
Abstract
Background The development of specialized stroke units has been a landmark innovation in acute stroke care. However, the high scientific evidence level for the recommendation for stroke units to provide clinical attention for acute stroke patients does not correspond to the level of stroke unit implementation. A narrative, nonsystematic review on published studies on stroke units was conducted, with special emphasis on those demonstrating their efficacy and effectiveness. We also attempt to provide some answers to several open questions regarding practical issues of stroke units.
The development of stroke units (SUs) has been a milestone in the care provision for patients who have suffered a stroke. From a nihilistic approach in which the clinical evolution of the patient was allowed to proceed uninterrupted, the care for these patients has progressed to being considered as a first-level neurological emergency. However, despite the high grade of scientific evidence on which the recommendations for SUs for care provision of the patients with acute stroke are based, there is no correspondence with the level of implementation of these SUs worldwide (1, 2). There are few studies and surveys analyzing the current population coverage from SU and the differences between countries are clear. In Scandinavian countries, up to 60–70% of stroke patients are managed in SU while in other European countries like the United Kingdom or Germany it reaches only 30–36% and in France or Italy < 10% (3). In Australia, only 19% of 261 acute public hospitals participating in a cross-sectional survey claimed to have an SU, and they did not treat all the stroke patients presenting to their hospitals (4). In the United States, data from a survey conducted in North Carolina showed that 45% of acute stroke patients have access to SU care (5). Finally, in the Canadian Stroke Network report in 2004, only 18% of acute stroke patients were admitted to an SU (6). Probably, in no other therapy with level I evidence based on randomized studies and meta-analyses has there been such a clear need for implementation of SUs. Our objective is to review the current issues associated with the provision of SU care from an international perspective.
Concept and historical development
SU is usually defined as ‘a geographic location within the hospital designated for stroke patients who are in need of rehabilitation services and skilled professional care that such a unit can provide’ (7). But several categories of SU have also been defined mainly based on admission policy (acute admission units, which admitted patients at stroke onset (within 1 week); delayed admission units, which admitted patients after a delay of at least 1 week and that are mainly focused on rehabilitation). On the other hand, mixed or comprehensive units are characterized by a combination of acute admission with a period of rehabilitation (7). Acute SUs are defined as those areas dedicated to the care (non or semi-intensive) during the acute phase and, once stabilized, the patient is transferred to the general neurology ward, where the diagnostic-therapeutic process continues up until the discharge from hospital, or transfer to rehabilitation or to geriatric units (8, 9).
To date, there exist some variabilities in the medical departments in which the SU are established: geriatric medicine, general medicine, neurology and rehabilitation medicine. Although all of these possibilities shared the multidisciplinary team care approach, general medicine and neurology are more focused on acute and more disease-specific approaches and geriatric and rehabilitation medicine on a more generic disability approach (7).
Although in several countries stroke expertise may reside within other hospital departments (e.g. general medicine, geriatric medicine), mainly depending on the Health Policy and on the different medical specialization developing and availability, acute SUs are recommended to be situated in a specific area within the Neurology department of the hospital and with dedicated beds. It should be of a multidisciplinary structure coordinated by a neurologist specializing in cerebrovascular disease, and with specially trained support personnel (9). There need to be predefine criteria of admission, explicit diagnostic and treatment protocols and work programs coordinated with other specialties such as cardiology, neuroradiology, neurosurgery, vascular surgery, rehabilitation and geriatrics. The activity of the SU needs to be continuous over 24 h/day; the physical presence of a neurologist on duty is a requirement (9). Further, it is recommended that the SU facilities include multiparameter noninvasive monitoring (EKG, oximetry, blood pressure and body temperature), together with a laboratory for blood analytic measurements as well as ultrasound for neurovascular assessment (transcranial and extracranial Doppler sonography) (7–10).
