
Abstract
The looming epidemic of stroke and other chronic non-communicable diseases associated with lifestyle and demographic transitions occurring all over the world is increasingly being acknowledged. However, the significance of these trends in the relatively young populations of the countries comprising Sub-Saharan Africa (SSA) is less certain and considerably overshadowed by attention given to the impact of human immunodeficiency virus and other infectious diseases. We undertook a literature review of the burden of stroke in SSA and provide recommendations for future research. Despite the paucity of high quality studies, the mostly hospital-based data and limited community surveys indicate there to be high and increasing rates of stroke affecting people at much younger ages in SSA than in developed countries. In general, awareness, diagnosis and management of stroke are poor, and the associated case fatality and residual disability are high. As elsewhere, elevated blood pressure is the major determinant of stroke but there are also high rates of strokes related to the complications of rheumatic heart disease and other infections. Given high attributable risks exposures in association with rapid ageing and urbanisation in SSA, the future is not bright. Population-based incidence studies are urgently needed to map the profile and outcome of stroke. Such data would provide the necessary evidence base to improve prevention and treatments for stroke alongside current efforts to bring infectious diseases under control in SSA.
Introduction
Strong evidence supports an emerging epidemic of chronic non-communicable diseases, lead by cardiovascular disease (CVD), in developing countries as a result of urbanization and demographic re-structuring over the next few decades (1). However, the situation is often considered different in Sub-Saharan Africa (SSA) where infectious diseases such as human immunodeficiency virus/acquired immune-deficiency syndrome (HIV/AIDS) and malaria are prominent, and expected to remain so for the foreseeable future (2). As a consequence, there is an apparent reluctance on the part of health funding agencies and policy makers to divert attention and (scarce) resources away from these major health problems into other areas of need (3, 4). Yet, as in other regions of the world, CVD is anticipated to soon eclipse infectious diseases as the leading cause of death and disability in SSA (5). In the absence of reliable data, though, it is difficult to assess the size of the potential burden of CVD and develop appropriate strategies to avoid another ‘disaster waiting to happen’ (6,–8).
The pivotal World Health Organisation (WHO) global burden of disease study was only able to provide broad and conflicting estimates of disease burden in SSA due to the limited data available (9). Even in the absence of reliable data (10, 11), though, CVD was predicted to overtake infectious diseases as leading causes of premature loss of healthy life expectancy in SSA (12, 13). As noted elsewhere, to ignore CVD in SSA will inevitably lead to an increase in suffering, poor coordination and inefficient use of health services, and place populations at the mercy of treatments and prevention strategies with primarily local and/or global commercial interests (3).
The experience that is being gained in other populations, and especially in Asia, informs us that stroke is the dominant manifestation of CVD that results to a large extent from population-wide elevations in blood pressure levels during the early and middle stages of epidemiological transition (1). Stroke, therefore, is an appropriate model to assess the burden of CVD in SSA. We undertook a review of the published literature to summarise current knowledge of the epidemiology of stroke in SSA. We aimed to appraise gaps in the data and suggest some approaches using surveillance methodology to improve the situation and better meet the challenge of stroke in this part of the world.
Source of data
A search of MEDLINE and reference lists of the literature on stroke in SSA was conducted in June 2006, initially using the MeSH Terms ‘cerebrovascular accident’ and ‘Africa South of the Sahara’, which provided 74 entries. This was considered insufficient as the second term was only introduced into the MeSH database in 1994. The search was subsequently extended using the key words ‘stroke’ and ‘Africa’, which yielded 303 entries extending from 1971 to 2006. We limited the review to studies published after 1976, for a time period we considered appropriate to reflect the ‘current situation’ of stroke in SSA. Known researchers in the field of stroke in SSA were also contacted and requested to provide information on stroke for their country or sub-region. We eliminated duplicate publications, studies from countries in Northern Africa, studies done on African migrants, case reports, and studies without stroke as main focus, to produce a final database of 75 studies from over 20 countries in SSA. As summarised in Table 1, the majority of publications were from retrospective hospital-based studies in major urban cities aimed at addressing particular aspects of stroke including incidence, prevalence, types, risk factors, management and outcomes. There were a few community-based studies in either rural or urban settings, which incorporated aspects of prevalence, incidence, risk factors, and disability outcomes.
