
Abstract
Atherothrombosis is responsible for most acute ischemic manifestations of atherosclerotic disease, including stroke. Individuals with evidence of atherothrombotic disease in one vascular bed have a significant risk of recurrence and show increased vulnerability over time for other manifestations elsewhere in the vasculature. Ischemic event rates for asymptomatic patients with multiple atherothrombotic risk factors appear to be similar to those in patients with documented cardiovascular disease. For example, diabetes mellitus and obesity are found at alarmingly high rates in patients with prior cardiovascular events, including stroke or transient ischemic attacks. Antiplatelet therapy is a key component of atherothrombotic event prevention. The results of the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance (CHARISMA) study showed that while dual antiplatelet therapy with aspirin and clopidogrel may not play a role in primary prevention, post hoc analysis alluded to the possibility of benefit for dual antiplatelet therapy in certain populations of stroke patients. We examined current recommendations for the prevention of atherothrombotic events, focusing on the role of oral antiplatelet agents in patients with ischemic stroke.
Introduction
Cerebrovascular disease (CVD) is a devastating disease with unacceptably high rates of mortality and disability. Annually, 700 000 individuals in the United States experience a stroke, of which 200 000 are recurrent attacks. Approximately 15–30% of stroke survivors are permanently disabled, and 20% require institutional care at 3 months poststroke onset. The substantial mortality and morbidity of stroke is reflected in the estimated economic burden of $62·7 billion for 2007 (1, 2).
Another manifestation of cerebrovascular disease is a transient ischemic attack (TIA), a serious event that often heralds further ischemic attacks and possible neurologic damage. Transient ischemic attack shares clinical features with stroke, but with resolution of symptoms within a few minutes, most lasting less than an hour (3).
The majority of strokes (87%) are ischemic in origin, often the result of atherothrombosis – a diffuse, generalized, and progressive vascular disease. Atherothrombosis rather than flow obstruction per se, is at the core of most of the acute ischemic manifestations of atherosclerotic disease, including ischemic stroke, unstable angina, acute myocardial infarction (MI), sudden cardiac death, and peripheral arterial disease (PAD) (4). The interaction of platelets with atherosclerotic lesions is central to this pathological process, whereby a platelet-rich thrombus forms on the surface of a ruptured or eroded plaque, causing partial or complete obstruction of blood flow (4, 5).
Studies in geriatric practice and data from the Framingham study have shown that clinical manifestations of atherosclerotic disease in one vascular bed are predictive of ischemic events in other vascular beds (6–8), a concept known as cross-risk. This explains why 20–40% of ischemic stroke patients may have abnormal tests for silent myocardial ischemia, and the risk of death (partly cardiac related) is at least twofold greater in stroke patients than in age-matched controls (9). Similarly, 25–60% of patients with carotid disease, but no symptoms of coronary artery disease (CAD), have abnormal results for provocative tests of myocardial ischemia or angiographic evidence of severe CAD (9). Consistent with the diffuse nature of atherosclerosis and the concept of cross-risk, individuals with PAD have a four- to fivefold greater risk of cardiovascular death compared with those without PAD (10). Evidence suggests that having a history of smoking, hypertension, and/or diabetes increases the cross-risk between the cerebral vasculature and the coronary arteries (11).
