
Abstract

Stroke is a heterogeneous disease with a plethora of differing stroke mechanisms. Small vessel, large artery atherosclerosis and cardio-embolic stroke are the most common subtypes encountered in clinical practice. Different stroke mechanisms may require different treatment. Anticoagulation for atrial fibrillation is a good example. Many recent research and clinical trials successfully targeted individual stroke subtypes rather than indiscriminately grouping all strokes together. For large artery atherosclerosis, carotid stenosis is the most common vascular lesion found in Caucasians in America and Europe and is extensively studied in terms of epidemiology, pathophysiology and treatment. Unfortunately, relatively little is known about intracranial atherosclerosis until recently; now, modern neuroimaging methods permit noninvasive screening of susceptible patients. Intracranial atherosclerosis affects the middle cerebral artery, intracranial portion of the internal carotid artery, vertebrobasilar artery, posterior, and anterior cerebral arteries. Examples of intracranial stenosis are shown in Figs 1 and 2. Transcranial Doppler ultrasound, CT angiography and MR angiography are now routinely available in clinical practice (1–4). Although digital subtraction angiography remains the gold standard of diagnosis of intracranial atherosclerosis, these noninvasive tests have been validated against clinical outcomes and events (5–7).
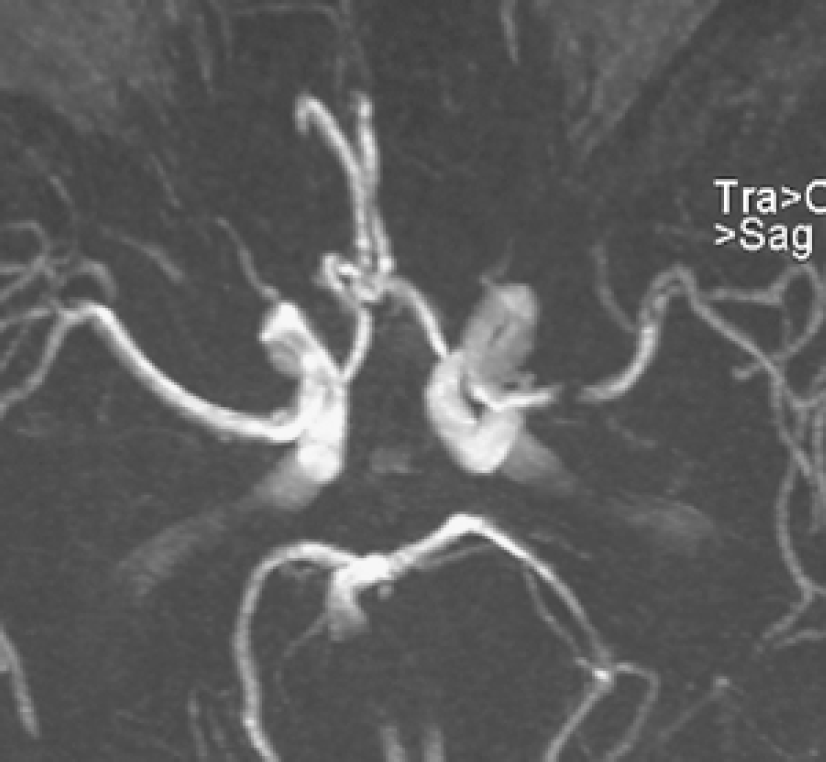
Right middle cerebral artery stenosis on a magnetic resonance angiography.
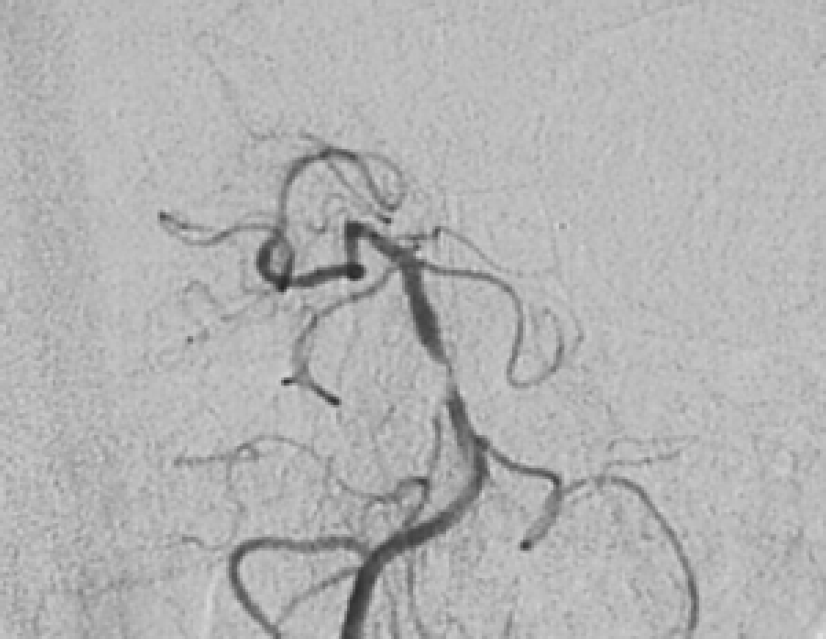
Severe basilar artery stenosis on a digital subtraction angiography.
For decades, it is well described that patients of Asian, African, and Hispanic ancestry were at higher risk of intracranial atherosclerosis (8). More recent studies on consecutive patients confirm this finding and pinpoint the frequency of intracranial atherosclerosis. In Chinese populations, intracranial atherosclerosis accounts for about 33–50% of stroke and > 50% of TIA (6, 9, 10). In Thailand, intracranial atherosclerosis was found in 47% of stroke patients (11). In Koreans, 56·3% of stroke patients had intracranial atherosclerosis although the authors used 30% stenosis as cutoff (12). In Singapore, significant intracranial stenosis was found in 47·9% of stroke patients (13). In Japan, the frequency of intracranial atherosclerosis remains high despite increasing frequency of extracranial carotid stenosis (14). In North America, extracranial carotid stenosis remains the most common vascular lesion in Caucasian stroke patients. However, when compared with Caucasians, the relative rate of intracranial atherosclerotic stroke was 5·00 for Hispanics and 5·85 for blacks (15).
Based on the widespread observation worldwide that intracranial atherosclerosis is the most common vascular lesions in Asians, Hispanics and Africans, and Caucasians remain the only ethic group with a low frequency of intracranial atherosclerosis. As the majority of the world's populations are Asians, Africans or Hispanic, it is reasonable to conclude that intracranial atherosclerosis is the most common vascular lesion in stroke patients worldwide. Not only the number of patients with intracranial atherosclerosis is staggering but also patients with intracranial disease are at a high risk of recurrence of up to 25–30% in 2 years after stroke (5, 7, 16), further magnifying the burden of intracranial disease. Unfortunately, there has been little progress in finding a specific treatment for this most common vascular cause of stroke. Routine use of warfarin is not better than aspirin alone but dual antiplatelet therapy appears promising (17,18). Because reduced flow may be an important factor in the pathogenesis (16, 19, 20), revascularization is another strategy that should be studied further (21). International randomized clinical trials are urgently needed right now to combat this frightful disease with pitiable prognosis.