Key published literature on stroke in Sub-Saharan Africa
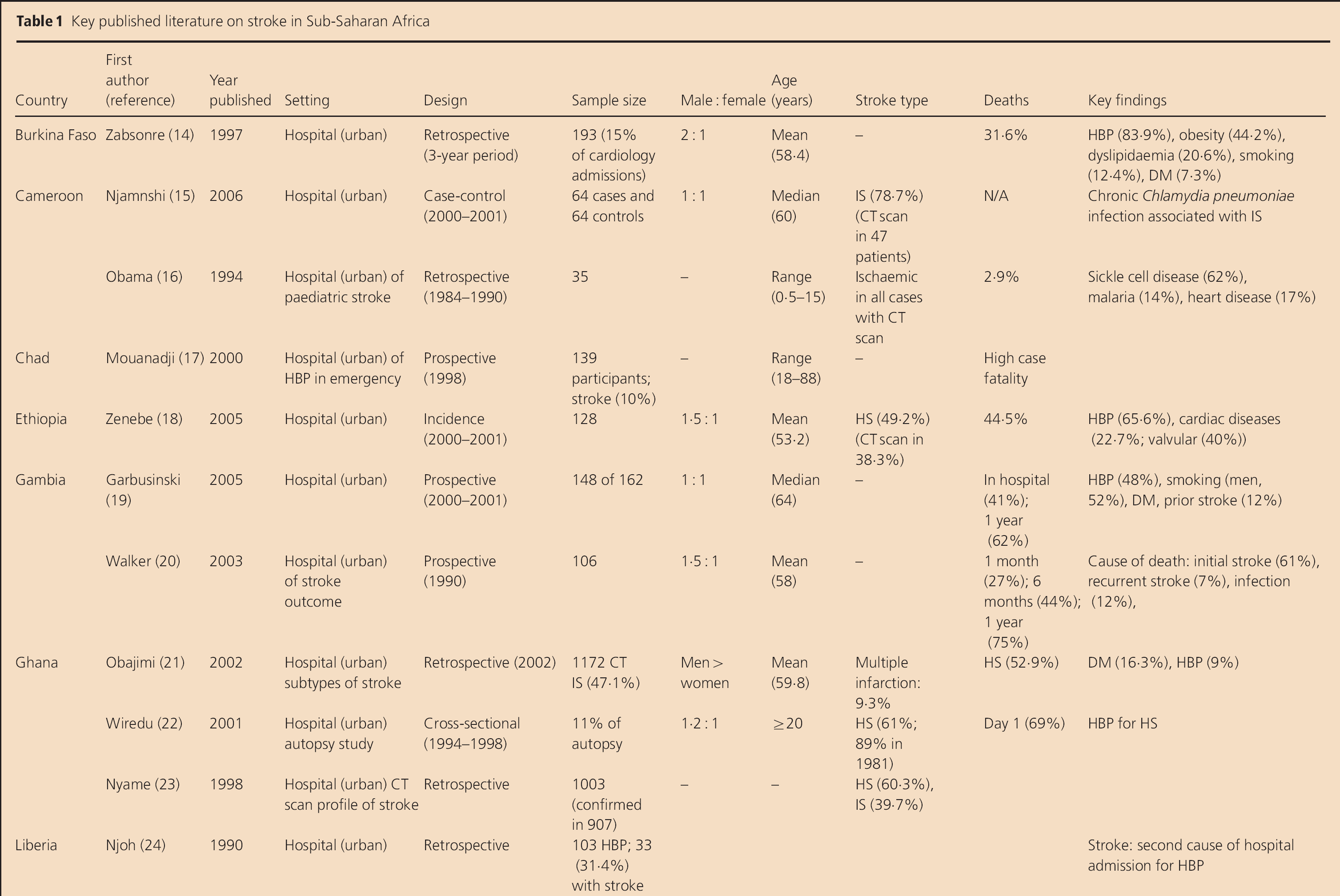
HS, haemorrhagic stroke; IS, ischaemic stroke; CVD, cerebrovascular disease; HBP, high blood pressure; HIV+, human immunodeficiency virus positive; CT, computerised tomography, DM, diabetes mellitus.