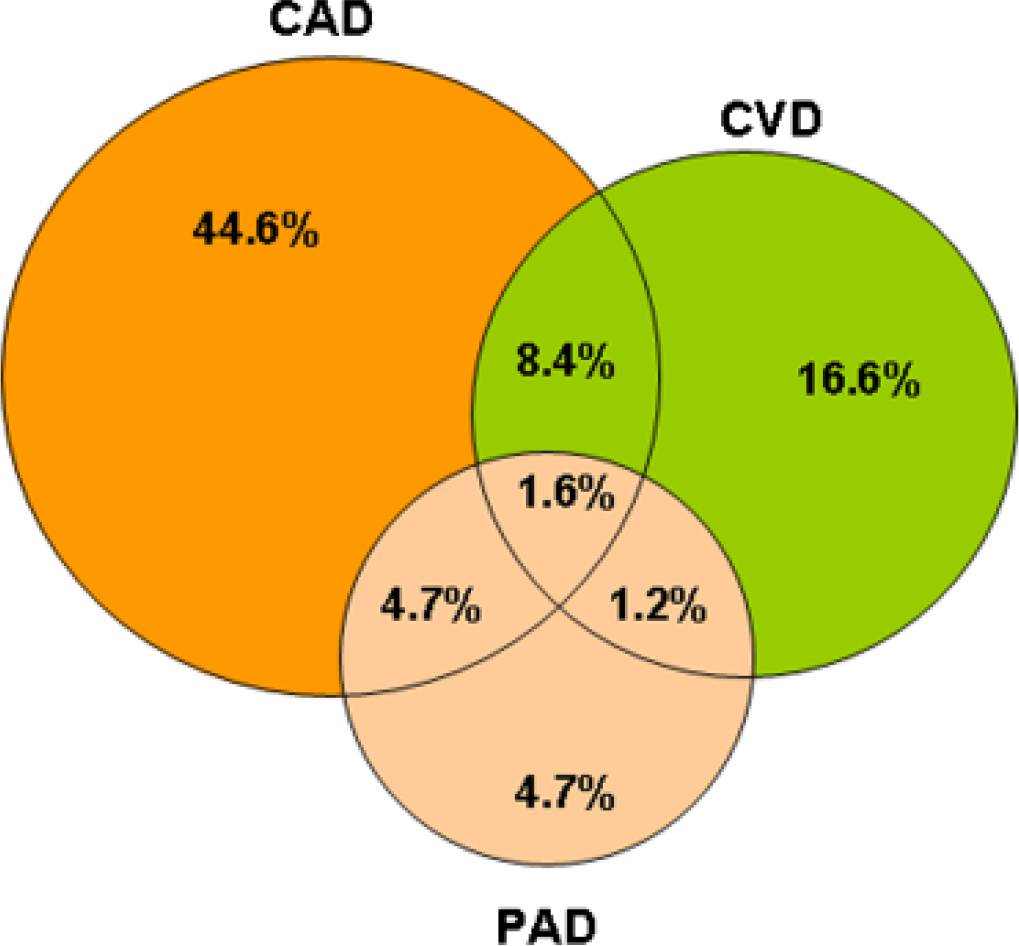
The Reduction of Atherothrombosis for Continued Health (REACH) registry, which included patients with multiple atherothrombotic risk factors in addition to those with documented atherothrombotic disease, showed that polyvascular disease was common among patients with established CAD, CVD, or PAD (12). Of the 67 888 patients enrolled in REACH, 81·7% had established disease in at least one arterial bed, 15·9% had disease in two or more beds, and 1·6% had atherothrombosis in all three vascular beds (Fig. 1). Cross-risk is also reflected in the long-term outcomes of stroke. In one study of patients with a first-ever stroke, 13% died from a recurrent stroke over a 10-year period, whereas 26% died from cardiovascular events (13).
Pathophysiology of atherothrombosis
The initiation of atherosclerotic lesions occurs as a result of the longstanding interaction between the endothelium and risk factors including smoking, hyperlipoproteinemia and diabetes. A host of molecular mechanisms further contribute to the pathology through upregulation of adhesion receptors and release of pro-inflammatory chemo attractant molecules that in turn recruit inflammatory leukocytes onto the growing plaque. Accumulation of extracellular lipid begins in the intima at this stage and attracts monocytes to the site of growing lesions, where they differentiate into macrophages with scavenger receptors that bind oxidized lipoproteins (5, 14). These macrophages engulf modified lipoproteins and become lipid-laden foam cells that eventually die, contributing their contents to help create the necrotic lipid core of the developing atherosclerotic plaque. Leukocytes and resident vascular wall cells release inflammatory cytokines and growth factors that further amplify leukocyte recruitment and foster smooth muscle cell migration and proliferation. Over time, inflammatory mediators upregulate the expression of tissue factors, potent activators of the factor VII/VIIa pathway, and activation of the metalloproteinase pathway of matrix-degrading proteinases that weaken the fibrous cap of the atherosclerotic plaque (5, 14).
Rupture of the fibrous cap exposes blood constituents to tissue factor within the atheroma, sparking a coagulation cascade under high-shear conditions of arterial flow that culminates in the formation of a platelet-rich thrombus (15, 16). Platelet adhesion, activation and aggregation at the site of vascular injury causes the release of thromboxane A2, serotonin, adenosine diphosphate, platelet-activating factor, and thrombin, which lead to further platelet recruitment, obstruction of the narrowed artery (17), and possible development of acute clinical manifestations (5, 14).