Since the 1950s, there have been several studies conducted with the objective of establishing an appropriate organizational model for stroke, focusing on aspects of rehabilitation (7). It was not until the 1970s that the idea of the SU was suggested for the first time. Initially, these were designed as intensive care units (ICUs), with facilities for monitoring and for the administration of intensive therapy. The patients admitted were those with severe stroke, with greater neurological deficit and poorer general status. Those with mild impairment or with a transient ischemic attack (TIA) were excluded. The results were very variable and did not show a clear reduction in mortality, although decreases in the numbers of complications were noted (11–15) (Table 1)
Nonsystematic selection of
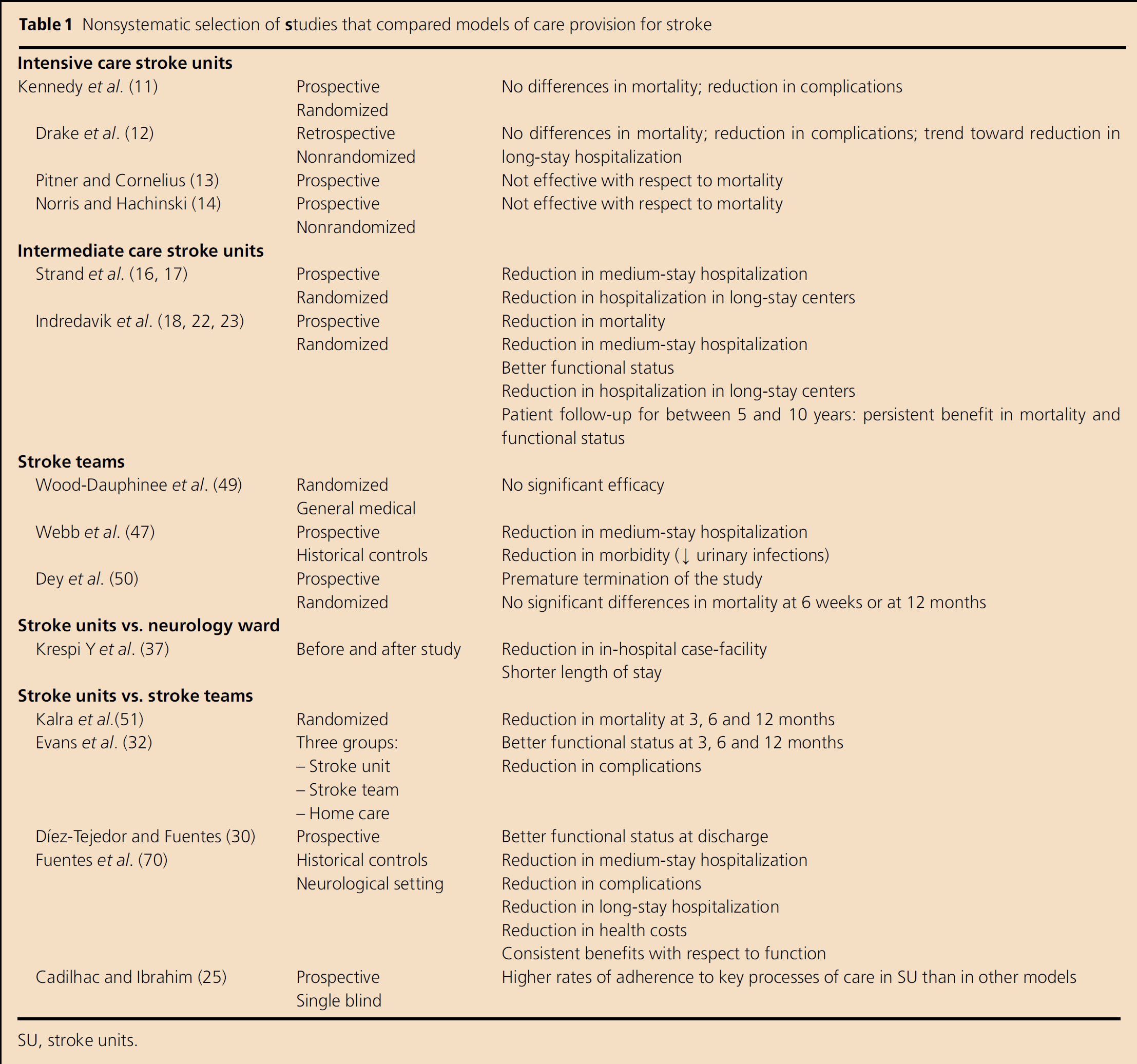
SU, stroke units.
Subsequently, in the 1980s, the concept of the SU evolved from acute, nonICUs characterized by a systemization of care provision for the patients and that involved trained personnel, preestablished criteria, with special attention being paid to the acute-phase treatment and the early functional rehabilitation and early return to society. This implied establishing a systematic diagnosis and precise therapy as well as an efficacious multidisciplinary approach. In the 1990s, interest in SUs was renewed following the publication of several studies comparing SUs with general medical wards that demonstrated the benefits in terms of mortality, functional recovery and in the rates of chronic institutionalization (16–19) (Table 1). Also, several meta-analyses confirmed the efficacy of SUs not only with respect to early mortality (28% reduction within the first 4 months) but also that at 1 year (21% reduction) (20). There was a reduction in the odds of death [odds ratio (OR) 0·86; 95% confidence interval (CI) 0·71—0·94], in the odds of death or institutionalized care (OR 0·80; 95% CI 0·71-0·90) and in the odds of death or dependency (0·78; 95% CI 0·68-0·89) (21). This means that the number needed to treat to prevent one death was 33, to prevent one patient being unable to live at home was 20 and to prevent one patient failing to regain independence was 20 (21).