It is clear that there is a dearth of high-quality published studies that quantify adequately the burden of stroke in SSA. The use of clinic-based studies has serious limitations, particularly with regard to the generalization of the data, so only a broad indication of stroke related issues can be provided. Despite these reservations, we provide an appraisal of the epidemiological data in the following sections and make recommendations regarding future approaches to measurement, not withstanding the challenges to funding such efforts.
Rates of stroke
Even some 20 years ago, chronic diseases due to unhealthy lifestyles were noted to be responsible for 24·5% of all deaths and 28·5% of deaths in people aged between 35 and 64 years in South Africa (53). The major causes of death contributing to these figures were cerebrovascular diseases (7·2% of all deaths and 7·9% of deaths in those aged 35–64 years) and ischaemic heart disease (8·7% of all deaths and 9·6% of deaths in those aged 35–64 years). However, mortality and morbidity data are scarce and unreliable in other countries in SSA as births and deaths are not always recorded early after an event, if at all, and access to care and systems for coding such episodes are unavailable for most of the population.
As summarised in Table 1, several door-to-door household community surveys have been undertaken to estimate the burden of stroke and other diseases at single points in time and place in SSA. These studies broadly indicate there to be an increasing problem of stroke in SSA. In a community study of neurological disorders undertaken in Nigeria 20 years ago, Osuntokun et al. (32) reported a crude prevalence of stroke of 58 per 100 000 population. Similar figures (68 per 100 000) for instance were reported by Matenga (51) in Zimbabwe just a few years later. More recently, community surveys undertaken in South Africa (40), Togo (50) and Tanzania (49, 54) suggest the prevalence of stroke to be between 200 and 300 per 100 000. Although these figures are much lower than has been reported in economically rich countries, they suggest a potential 400% increase in the burden of stroke over at least the last two decades (40). More worrisome is the high prevalence of people living with stroke-related disability (200 per 100 000 population).
Of course, prevalence studies are likely to underestimate the burden of stroke as no account can be made of the potentially high early case fatality as well as there being problems with the diagnosis of stroke at a long time after the initial event. Population-based surveillance, on the other hand, is more reliable (and necessary) but is complex, costly and demanding. Consequently, there has not been any population-based stroke incidence study undertaken in SSA to date. However, one hospital-based stroke registry undertaken in Ibadan, Nigeria suggests an annual incidence of stroke of 26 per 100 000 population (28).
Types of stroke
Cost constraints and limited availability of computerised tomography (CT) imaging considerably restrict information on the profile of different pathological types of stroke in SSA. In many hospitals, CT scan is only performed in about half of all patients presenting with stroke, and usually only among those who can afford it. In those studies that have been able to achieve relatively high rates of CT, there is variation in the proportion of ischaemic compared with haemorrhagic stroke types. For example, the MEDUNSA stroke register showed that cerebral infarction accounted for 71% cases of stroke in South African Blacks (55), while intracerebral haemorrhage accounted for 60% of strokes in a series of over 900 CT-confirmed cases of stroke in Ghana (23). Similarly high proportions of haemorrhagic stroke were reported in a study in Tanzania (47). Even more inconsistent are the frequencies of different subtypes of ischaemic stroke across studies, with ‘small vessel’ lacunar infarction reported in up to 20% of all strokes (36, 56).