Risk factors for ischemic stroke
Risk factors that predispose patients to the development of systemic atherothrombotic disease are essentially the same across coronary, cerebral, and peripheral vascular beds, but the relative importance for some of them may vary between vascular territories (14). Patients who clinically manifest CAD, CVD or PAD, and asymptomatic patients with one or more cardiovascular risk factors and/or metabolic syndrome are at risk for recurrent or new atherothrombotic events (18). Notably, individuals with TIA are at substantial short-term risk of stroke and other atherothrombotic events (2). In order to reduce the risk of recurrent atherothrombotic events, various evidence-based guidelines have been compiled (19–24).
Hypertension [blood pressure (BP) > 140/90 mmHg] is the most ubiquitous cardiovascular risk factor, affecting approximately one-third of adults (≥ 65 million) in the United States (25). Furthermore, its prevalence is increasing due to higher rates of obesity and an aging population (26). Blood pressure lowering has been shown to significantly decrease the risk of stroke, MI, and vascular events in patients with a history of stroke or TIA (27). With regards to specific classes of medication, current data seem to suggest that inhibitors of the renin–angiotensin system, calcium channel blockers, and diuretics are more effective than β-blockers in preventing stroke (27–30). Specifically, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), and aldosterone antagonists may prevent or modify vascular remodeling and provide increased protection (31).
Another common risk factor for vascular disease is dyslipidemia. According to the current US National Cholesterol Education Program criteria, dyslipidemia is widespread in the United States as approximately 105 million (48·4%) people over the age of 20 have elevated total cholesterol (> 200 mg/dl), 79 million (32·5%) have elevated low-density lipoprotein (LDL) cholesterol levels (≥ 130 mg/dl) and 44 million (16·7%) have low high-density lipoprotein (HDL) cholesterol levels (≤ 40 mg/dl) (2). Clinical trials of statin therapy have demonstrated consistent benefits in reduction of stroke risk among individuals with stroke or CAD and elevated cholesterol levels, as well as among those with only mild to borderline elevations of cholesterol (32–40). Concern exists regarding extreme LDL lowering and possible hemorrhagic complications in stroke patients (32, 41).
Additional risk factors for stroke and other atherothrombotic events include obesity, diabetes mellitus, and smoking. Obesity [body mass index (BMI) ≥ 30 kg/m2] increases all-cause mortality rates by 50–100% above those with a BMI in the range of 20–25 kg/m2 (42), and diabetes mellitus (DM) is associated with risks of cardiovascular mortality and stroke that are about two to four times higher than those of individuals without diabetes (43). This is significant as the global population of adults with diabetes is expected to increase from 135 million in 1995 to approximately 300 million by 2025 (44). Although diabetes is a strong risk factor for stroke, tight glycemic control alone has not been shown to significantly decrease the risk of stroke (21). The significance of smoking as a risk factor for stroke, CAD, and PAD is evidenced by the inclusion of smoking cessation in current primary and secondary prevention guidelines for stroke, PAD, and acute coronary syndromes (19–24). While smoking in the United States has declined by 49% since 1965, 19% of women and 23% of men, as well as 25–32% of students in grades 9–12, report current tobacco use (2).
Stratification of patients according to risk
On the basis of population research, a range of risk factors have been incorporated into risk profiles that can be used to simply calculate the risk of an ischemic event in an individual for each clinical manifestation of atherothrombotic disease, including CAD and PAD (45–47). A number of different risk scores have been developed and utilized for stroke patients (48–52). A health risk appraisal function has been developed for the prediction of stroke using the Framingham Study cohort (48). This profile was based on the occurrence of 472 stroke events during a 10-year follow-up, and stroke probabilities were computed using the Cox proportional hazards model for each gender based on a point system. The risk factors included were age, systolic BP, use of antihypertensive therapy, diabetes mellitus, smoking, prior history of cardiovascular disease (CAD, cardiac failure, or intermittent claudication), atrial fibrillation, and left ventricular hypertrophy by ECG. The risk for stroke is particularly high following a first stroke or TIA (49). A six-point ‘ABCD’ score was developed and validated based on age, BP, and duration and features of symptoms, which were highly predictive of the 7-day risk of stroke following TIA (53). The Essen Stroke Risk Score was developed and validated for predicting the risk of a recurrent stroke and is a nine-point scale based on age, hypertension, diabetes, and a prior history of MI, other CAD, PAD, smoking, and ischemic stroke or TIA (52).