Despite the grade I evidence of the efficacy of SUs based on randomized studies and meta-analyses, there has not been a generalized implementation of SUs, in contrast to that which occurred with specialized coronary care units. We intend to provide responses to the different questions raised regarding the practical utility of SUs. These include: are they effective in the management of stroke and are the benefits reproducible in standard clinical practice? Are there alternative models? Who benefits? Are SUs cost-effective? Is efficacy consistent within the time of operation? Is the effectiveness comparable to other therapeutic measures in the management of stroke patients? How can the outcomes be improved? For this purpose, a nonsystematic review of published studies that have specifically addressed any of those points of controversy or that have added relevant knowledge to those questions was conducted.
Are SUs efficacious in the management of acute stroke and are the benefits reproducible in standard clinical practice?
One of the most consistent benefits demonstrated in the randomized studies is the reduction in mortality, which is clearest in the analysis of early mortality (5 days to 6 weeks), the most frequent cause of death being pneumonia, recurrent stroke and pulmonary embolism. In the first week following a stroke, there are no significant differences with respect to the effect of SU. This is probably due to the fundamental cause of death in this period being directly related to the severity of the stroke and is not modifiable by any specific therapeutic intervention. From about 5 days onwards, however, a significant reduction in mortality is observed in the patients receiving attention in the SU compared with those receiving attention in the general medical ward (18, 19). Further, the results of follow-up over 5–10 days of patients attended to in the SU compared with the general medical ward show a higher long-term survival in the former, and that this reduction in mortality is maintained from the first 6 weeks. This indicates that it is the treatment in the acute phase in the SU that determines the better prognosis of the patients (22–24). Another important aspect to consider is the neurological recovery of the patients, because stroke is one of the principal causes of adult dependency. The studies that analyzed this aspect have shown that the functional status at discharge from hospital improves in those patients attended to in the SU compared with those in the general medical ward (18, 22–24). This, together with the reduction in mortality, is the most important benefit obtained with the SUs i.e. increase in survival at the cost of a greater proportion of patients being dependent would be a poor outcome for the SU.
Once the advantages of the care provision in the SU have been demonstrated, the factors that determine these benefits need to be evaluated, and whether the benefits observed in the randomized studies can be reproduced in standard clinical practice. In the Stroke Care Outcomes: Providing Effective Services (SCOPES) study, a prospective single-blind multicenter study conducted in Australia, the adherence to a selected set of clinically important processes of care, which included aspects of care within 24 h of admission, documentation and general management, was analyzed in three models of stroke care (equivalent to SU, ST and general medical care). The main findings were that the adherence to those predefined processes of care was associated with improved survival at discharge and that adherence to those processes of care was higher in SU than in other models (25). Similarly, in the PROSIT study performed in Italia, a higher quality in terms of infra-structure and organization in terms of diagnosis and the processes of care was found in the SU group. However, the effects of these components on the efficacy and effectiveness of stroke treatment had not been analyzed sufficiently in this last study (26). In 1997, the Cochrane meta-analysis, based on the observations of deaths from the illness, suggested that the benefits of the SU are related to a reduction in the secondary complications of the stroke, especially the relationship with the hospitalization of the patient i.e. the majority of the deaths avoided by the SU correspond to weeks 1–4 following the stroke (27). It has been highlighted that an early commencement of patient mobility and rehabilitation, together with stabilization of blood pressure, were the most important aspects in the health care provision in the SU (28). In an observational study in which the clinical evolution of the patients with acute stroke in the SU was compared with historical controls attended to by STs within the same department of neurology, the better attention to the overall care of the patient with a reduction in complications (systemic and neurological) was found to be independent good prognostic factor not only with respect to mortality or dependence but also chronic hospitalization (29–31). Further, a post hoc analysis of a randomized study that compared SU vs. ST concluded that the differences in the management of the patients (with respect to the diagnostic procedures and therapeutics) and the reduction of complications were the two factors that determine the greater efficacy of the SU compared with the ST (32). The importance of SUs in the reduction of complications, especially of infections and of mortality associated with them, has been confirmed recently in a systematic review (33).