It is anticipated that the ongoing phase of the AMMP stroke incidence study in Tanzania (47) with high use of CT will provide more reliable estimates of the proportional frequencies of stroke types within a community setting. An age differential effect has been shown in the distributions of stroke types in SSA, with consistency across studies showing that haemorrhagic strokes occur at younger ages than ischaemic stroke. In fact, a 10-year difference in the peak age of occurrence in these stroke types has been shown in Ghana (22), where 50–59 years was the peak age of onset of fatal haemorrhagic stroke compared with 60–69 years for cerebral infarction. These finding was consistent with an earlier report of 60–70 years as the average age of onset of undifferentiated cerebrovascular disease in South Africa (57).
Sex differences
In general, the studies suggest that there are equal proportions of males and females affected by stroke in SSA, which may reflect an equal burden of CVD risk factors between the sexes. However, as it is difficult to relate case numbers to a base population at risk or assess the impact of selection bias favouring males who for cultural and/or financial reasons are more likely to be admitted to hospital. Moreover, the impact of sex on the age of occurrence of stroke varies across studies. In Ghana, for example, stroke deaths in males exceeds females in all age groups up to 60–69 years, but at older ages mortality is greater for females (22). In addition, there is an overall trend towards a poorer outcome from stroke in females compared to males (14).
Determinants of stroke
The key risk factor determinants of CVD recognized elsewhere are similarly responsible for stroke in SSA. However, the impact of individual risk exposures is likely to display temporal variation in different populations as the result of epidemiological and demographic transition.
Age
The study of any age-related phenomenon in SSA is seriously compromised by the considerably reduced average life expectancy as the result of the HIV/AIDS epidemic in this part of the world over recent decades. This illness has reduced average life expectancy to just 33 years in some African countries. Even so, most cases of stroke are reported to occur at relatively young ages (mean age <60 years in most studies) in SSA (20, 52), some 10–15 years younger than in developed countries (4). The age of occurrence is even younger for haemorrhagic compared with ischaemic stroke. These data indicate a high burden of premature stroke in SSA, consistent with previous reports of the early onset of complications of hypertension and CVD in developing countries.
Classical and other risk factors
Most of the classical risk factors described elsewhere are reported at different levels in SSA patients with stroke. High blood pressure is the risk factor most often reported in patients with stroke in SSA, with a frequency of over 90% at the time of presentation of stroke in several studies (52). In most cases, a history of high blood pressure is not known and therefore not treated (31, 52). Stroke is the second leading cause of hospital admission in patients with known high blood pressure in SSA (24). Other risk factors include diabetes (36), which is reported in up to 37% of patients, coagulopathies such as Protein S deficiency (42, 58), and cardiac disease, mainly valvular heart disease associated with atrial fibrillation, causing embolic stroke (18, 15, 52, 55, 59). Chronic infection with streptococcal pneumoniae has also been reported to be associated with ischaemic stroke in Cameroon (15). Dyslipidaemia has been reported in South Africa in general and in Burkina Faso, but at lower frequency in Blacks (14, 60). Other risk factors include neurosyphilis (52), smoking (14), and heavy alcohol consumption. Limited studies also suggest the contribution of cervical spine hyperflexion, stenosing carotid arteritis, cocaine and chorionic cancer (61). Reports of other risk factors/markers are limited to anecdotal case reports. However, the common denominators of most modifiable risk factors described in SSA series are under-diagnosed and poorly controlled (18).
Atherosclerosis
Atherosclerosis is an age-related degenerative process manifest symptomatically by coronary heart disease, cerebrovascular disease and peripheral vascular diseases as terminal events. Studies that have included various technologies report an increasing association of atherosclerosis with ischaemic stroke in SSA (22, 44). More importantly, atherosclerosis, as described elsewhere, tends to be generalized process especially in patients with multiple risk factors (59, 62, 63). Although not of the same magnitude as reported in other, predominantly ‘white’, ethnic groups, such findings herald the imminent surge of additional complications of atherosclerosis such as myocardial infarction in SSA (62).