An individual's level of risk could be related to the average risk of stroke for persons of the same age and gender. The impetus for risk factor modification may be provided by information that an individual's risk of stroke is several times higher than average. Moreover, it may also be useful in the identification of individuals at substantially increased stroke risk as a result of borderline levels of multiple risk factors, such as those with mild or borderline hypertension, and facilitate multifactorial risk factor modification (48).
Antiplatelet therapy in secondary prevention
Aspirin
The AHA/ASA guidelines recommend low-dose aspirin for the primary prevention of CAD and stroke for individuals at a 10-year risk of CAD ≥ 10% (23). However, aspirin is not recommended for primary prevention of stroke in men without sufficient risk for CAD (21).
For secondary prevention, the benefits of aspirin are well established. Data from the Antiplatelet Trialists' Collaboration confirm the protective effects of aspirin 50–325 mg/day in patients at an increased risk of a cardiovascular event (54). A meta-analysis of two studies with a total of 2980 patients with a history of ischemic stroke or TIA revealed that aspirin decreases the risk of recurrent stroke by 20–30% (55). However, a second meta-analysis of 11 studies consisting of 13 587 patients with cerebral ischemia of arterial origin showed that aspirin decreases the risk of vascular events by only 13% (56). While aspirin remains the most widely used antiplatelet therapy, it is not without limitations. Aspirin ‘resistance,’ increased bleeding risks and potential interactions with non-steroidal anti-inflammatory drugs are concerns (56–61).
Clopidogrel
In over 19 000 patients in the Antiplatelet Trialists' Collaboration with a history of MI, stroke or PAD, clopidogrel produced a 10% relative reduction in the incidence of serious vascular events compared with aspirin (P = 0·03) (54). The Clopidogrel vs. Aspirin in Patients at Risk of Ischemic Events (CAPRIE) trial showed 75 mg/day clopidogrel to be more efficacious than 325 mg/day aspirin in patients with atherothrombotic disease for the composite endpoint of vascular death, stroke, MI, or rehospitalization for an ischemic event or bleeding (8·7% relative risk reduction; P = 0·043) (62). Although clopidogrel appears to be particularly beneficial in patients with PAD (62), diabetes (63), or a history of revascularization/ischemic events before enrollment (64, 65), the results should be interpreted with caution as they were obtained from post hoc (63–65) and predefined secondary (62) analyses. In a retrospective analysis of patients with a history of ischemic stroke or MI, clopidogrel was superior to aspirin in reducing the risk of the composite endpoint of ischemic stroke, MI, or vascular death (65). Similar to aspirin, resistance to clopidogrel has been reported (66), although there is currently no assay standard to establish resistance and no direct clinical correlation has been established.
Aspirin plus extended release (ER) dipyridamole
The European Stroke Prevention Study 2 (ESPS-2) of over 6600 patients with recent ischemic stroke or TIA demonstrated that the combination of aspirin plus ER-dipyridamole reduced the risk of recurrent stroke by 37% (P < 0·001), whereas aspirin alone only produced an 18% (P = 0·013) risk reduction and dipyridamole alone led to a 16% (P = 0·039) reduction. Compared with aspirin alone, the relative risk reduction of this combination therapy was 24% (P < 0·001) (67). More recently, this dual regimen was shown to significantly reduce major vascular events in an analysis of results from the European/Australian Stroke Prevention in Reversible Ischaemia Trial (ESPRIT) (68). European/Australian Stroke Prevention in Reversible Ischaemia Tria, an open-label study with blinded evaluation, examined the effects of aspirin 30–325 mg/day with or without ER-dipyridamole in 2739 patients who experienced a stroke or TIA within 6 months. In the combination therapy group, 13% of patients experienced the primary outcome of all-cause death, nonfatal stroke or MI, or major bleeding complications, compared with 16% in the aspirin monotherapy group, resulting in a relative risk reduction of 20%. A meta-analysis of six trials, including ESPRIT, with a total of 7795 patients allocated to aspirin alone or aspirin plus dipyridamole (any formulation) showed that the combination of aspirin and dipyridamole reduced the relative risk of the composite of vascular death, nonfatal stroke, or nonfatal MI by 18% (95% confidence interval, 9–26%) compared to aspirin alone (68). However, in both ESPS-2 and ESPRIT, adherence to the combination regimen was compromised by headaches associated with dipyridamole.