Hence, it is evident that, apart from the organizational differences, one of the fundamental aspects of the SU is the specialized management of the patient in the acute phase, especially with regard to overall care, with strict control of the blood pressure, temperature, glycemia, oxygen saturation and prevention of complications. Maintenance of homeostasis in this phase has a direct impact on functional prognosis in the short term (31, 34). Differences in the management of these physiological parameters of the patients in acute phase determine, in great part, the different stroke-related mortality rates in different countries (35). Further, the benefits of SUs are reproducible in standard clinical practice and result in an increase in patient transfer to home care and improvement in functional status (29, 30, 36–38).
Are there alternative models for care provision following stroke?
Nonneurological care: The majority of SU trials were conducted in nonneurological wards and the benefits when compared with general wards without specific stroke care programs is clear. To date, there exist some controversies regarding which medical specialist should manage acute stroke patients (39–41). However, there are some studies suggesting that specific neurological care could provide additional benefits to stoke patients. Already in 1995 a randomized study that compared the efficiency of the Neurology Department vs. that of Medicine demonstrated a mean reduction in hospital stay, improved the functional status at discharge from hospital and an increase in the number of patients capable of returning home in the group that was attended to in the neurology ward (42). This was reinforced by a multicenter study of the Spanish Stroke Study Group, which demonstrated that early care (within the first 6 h) by the neurologist was related to a better functional prognosis and shortening of hospital stay (43). Other observational studies have shown better outcomes in patients treated by neurologists as compared with other specialists (44–46). Thus, in our opinion, although a multidisciplinary approach is the basis of SU care, neurologists should have a key role in SU organization as it is recommended by some societies (8, 9). In fact, in many countries in Europe, SUs are predominantly set up in neurological departments (1).
Stroke teams (STs): These are defined as multidisciplinary teams available for the care of stroke patients in any hospital environment. Generally, this would be composed of one or two neurologists, a physiotherapist or occupational therapist and a nurse specialized in care of the stroke patient. There have been few studies conducted to assess the efficacy of STs. Initial studies highlighted a benefit of STs in relation to the mean reduction in hospital stay and in morbidity (decrease in urinary infections) (47). Subsequent observational studies, randomized trials and meta-analyses (29, 29, 51) that compared STs with general medical wards (49, 50) and with SUs (30) confirmed that the STs are not an effective alternative in the care provision for patients with acute stroke (21, 21, 52). Nevertheless, in those centers in which it is not feasible to set up SUs, the ST could be considered as a valid organizational option but always with the premise that those ST be integrated in a Stroke care network with tight collaboration with a reference center with an SU (Comprehensive Stroke Centre) (54).
Care pathways: There have been, over the past few years, new tools of clinical administration developed of note, among which are clinical decision trees. This deals with care-provision plans that define and regulate sequences of health-care activities or interventions for a defined group of patients with a predictable clinical course and whose principal objective, is to provide quality care for the patient based on the best scientific evidence available. A further objective is to avoid the interindividual variation between health-care professionals. When analyzing its efficacy in general neurology wards, set up as an alternative to SUs, there were no benefits observed with respect to the management of the patients whereas, conversely, there was a trend towards a poorer clinical evolution of the patient (55).
Which patients benefit from care in SUs?
Starting from the premise that, to achieve a benefit, all patients with stroke, independent of severity, age or comorbidity should be attended to in SUs, it is clear that on many occasions the resources available in the SU, especially with respect to bed availability, are limited. A health-care political priority would be to select those patients who may benefit from SU attention. Hence, in the studies published on SUs, there has been, with disturbing frequency, a search for a patient profile that would best benefit from the specialist attention. To date, there have been analyses based on the severity of the stroke, age of the patient, presence of comorbidity and stroke sub-type.
Analysis of the clinical evolution of the stroke patient attended to in the SU compared with the general medical ward with respect to age and grade of neurological involvement have highlighted the presence of hemiparesis on admission to hospital and advanced age as factors determining mortality and/or dependency. The effect of age depends on the moment in which its impact is evaluated. For example, patients <75 years of age are those that benefit most from attention in the SU in the short term because this attention accelerates the patient's neurological recovery; in the long term, however, the recovery will be the same if the patient was attended to in the general ward. Conversely, in patients >75 years of age, the differences are modest initially but become statistically significant in favor of the SUs in the years following the stroke (17). Another circumstance that has been considered is the presence of comorbidity especially in relation to the presence of concurrent heart disease i.e. patients with cardiac disease benefit more at 3 months in terms of mortality and/or institutionalization when attended to in SUs (17, 56).
