
Abstract

Genetic factors predispose to stroke risk, although the magnitude of this contribution remains uncertain (1). Considerable effort is being invested in unravelling this genetic component but what does the practising stroke physician need to know about this rapidly advancing field? Monogenic (single gene) disorders raise very different issues from genetic predisposition to multifactorial stroke.
A large number of monogenic disorders can cause stroke (1). Many of these are part of systemic diseases where stroke is only one small part of the overall clinical syndrome and that rarely present to neurologists. However, a number of monogenic conditions frequently present with stroke, and for some of these, stroke is the only clinical manifestation. In many cases, such conditions predispose to only one stroke subtype. Diagnosis depends on both an awareness of the particular phenotype, and where relevant associated systemic features, as well as a careful family history.
Perhaps the most common genetic form of stroke is Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leucoencephalopathy (CADASIL). This autosomal dominant condition arises from mutations in the notch 3 gene (2). Although it is a systemic small vessel arteriopathy, pathological changes are most marked in the cerebral vessels and symptoms are limited to the brain. Recurrent lacunar strokes occur with onset usually between 30 and 50 years of age, although there is a variable phenotype (3). Migraine occurs in about two-thirds, usually with aura that may be prolonged. Depression may occur even before the onset of stroke, and is frequent with disease progression, subcortical cognitive impairment, and dementia. An acute encephalopathy with reduced conscious level, seizures, and cortical features may occur and this resolves spontaneously (4). Magnetic resonance imaging (MRI) shows a combination of lacunar infarcts and leukoaraiosis and also provides very useful diagnostic clues (Fig. 1). The presence of confluent anterior temporal pole involvement is both sensitive and specific, while involvement of the external capsule and corpus callosum are also useful pointers although less specific (5–7). Definitive diagnosis is made by detecting mutations in the notch 3 gene. There are a large number of potential mutation sites and most laboratories only screen for the most common mutations, which excludes between 60% and 90% of cases in different populations. Diagnosis can also be made on skin biopsy; the presence of granular osmiophilic material (GOM) in the vessel wall seen only on electron microscopy is diagnostic but skin biopsy may be negative in up to 40–50% of cases (7).