Aspirin plus clopidogrel
One potential mechanism how dual antiplatelet therapy may offer extra reduction in cerebral ischemic events has been demonstrated in the Clopidogrel and Aspirin for the Reduction of Emboli in Symptomatic carotid Stenosis (CARESS) trial that included patients with recent stroke/TIA and silent microembolic signals (MES) in the setting of significant internal carotid artery stenosis. Microembolic signals-positive patients have unstable carotid atheromas, experience more recurrent events that MES-negative patients, and MES are considered surrogate markers for ischemic cerebrovascular disease (69). The CARESS trial demonstrated that the combination of clopidogrel plus aspirin in patients with symptomatic carotid stenosis was more effective than aspirin alone in reducing the number of silent cerebral MES (69).
Treatment with the combination of clopidogrel plus aspirin has been shown to be more efficacious than aspirin alone in patients with acute coronary syndromes in the Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) trial (70, 71). Similar results of dual antiplatelet therapy were seen in patients with ST-segment elevation MI in the Clopidogrel and Metoprolol in Myocardial Infarction Trial (COMMIT) (72), and the Addition of Clopidogrel to Aspirin and Fibrinolytic Therapy for Myocardial Infarction with ST-Segment Elevation (CLARITY) trial (73).
However, in the Management of AtheroThrombosis with Clopidogrel in High-risk (MATCH) patients with recent TIA or ischemic stroke trial, addition of aspirin to clopidogrel resulted in a higher risk of life-threatening bleeding compared with clopidogrel alone (absolute risk increase of 1·3%), which offset the potential benefits in terms of a reduction in major vascular events over and above that observed with clopidogrel alone for secondary prevention of ischemic events in high risk patients with prior stroke or TIA (74). Results of the pilot phase of the Fast Assessment of Stroke and Transient ischemic attack to prevent Early Recurrence (FASTER) trial confirm the increased risk of bleeding associated with dual aspirin and clopidogrel therapy in patients with ischemic stroke and TIA (75). In this trial, 390 patients were randomized to receive aspirin (162 mg loading dose plus 81 mg/day) and clopidogrel (300 mg loading dose plus 75 mg/day) (± 40 mg/day simvastatin) or aspirin alone (± simvastatin) within 24 h of a minor stroke or TIA. At 90-days, patients who received both clopidogrel and aspirin had an insignificant 3·8% reduction in the risk of recurrent stroke compared with those who received aspirin alone (95% CI, 9·4–1·9%; P = 0·19) (75). However, those patients who received clopidogrel also had a significantly higher bleeding rate (P < 0·0001), attributable to both symptomatic and asymptomatic (i.e. bleeding) hemorrhages. Based on concerns about the event rate, the ability to recruit patients, and the safety of dual aspirin/clopidogrel therapy, a larger trial was deemed infeasible.
Against the background of MATCH, the Clopidogrel for High Atherothrombotic Risk and Ischemic Stabilization, Management and Avoidance (CHARISMA) trial was designed to determine whether dual antiplatelet therapy with clopidogrel and aspirin is superior to aspirin alone in terms of prevention in high-risk asymptomatic patients (with ≥ 3 risk factors) or symptomatic patients with documented CVD, CAD, or PAD (76). In CHARISMA, 15 603 patients were randomized to receive clopidogrel (75 mg/day) or placebo, in combination with low-dose aspirin (75–162 mg/day), for a median of 28 months. Results showed no overall benefit with dual antiplatelet therapy, with a similar rate of the primary composite endpoint of MI, stroke, or death from cardiovascular causes in both the clopidogrel/aspirin and placebo/aspirin groups (6·8% vs. 7·3%; relative risk 0·93; P= 0·22) (77). There was a nonsignificant trend toward an increased incidence of severe bleeding among clopidogrel/aspirin recipients compared with the placebo/aspirin group (1·7% vs. 1·3%; relative risk 1·25; P= 0·09) but no difference in the risk of primary intracranial hemorrhage (0·3% in both groups; relative risk 0·96; P = 0·89) (77).