The Cochrane meta-analysis of 2002 analyzed the differences between sub-groups of patients. The main conclusion was that the benefits observed with the organized care and specialized for stroke were not confined to a specific patient sub-group. The analysis highlighted that clear benefits were obtained in patients of either gender, of different age ranges and independent of the grade of neurological involvement. The more severe stroke patient groups have a higher mortality risk inherent in the severity of the stroke, and are those patients who benefit most in terms of mortality or dependency rates, the benefit being less evident when mortality and institutionalized care were assessed (21). Also of note is that patients with preexisting functional dependency were not included in randomized studies on SU but data from observational studies suggest that they do not obtain a clear benefit from SU attention (57).
With respect to the stroke type, a few authors have analyzed the possible differences in the benefits from SU care in terms of mortality and functional recovery, despite the known differences in prognoses. In a post hoc analysis of a randomized trial that compared SU against ST and home care, the prognostic differences and associated costs were evaluated in patients with nonlacunar cerebral infarction (CI) compared with patients with lacunar strokes attended to in the SU vs. those receiving ST attention in the general ward. In the group of patients with large-vessel CI, attention provided by the ST was associated with higher mortality probability at 3 months and at the end of 1 year and also mortality and institutionalization. In the group with lacunar infarction, no significant differences were observed in the prognosis at 3 months or at 1 year between the two organizational models. However, there were higher costs resulting from an increase in the mean hospital stay and greater use of resources (physiotherapy, occupational therapy and logopedia) (58). Nevertheless, the patients with lacunar strokes benefited from SU attention as well, with a reduction in complications and hospital stay apart from achieving a better functional status at discharge from hospital. The significant increase in patient independence was clearer in the multivariate analysis in which being treated in the SU was an independent factor for a better prognosis with respect to the dependency variable (59).
In relation to cerebral hemorrhage (CH), there have been few studies that have specifically evaluated the benefits of SU in the management of CH. The possible benefit (mortality reduction) in the patients with CH attended to in the SU compared with those in the general medicine ward and compared with those receiving attention in the ST in the neurology ward was noted for the first time in 1998 (60). The study demonstrated a reduction in complications, mean hospital stay and improvement in functional status associated with the SU. Subsequently, in a controlled prospective study in which 121 patients with stroke were randomized to an SU or to a general medical ward, a significant decrease in mortality at 30 days and at 1 year was found in favor of the SU (61).
The majority of the studies that analyzed the efficacy of SUs or STs did not include patients with TIA, and there are few studies on the short-term prognosis or the diagnostic and therapeutic implications of care provision for TIA. In observational studies, care provision for patients with TIA in the SU was associated with a reduction in the mean hospital stay, health-care costs and improved diagnostic efficiency compared with those attended to in the same neurology ward by the ST (29) with earlier application of specific treatments (62).
In summary, all the patients with acute stroke, independent of age, severity, cardiac comorbidity or stroke sub-type, benefit from care provision in SUs.
Are SUs cost-effective?
Taking into account elevated health-care costs and limitations on resources, it is necessary to identify care-provision models that are not only efficacious but also efficient. The costs of acute stroke derive from hospital costs while, in the long term, the costs are related mainly to the grade of the residual incapacity of the patients. Direct costs are those derived from the use of the health service resources (drugs, nursing care, rehabilitation,…) and indirect costs are those that are implied in the loss of productivity of the subject who has suffered a stroke. At the time of assessing those with stroke, we need to consider different variables: those in the acute phase, fundamentally attributable to hospital costs and directly related to the mean hospital stay, and those of the long term, which are derived from the care of the patient with functional dependency requiring rehabilitation, short-stay hospitalization, long-stay hospitalization, home care, etc (63). Clearly, the care organization model that shows a reduction not only in the mean hospital stay but also in the percentage of patients with dependency at discharge from hospital can be considered as the more cost-effective system.
The care provision in the several models of SU (acute care, rehabilitation or mixed) is associated with a reduction in the mean stay in hospital, despite the heterogeneity in the calculation of this variable (hospitalization in the acute phase, overall duration of hospitalization and long-stay institutions) as demonstrated in individual studies and in systematic reviewers (16, 21, 29–30, 37, 47, 64–66). This reduction in hospital stay is associated with a reduction in hospital costs (30). Further, SU care achieves an increased transfer to home care with less long-term hospitalization (16–19, 27, 29, 30). Further, if we consider that the SU improves the functional status at discharge from hospital and that fewer patients are discharged to home-care with physical dependencies, we observe a greater effectiveness of SU, whose repercussion is a reduced burden on family and on society.