Impact of HIV/AIDS
Studies are consistent in reporting that HIV/AIDS is not a major direct cause of stroke in SSA (40). Patients with HIV/AIDS and stroke share similar vascular risk factors to other patients with stroke. However, as such patients have elevated systematic inflammation, as noted by an increase in markers such as erythrocyte sedimentation rate (ESR) (39), HIV/AIDS may exacerbate the development of atherosclerosis. There are often challenges to the diagnosis of stroke and neuro-infectious complications of HIV/AIDS (64), but the presence of fever is a useful differential (25).
Stroke and sickle cell disease
Sickle cell disease occurs with high frequency in many African countries. It has been reported to be a major contributor to stroke in children, accounting for up to 57% of cases in Nigeria (65). The frequency of stroke among such patients in Cameroon is 6·7%, with an annual recurrence of 25% (66). In Congo, 3·2% of patients with sickle cell disease admitted experience stroke, and males are more often affected than females (67).
Socioeconomic factors
Poor socioeconomic status is the hallmark of stroke in SSA. Up to 72% of patients with stroke have low-income backgrounds, such as labouring jobs in 22% of cases in Burkina Faso (14). In a study of over 1000 consecutive cases of stroke in Congo, low socioeconomic class was also a strong predictor of poor outcome (34). Despite being disadvantaged, there are some reports to suggest that patients with known risk factors were reasonably compliant with treatments before the onset of stroke, despite having a poor understanding of risk factors and stroke symptoms (46). Community surveys also suggest that people with stroke-like symptoms maintain their physical, mental and social well-being reasonably well, and deal with this affliction and misfortune by visiting healers, prophets and churches more often than doctors (68).
Management of stroke
It is not uncommon for patients with stroke to present late, often more than a month after onset, to the hospital (31), and many people never present at all. In general, the in-hospital and post-acute care for stroke appears quite poor in SSA (19, 41). The majority of patients do not have access to confirmatory investigations such CT or magnetic resonance imaging (MRI), which are only available in major cities. Thus, the potential for misdiagnosis is high, and patients with surgically correctable conditions such as subdural haematoma and malignancy masquerading as stroke, are being denied treatment (30). There are few rehabilitation services available in SSA and there is low adherence to secondary prevention (69, 70). Some factors that have been associated with good recovery from stroke include younger age (<55 years), haemorrhagic forms of stroke, and access to early rehabilitation (35), but these data are complicated by the inclusion of ‘healthier’ patients who had the opportunity to receive in-hospital care. Cultural behaviour in SSA has meant that patients now combine traditional and modern medicine, although many refer preferentially to traditional faith healers. In the SASPI project, for example, up to 91% of stroke survivors had sought help, which involved allopathic health care for most and from traditional healers in many (41).
Burden on health resources
Stroke is the major neurological cause of admission to hospital in Nigeria (29), and the third most common cause of admissions to neurological services in Senegal (37), consuming up to 39% of healthcare resources and staying on average 3 weeks (31). The cost of care for stroke has been estimated at US$157 per episode which is high in fee-for-service countries where most of the population live below the poverty line. Stroke accounts for about 1·8% of all consultations and 1·9% of deaths in emergency services in Nigeria (28). Stroke is the second leading cause of admission to hospital among people with high blood pressure (34·8%) or heart failure (36·4%). Stroke accounts for about 10% of all presentations to emergency services among patients with high blood pressure in Djamena (17), and approximately 5% of all admissions and 10% of bed occupancy in adult medical wards in South Africa (20). Stroke also accounts for up to 17% of deaths in hospital (28). In specialized neurological service in Senegal, stroke accounted for 45% of all admissions and was associated with a high case fatality (38). The burden of stroke on healthcare resources has remained at best stable in African countries over the past few years. In a 10-year retrospective study in Nigeria, stroke accounted for 2·4% of emergency admission and contributed 1·8% of death in this setting (28).