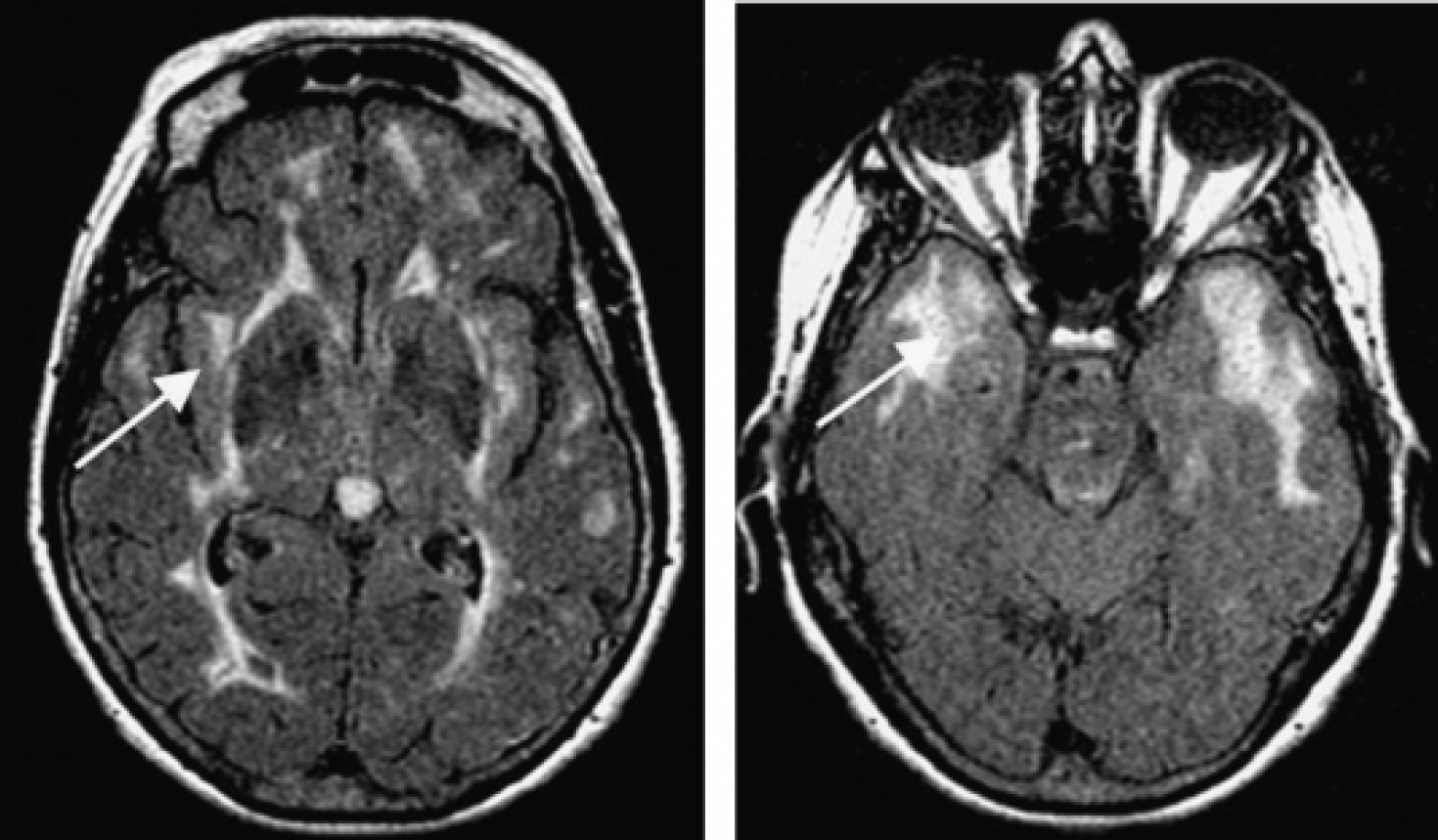
Characteristic imaging appearances of CADASIL. Anterior temporal pole involvement and external capsule involvement, both arrowed. [Figure originally published as Figure 13·2 (p. 314) from ‘Investigating a patient with stroke for genetic causes’ by Hugh Markus from ‘Stroke Genetics’ edited by Markus, Hugh (2003).]
Sickle cell disease is another important cause of monogenic stroke, particularly because preventative treatments are now available. This inherited hemoglobinopathy results from an amino acid substitution in the β-globin chain. Patients have often experienced other features of the disease, such as crises, before presentation with stroke, but stroke is an important complication and may affect up to 25% of patients by age 45 (8). Both occlusion of cerebral small vessels and a large vessel arteriopathy may occur. The latter can lead to tight stenosis or occlusion of basal intracerebral vessels and a subsequent moyamoya appearance. Therefore, presentation may be not only with ischemic stroke but also with intracerebral hemorrhage due to bleeding of new vessels and this is particularly common in adult patients. Asymptomatic intracranial stenosis can be detected by transcranial Doppler, or other noninvasive imaging techniques. Their presence has been shown to identify a group at a high risk of future stroke (9), and a randomized trial demonstrated that regular exchange transfusion markedly reduces this risk (10). A recent study found that whether stroke occurred in sickle cell patients could be almost entirely explained by a combination of modulating genes (11). This emphasizes the importance of gene–gene interactions.
Other monogenic causes of stroke include connective tissue disorders such as the Ehlers–Danlos syndrome resulting in large artery dissection, homocystinuria, which can cause arteriopathy of both the small and large arteries, and familial cardiomyopathies and dysrhythmias (1). Genetic prothrombotic disorders such as protein C and S deficiency are not uncommon and are frequently searched for in ischemic stroke (12). However, there is little evidence that they are major contributors, except perhaps in younger individuals (13). They are more important risk factors for venous thrombosis.