With respect to the cost-effectiveness from the point of view of the health economy, it has been highlighted over the past few years that SU implementation has an increased cost due to the increase in personnel and of the diagnostic/therapeutic procedures, which reach 7% of the cost of the admission to hospital and 15·6% if we consider the mean costs per day of admission to general neurology wards (67). However, although the costs related to resource use are generally higher in SU as compared with conventional care, but similar to mobile service, when outcomes are included in the analysis, SU appears to be more cost-effective than either mobile stroke teams or general medical care because of the potential health benefits that can be achieved (68).
On the other hand, with the objective of calculating the clinical and economic consequences of establishing SUs compared with conventional care, the study conducted by Launois et al. (69) in France is of considerable interest. Focusing essentially on administration, the authors performed an analysis in which the important variables included were the grade of incapacity of the patients, the destination on discharge from hospital and probability of stroke recurrence. These variables were in addition to those usually considered in economic studies on care provision such as the probability of death or survival and the specific model of care provision. As such, the study could be considered as the most comprehensive cost-effectiveness study of stroke care provision conducted to date. The study not only confirmed that the SU results in a higher patient survival rate without sequelae in the 5 years of follow-up but also, and more significantly from the perspective of the administrative process, the SU cost-effectiveness ratio is much lower than the threshold of acceptability recognized by the scientific community. This finding justifies, as highlighted by the authors of the study, the need for organizational changes in the care provision for stroke patients, and that it is essential that SUs are established in France. Certainly, these data cannot be extrapolated to other countries but they do provide important departure points, demonstrating, from the clinical administration perspective, that the SUs are superior to conventional care not only in terms of efficacy but also cost i.e. the implementation of such units is clearly justified.
Are the benefits of SUs consistent over the time they have been in operation?
The majority of long-term studies performed have focused on the follow-up at 5–10 years of patients initially attended to in SUs. The authors of these studies demonstrated high survival rates in the long term and an increase in the patient's capacity to return home (22–24). However, what remains to be determined is whether the efficacy of the SU is maintained over the period in which the SUs have been operating. This question is of considerable importance because a possible bias in the analysis of efficacy of a new organizational model is the motivation and enthusiasm of those health-care professionals involved in the initial implementation of such units. Further, almost all randomized trials compared SUs with the attention provided to stroke patients in other non-specific wards in which the personnel did not follow the same protocols or guidelines for the management than in the SU groups. As such, some of the favorable results observed for SUs could be a reflection of the greater dedication and specific care provided by the SU personnel (7). Thus, the good outcomes not only in the acute phase but also in the subsequent follow-up of the patients in these studies could be due to the differences in the clinical management related to each of the care-provision models during the hospitalization phase, and not due to a real benefit of the SU per se. The response to this criticism is that an analysis has been performed of the functional status at 8 years of the SU that demonstrated that the benefits of the SU in terms of reductions in the mean hospital stay, mortality/dependency and institutionalization were maintained over the period of 8 years analyzed and that, indeed, over the last few years, further reductions in the mean hospital stays, intrahospital complications and a higher percentage of survival have been achieved (70). As such, as with the health-care personnel and diagnostic protocols/therapies, it is the specific attention provided in the SU that determines the good results, and that have been consistent over the time they have been in operation.
Is SU effectiveness comparable to other therapeutic measures in the management of stroke patients?
In 1999, Hankey and Warlow published an analysis of the effectiveness of the different treatments available for acute-phase CI, such as aspirin, fibrinolytic treatment tissue-type plasminogen activator (rt-PA) and attention received in SUs. The authors considered the impact of the application of these treatments at the level of the community and on the overall stroke load. Although thrombolysis would be the therapeutic measure with the best numbers needed to treat (NNT; 16 for thrombolysis vs. 18 for SU and 83 for aspirin), the analysis of mortality and/or dependencies avoided showed 8·3% for SU vs. 1·2% for thrombolysis and 1·8% for aspirin (Fig. 1) (71). The cost-effectiveness analysis highlighted that the SUs are highly cost-effective because they achieve an absolute benefit similar to thrombolysis but can be applied to greater numbers of patients (71). These data have been confirmed in a study conducted by Gilligan and colleagues in which the eligibility of the different specific treatments available (including further hypothetical data on neuroprotection deduced from clinical trials) was analyzed in a group of acute-stroke patients attended to in the hospital, and the results were extrapolated to the general population. Of the patients, 83% would be candidates for management in a specialized SU, 40% to treatment with aspirin in the first 48 h and only 10% to intravenous thrombolysis with rt-PA in the first 3 h (Fig. 1). The authors concluded that greater benefit to the community is achieved with SUs and that although all these therapeutic measures should be accessible to the acute-stroke patients, access to the SU needs to be considered a priority (72).