Case fatality
Most hospital series report a high risk of death from stroke in SSA (49, 51), with more than 30% of patients dying within the first month of onset (51). At 6 months after onset, less the 60% of patients are still alive, and by 1 year the number is below 50%. Less than one quarter of all patients survive for longer than 4 years after the onset of stroke in SSA. The causes of death are the initial stroke (in 60%), recurrent stroke (7%), infection (12%) and others factors attributed to inappropriate care in hospital (20). Advanced age is a key determinant of survival after stroke; older people are at much greater risk of death (20, 32, 40). Other predictors of poor outcome include low social class, migration, higher baseline heart rate, systolic blood pressure levels and fibrinogen (34). Recurrent stroke has been reported at 11% by 1 year after onset and is associated with death in 80% of the time (28).
Disability
There is poor access of patients to rehabilitation services and little information available on the functional recovery of patients after stroke in SSA. While a report by Hale (71) suggests that many patients make a good recovery of their gait within the first few months after hospital discharge, it is likely that this is far too optimistic given the stringent selection criteria used, which was acknowledged in the report, thus limiting the generalisability of the findings. The age-standardised prevalence of people with stroke-related residual disability living in Tanzania is about half that reported in studies from developed countries (48).
Approaches to studying the epidemiology of stroke
The rational planning, provision and evaluation of prevention and management strategies all require reliable information on the rate of disease, the number of patients who survive, the extent of continuing disability, the amount of health care and resources required, and whether any of these outcomes are changing over time. Clearly, there are special challenges to obtaining such key epidemiological data on stroke in SSA. Risk factor associations require an ability to classify strokes into specific subtypes on the basis of an accurate clinical diagnosis and supporting information on CT and other diagnostic technology. In SSA, there are major access and cost barriers to care, with a sizeable proportion of patients with stroke who are never admitted to hospital and/or are in contact with the healthcare system. However, the ascertainment of cases of stroke on a community-wide basis is costly and demanding, particularly with regard to the diagnosis of stroke in situations where people have mild (or transient) symptoms, and where pathological confirmation is not readily available due to high early case fatality or ‘out-of-hospital’ death. Another factor is that an estimation of rates requires the ability to relate cases to a defined ‘at-risk’ denominator which is difficult to obtain in situations where there is no formal census of the population. As well as other methodological issues related to the assessment of the outcome including ensuring uniformity in the timing of follow-up assessments and the use of measurement instruments whose validity and reliability have been established, there are the obvious issues of safety for staff who undertake field work within many countries of SSA.
With all of these issues in mind, we consider there to be three key types of epidemiological studies that are both necessary and potentially achievable in SSA.
A population-based stroke incidence study in an urban setting
Such a study would have the advantage of allowing access for many patients to imaging and specialist physicians for diagnosis. Urban settings would also allow the inclusion of patients across the gradient of socioeconomic circumstances that are near representative of most populations in SSA. It would be important to ensure that the study population is of an appropriate ‘manageable’ size that produces adequate power to allow precision around the estimates generated. It should also be relatively well defined, with low levels of inward or outward migration. As many patients with possible stroke prefer to consult traditional healers rather than accessing health facilities in SSA, special effort would be required to ensure that these people as well those who died rapidly at home or in the community where captured by such a study. Although this study could provide the most reliable estimates of the burden of stroke, it would not allow these data to be directly compared with other major diseases unless similarly captured (e.g. acute coronary syndromes) into the surveillance protocol. Yet, the crude rates of stroke could be standardised to allow appropriate comparisons with other datasets, both within and outside SSA.
A verbal autopsy (VA) study in a rural setting
AVA study has several advantages, including the availability of expertise in many of the countries in SSA where such approaches have already been used quite successfully. The design also allows an assessment of stroke in the context of other major diseases by first providing data on mortality and eventually morbidity. Such studies are relatively straightforward to perform in rural settings where communities are more stable and there are traditional communication networks to allow good capture of information on major events within an entire population. The validity of VA, however, is influenced by the spectrum of causes of death, the characteristics of the deceased, and several other factors, which would need to be considered. There are also costs associated with the access to geographically remote populations as well as the training of research staff and ongoing quality control. A study of this nature would also be required to have an adequate size and/or period of observation to achieve the required numbers of outcomes for power. Long period of observation raise questions about the consistent data, and a parallel validation study is almost always necessary to assess the validity of diagnosis derived from VA.
