helpful suggestions.