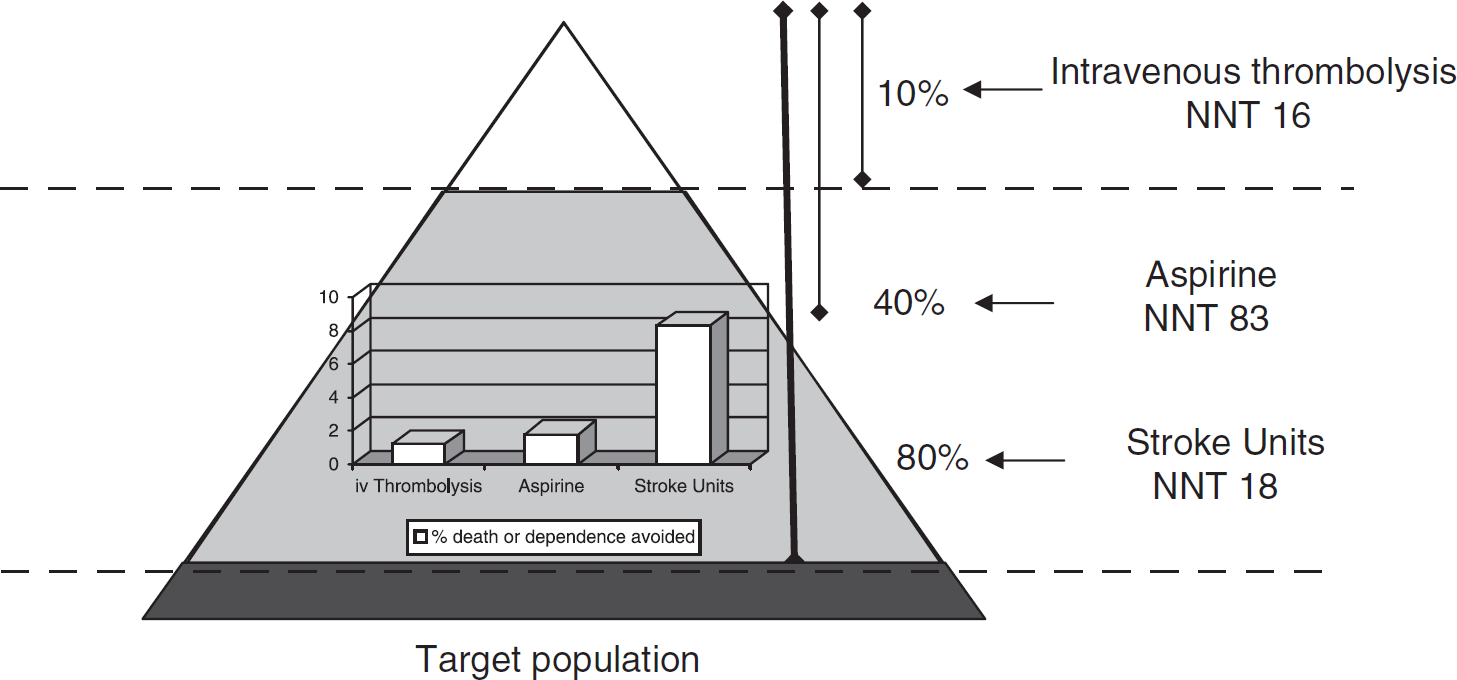
Effectiveness of the different treatments available for acute phase confidence interval (CI).
How can we improve the results of the SUs?