Findings for the primary composite endpoint differed in the asymptomatic and symptomatic patient subgroups. Among the 3284 high-risk asymptomatic patients, a trend toward a higher rate of primary endpoint events was observed with clopidogrel/aspirin relative to placebo/aspirin (6·6% vs. 5·5%; P = 0·20), while the rate of death from cardiovascular causes was significantly higher with clopidogrel/aspirin than with placebo/aspirin (2·2–3·9%; P = 0·01). In this subgroup, severe bleeding occurred in 2% of clopidogrel recipients compared with 1·2% in the placebo groups (P = 0·07) (77). In contrast, in the subgroup of 12 153 symptomatic patients, clopidogrel plus aspirin was associated with a significant reduction in the incidence of the composite primary endpoint compared with placebo plus aspirin (6·9% vs. 7·9%; P = 0·045). The rate of severe bleeding was similar between the clopidogrel/aspirin and placebo/aspirin groups in this population (1·6% vs. 1·4%, respectively; P = 0·39) (77).
Results from the stroke substudy of CHARISMA were presented at the European Stroke Conference in May 2006, and showed that the incidences of nonfatal stroke and nonfatal ischemic stroke were reduced in patients receiving clopidogrel plus aspirin (78). Among clopidogrel/aspirin recipients, the incidences of nonfatal stroke and nonfatal ischemic stroke were 1·9% and 1·7%, respectively, compared with corresponding rates of 2·4% and 2·1% among placebo/aspirin recipients. This corresponded to relative risk reductions of 21% (P = 0·03) for nonfatal stroke and 19% (P = 0·07) for nonfatal ischemic stroke, respectively, in favor of dual antiplatelet therapy (78).
Several ongoing trials are examining the safety and efficacy of combination antiplatelet therapy in patients with cerebrovascular disease. The Secondary Prevention of Small Subcortical Strokes (SPS3) study is investigating the efficacy of aspirin vs. clopidogrel plus aspirin in patients with small subcortical strokes, while the Prevention Regimen For Effectively avoiding Second Strokes (PRoFESS) trial is comparing clopidogrel monotherapy to aspirin plus ER-dipyridamole for the prevention of secondary strokes (79). Patient enrollment was recently completed and the results of this trial are eagerly awaited. The Aortic arch-Related Cerebral Hazard (ARCH) trial is designed to compare the efficacy of aspirin plus clopidogrel vs. oral anticoagulant therapy in preventing vascular events in patients with atherothrombosis of the aortic arch and a recent cerebral or peripheral embolic event (79).
Conclusions
Some patient populations are at particularly high risk for atherothrombosis events, including ischemic stroke. It is important to modify the risk factors that predispose individuals to develop atherothrombotic events; this should include lifestyle modifications and pharmacotherapy. Oral antiplatelet agents are an integral component of pharmacotherapy for the reduction of atherothrombotic events in high-risk patients and have demonstrated efficacy in reducing the incidence of stroke in a number of clinical studies. Results from recent clinical trials have helped to clarify the role of oral antiplatelet therapy in risk reduction. The benefit of aspirin and ER-dipyridamole in preventing secondary stroke was confirmed by the results of ESPRIT and a subsequent meta-analysis. Results of the CHARISMA study showed that dual antiplatelet inhibition with aspirin and clopidogrel was not appropriate for primary prevention in asymptomatic patients with multiple risk factors. However, subgroup analysis suggests a possible benefit in certain symptomatic patients. Although an increased risk of bleeding remains a concern for patients on dual antiplatelet therapy, further study is needed, particularly among patients with lacunar stroke and aortic atheromas.
Footnotes
Acknowledgements
Editorial assistance for the development of this manuscript was provided by Richard Glover and Susan Abulhawa.
Disclosure: Preparation of this manuscript was supported by the BMS/Sanofi-aventis Pharmaceuticals Partnership. Dr Alexandrov serves on speaker bureaus for Sanofi/BMS partnership and Boehringer Ingelheim. Dr Alagona reports no conflict of interest.