A recent study of over 700 subjects from Germany has suggested that Fabry disease may account for 4·9% of young (age range 18–55 years) cryptogenic stroke in males and 2·4% in females (14). This is an X-linked disorder resulting from mutations in the α-galactosidase A gene, which results in progressive accumulation of glycosphingolipids in various organs, predominantly vascular endothelial and smooth muscle cells, myocardial and renal epithelium, and the central nervous system. Important features include neuropathic pain and acroparesthesia, anhydrosis, and mucosal angiokeratoma. Severe morbidity may follow from cardiac and renal disease as well as stroke. Importantly, many of the cases in the stroke cohort were in patients without obvious clinical disease in other organs (14). Stroke is mediated by both large- and small-artery involvement with a preference for the posterior circulation. The most frequent sign of large artery disease is dolichoectasia of the basilar and vertebral arteries. Enzyme replacement therapy is now available and this seems to reduce the severity of pain, but whether it reduces the risk of recurrent stroke remains unknown. Although the disease is X-linked, it can result in clinical manifestations and stroke in women. Diagnosis can be made by enzyme testing in men, but mutation screening may be required in women. Further studies are now required to determine whether the disease is as frequent as recently reported in other populations with cryptogenic stroke.
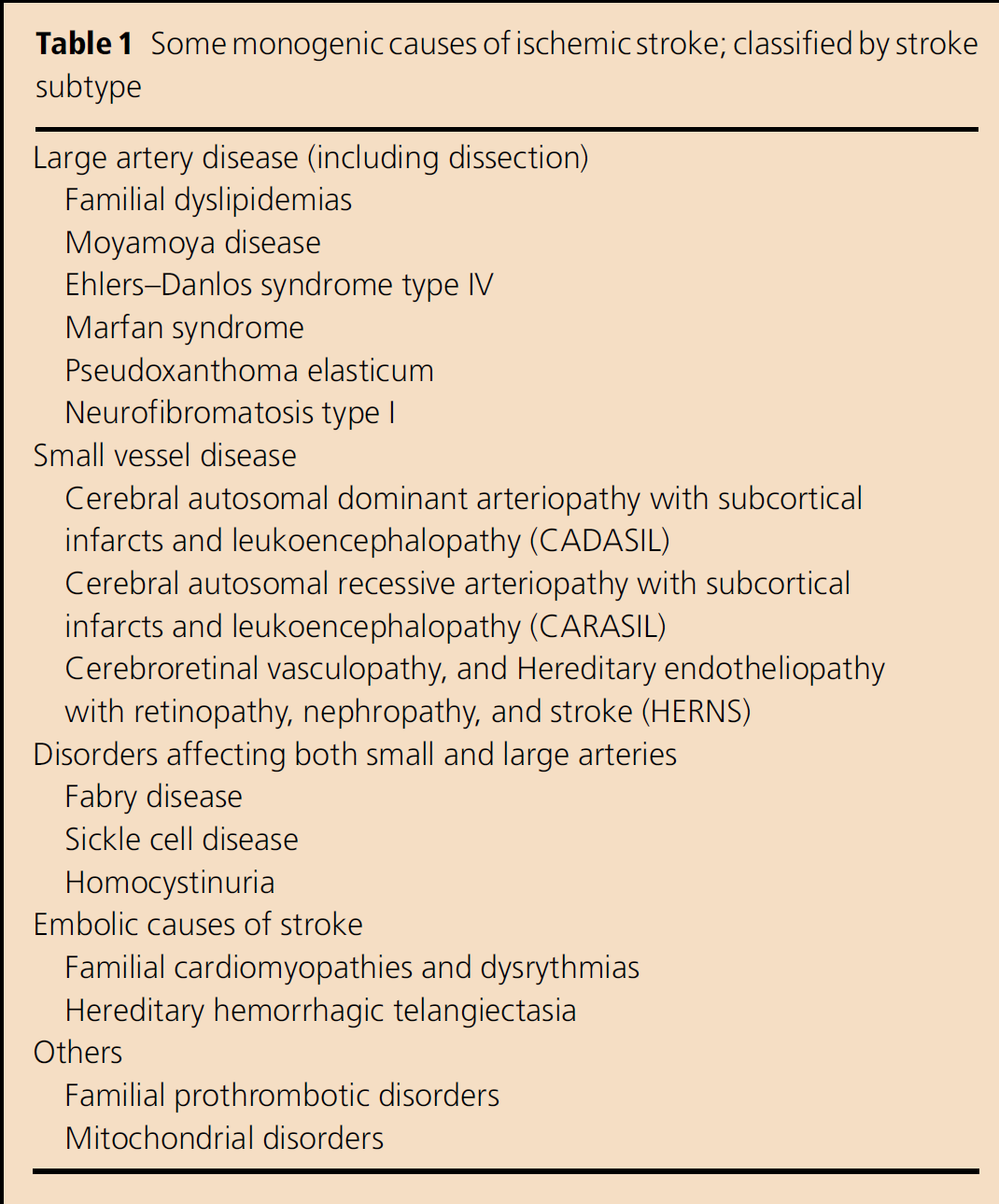
Some monogenic causes of ischemic stroke; classified by stroke Subtype
The diagnosis of monogenic stroke is undoubtedly important in the individual patient, but such cases account for only a small proportion of all strokes. The genetic contribution to multifactorial stroke is thought to be polygenic, although the number of genes involved is unknown. How might understanding the molecular basis help the clinician? A frequent justification is that it will allow genetic profiling of individual patients and better risk assessment. Rapid advances in genotyping may make this technically possible but the contribution of individual genes to stroke risk is likely to be small with odds ratios of perhaps between 1·1 and 1·5. While we struggle to adequately control conventional risk factors such as hypertension and smoking, such information may be less relevant to clinical practice. More importantly, in my opinion, understanding the molecular basis of stroke may provide completely novel insights into disease pathogenesis and therefore new therapeutic avenues.