Monitored SUs: Over a considerable period of time, the early rehabilitation has been considered as the most important component and determinant of efficacy. However, the study by Indredavik et al. (28) highlighted the possible influence of general care, particularly in relation to the control of blood pressure and the early treatment of hypothermia; the importance of maintaining homeostasis of the patients is becoming progressively more evident in terms of short-term prognosis (34) and the reduction in the complications (30, 32, 33, 73). These beneficial effects have been demonstrated in the SU in which vital signs are noninvasively measured four times daily. Over the past few years, several studies have been published highlighting the importance of continuous monitoring of these parameters and the implication in the patient's prognosis and have demonstrated lower mortality rates at 3 months (74) and at 1 year (75). This benefit is probably due to a better detection of complications (cardiac events, fever, hypertension, hypotension and hypoxia) in the monitored patients and, hence, a more rapid deployment of appropriate therapy. Because a lack of a properly designed study of conventional SU with physiological variable measurement (blood pressure, cardiac frequency, body temperature and oxygen saturation) four times a day compared with SUs with continuous monitoring of these same variables, there continues to be considerable controversy on the convenience and/or the desirability of SUs with continuous monitoring (76–78). Currently, the cost on continuous monitoring in SUs is advisable, but it is not vital to implement a new SU in such a manner that the cost of acquiring noninvasive monitors does not convert to being inconvenient, being sufficient to monitor these vital signs clinically because only this model of SU (nonmonitored) has demonstrated cost-effectiveness in randomized trials.
Care pathways: There have been several studies on the implementation of care pathways of administration in the care provision of stroke patients. These have focused on aspects of rehabilitation and without analyzing the impact of these clinical routes on acute-phase stroke. The emphasis has been on increasing the diagnostic tests and reducing the risk of urinary infections, and of re-hospitalization. However, there is insufficient scientific evidence regarding their benefits in the prognosis of vital function and status. As highlighted by the Cochrane reviews (79–81), this is due to methodological limitations such as a nonrandomized design in the majority of trials. Only one study with historical controls had analyzed the impact of the introduction of a new stroke care pathway in an acute SU. The study showed a greater quality in the process of diagnosis and a reduction in the urinary infection as an intrahospital complication (82). Further, the care pathways specifying the day-to-day diagnostic and therapeutic measures that need to be applied to the stroke patients assure a continued quality of care provision. The process should also include greater monitoring and follow-up on weekends and holidays. Admission into the SU on the weekend or in vacation periods has been shown to be associated with a higher mortality rate and poorer functional recovery, which can be attributed to decreased numbers of clinical personnel, a lower multidisciplinary treatment intensity and a delay in the rehabilitation process (83, 84). Hence, it is necessary to ensure continuous care in the SU that includes not only an adequate proportion of nursing care but also continuity in the diagnostic processes, together with physiotherapy and rehabilitation, including on weekends and holidays.
Final considerations, SUs: scientific and social demand
Since 1995, the World Health Organization (WHO) and the European Stroke Committee have implemented the Declaration of Helsingborg in which it was specified, as an objective to be achieved by the year 2005, that all stroke patients in the acute phase should have an early, and specialized, evaluation and treatment in an SU. In the year 2006, the revised Declaration of Helsingborg declared that by the year 2015 ‘all patients in Europe with stroke will have access to a continuum of care from organized SU in the acute phase, to appropriate rehabilitation, and to secondary prevention measures’ (85). Neurology scientific societies insist on the need to establish SUs in the majority of hospitals, the option of STs being acceptable only when it is not possible to implement SUs (86–91).
Based on the scientific evidence, specialized neurology care provision for stroke patients is not only a necessary and cost-effective facility but also a social demand (92). As such, for example in Spain, the Associations of Neurological Diseases and the Spanish Society of Neurology [Sociedad Española de Neurología] developed the ‘Madrid Declaration’ [Declaración de Madrid] in 2000, which proclaimed ‘the right of all citizens to receive attention by an expert with specialist competence in the different neurological pathologies, to have access to up-to-date diagnostic and therapeutic techniques, and to be attended to by specific interdisciplinary units in which they can obtain all the help necessary for their health problem, with guarantees of it being the best quality possible’ (93). More recently, the Defensor del Pueblo in his report on overcoming cerebral damage, recommended that the Health Authorities should emphasize the early and specialized care for stroke patients by creating specialized SUs to provide sufficient cover for the total population (94). A questionnaire conducted among 1713 stroke patients receiving attention in hospitals in the United Kingdom had a higher percentage of satisfaction with the language and communication skills of the carers, with the basic activities such as hygiene and alimentation, together with the planning of care, rehabilitation and physiotherapy at discharge from hospital as well as a greater confidence in the health-care personnel (95).
In summary, the SU is the most efficacious care organization model for acute stroke, even in comparison with STs. All patients suffering from a stroke can benefit from attention in the SU. These units are efficient and cost-effective, and consistent over the time period of their operation. When the community benefits of the different specific treatments for stroke such as aspirin and intravenous thrombolytic agents are considered, the SUs have a higher target population potential and a higher benefit in terms of numbers of deaths or dependencies avoided. As such, the SU is a necessary care-provision facility that is also cost-effective.