A multicentre, hospital-based, stroke registry study
A multicentre hospital-based stroke study involving many urban centres in SSA has several advantages over a single large-scale incidence study in urban setting. Large numbers of cases could potentially be collected over a relatively short period of time, and it would be possible to compare resources and outcomes within and across countries. However, the major limitations of this approach include the costs associated with the effort and infrastructure for coordination and communication between centres, as well as data capture and ongoing monitoring and quality control. In addition, the approach is limited by the very nature of it being hospital based. The degree of such selection bias is likely to vary considerably across centres, affecting both case mix and outcomes. The approach would therefore not provide a study population fully representative of incident cases and the natural history of disease and its management.
Conclusions
A combination of these approaches would probably overcome some of their respective limitations and improve the quality of estimates generated. Therefore, we consider the highest priority to be an incidence study undertaken in a representative urban population to be able to provide the most reliable estimates of the burden of stroke based on its ability to achieve near complete ascertainment of cases. Such a study could be complemented by a verbal autopsy study undertaken in a rural setting to provide estimates of stroke against the overall impact of chronic diseases.
Limitations and perspectives
SSA is a large and diverse multicultural and multiethnic region, which makes it difficult to quantify and compare the burden of stroke. There is clearly a dearth of published literature on stroke in SSA at large. Indeed, the challenges to performing high quality incidence and prevalence studies of stroke (and neurodegenerative diseases) are well known (72, 73). Cases are difficult to define and ascertain reliably in populations, and there are problems in relating events and the effects of different exposures to defined ‘at-risk’ populations (74).
Even accounting for the uncertainties in the prevalence of HIV/AIDS, as the populations of SSA undergo ageing and other structural changes, the importance of stroke and other non-communicable diseases is likely to increase considerably. Indeed, by 2025, about half of the populations of SSA will live in urban areas and the numbers of people aged 60 years and over will more than double in countries such as the Democratic Republic of Congo, Mozambique, Cameroon, and Ghana (75). With this rapid demographic transition, stroke is likely to become a more important cause of disability in SSA. Elevated blood pressure is the most frequent and important risk factor for stroke and other CVD, the prevalence of which is estimated to be around 20 million in the SSA. Diabetes mellitus, another risk factor, is rapidly increasing in SSA, driven by urbanisation, obesity and sedentary lifestyle.
Critical investments are required to improve surveillance and program-relevant research to provide an evidence base for policy development and effective stroke and CVD prevention and control. Action on stroke and CVD at large in SSA should go beyond just ‘primordial’ prevention as suggested by some authors (76). Aggressive risk factor control throughout communities, combined with high risk approaches, are urgently needed, along with health system realignment to incorporate acute episodes as well as the chronic management of non-communicable diseases.
Conclusions
In conclusion, this review highlights the high burden of stroke in SSA, which poses a significant burden on the prevalence of chronic diseases in these populations. Stroke in SSA occurs at an earlier age and is associated with a poor prognosis. High blood pressure is one of the major factors associated with stroke in this region and remains under diagnosed and inadequately managed. The magnitude of high blood pressure and other risk factors in SSA are already consistent and is expected to increase substantially (75, 77). Preventive measures (both primary and secondary) are urgently needed in this part of the world. High-quality stroke incidence studies, by compensating for the imprecise nature of the available data, will help map the epidemiology of stroke in SSA and serve as indicator of the true burden of CVD.
Footnotes
Acknowledgements
We thank Dr Myles Connor, Johannesburg for his comments and advice on the conduct of research on stroke in SSA.