Most genetic studies in polygenic stroke have been candidate gene case–control studies. In these, the frequency of a polymorphism or variant in a known candidate gene is studied in a population of cases and in controls. Such studies may confirm predefined hypotheses but will not identify novel genes. Nevertheless, they may be useful in determining whether particular pathways, such as the homocysteine pathway (15, 16), play a causal rather than a secondary role in disease pathogenesis. Despite a large number of candidate gene studies in stroke, there are few robust positive findings. This situation is common to many complex genetic diseases, not only stroke. It may reflect the multitude of genes involved, each with a small contribution, but is also likely to be due to methodological problems including small samples sizes and poor phenotyping of cases (17).
These complexities have encouraged researchers to study intermediate phenotypes. These are quantitative traits part way toward the final phenotype of ischemic stroke. They offer more statistical power for a number of reasons: they are continuous variables, performing large studies in normal controls is feasible, fewer genes may be involved, and they overcome the problem of subclinical disease whereby a control in a case–control study has subclinical cerebrovascular disease and is due to suffer stroke soon after recruitment. The two most widely used in stroke are carotid artery intima media thickness (IMT) measured on ultrasound and MRI white matter hyper intensities, as intermediate phenotypes for large and small vessel disease, respectively. Work with carotid IMT has emphasized the importance of gene–environment interactions in cerebrovascular disease, a theme that appears to be important in cardiovascular disease in general. Genes associated with enhanced inflammatory responses predisposed to increased carotid IMT in the presence of both ‘inflammatory’ environmental stimuli (such as smoking) and chronic infection (18, 19).
Both linkage-based approaches, and genomewide association scans, can identify novel genetic loci, and do not require a prespecified hypothesis implicating a particular candidate pathway. A linkage approach based on large extended pedigrees from Iceland has recently identified two possible novel pathways. A haplotype in the phosphodiesterase 4D gene (PDE4D) was associated with both cardioembolic and large vessel disease stroke (20). This association is biologically plausible. PDE4D selectively degrades the second messenger cAMP. Increased cAMP is associated with smooth muscle cell proliferation and migration, both key processes in atherosclerosis. The second pathway implicated is the leukotriene pathway which is involved in both leukocyte chemotaxis and inflammatory responses and vascular permeability. A haplotype in the ALOX5AP gene was associated with both ischemic heart disease and ischemic stroke (21). ALOX5AP codes for 5-lipoxygenase-activating protein (FLAP). Interestingly, a variant in another component of the pathway (5-lipoxygenase) was associated with increased carotid artery IMT (22). A number of studies have attempted to replicate associations with both of these pathways with varying results and the jury remains out. However, pharmacological inhibitors to both pathways are available and could represent new therapeutic tools (23).
The revolution in genotyping technology now allows genomewide screens of up to 500 000 polymorphisms (24). This offers the opportunity of using a case–control methodology to identify novel associations, and this approach is beginning to be used in complex diseases, with the most striking success in macular degeneration (25). The technology and associated bioinformatics are evolving fast and may make major contributions to unravelling the genetics of polygenic stroke. However, to do this well, large phenotyped DNA databases will be required of a greater ability than those used for most candidate gene genetic studies to date.