
Abstract
Background and Purpose
The improved outcome (survival and function) of stroke patients admitted to multidisciplinary stroke units (SU) in developed countries has not been replicated in developing countries in sub-Saharan Africa. This study documents the outcome of patients admitted to the first multidisciplinary SU opened at a secondary hospital in Cape Town, South Africa.
Methods
Patient outcomes including in-hospital mortality, resource utilization (length of hospital stay, CT brain scans performed, and tertiary hospital referral), and access to inpatient rehabilitation were recorded for all patients admitted to the hospital for 3 months before initiating multidisciplinary stroke care and for 3 months after implementing multidisciplinary stroke care.
Results
One hundred and ninety-five patients were studied; 101 of these were managed in the SU. Inpatient mortality decreased from 33% to 16% after initiating multidisciplinary stroke care (P = 0·005). The length of hospital stay increased from a mean (SD, 95% CI) of 5·1 (6·5, 3·8–6·4) days to 6·8 (4·5, 5·9–7·6) days (P = 0·01). Referral to inpatient rehabilitation increased from 5% to 19% (P = 0·04) for those who survived to discharge. The number of CT brain scans performed and the number of referrals to the tertiary academic hospital did not increase significantly.
Conclusions
Multidisciplinary stroke care was successfully implemented in a resource-constrained secondary-level hospital in South Africa and despite the limitations of the study, the significant reduction in inpatient mortality and increase in referral for inpatient rehabilitation would suggest an improvement in stroke care. Resource utilization in terms of length of hospital stay increased by a mean of 2 days but the number of CT brain scans performed and referral to a tertiary hospital did not increase significantly.
Introduction
Patients treated in stroke units (SU) have been shown to have a better outcome than those treated in general wards (GW) (1–5). Meta-analyses of all available controlled trials indicate that treating patients in SU reduces mortality, institutionalization, and dependency (6–8). Comparable benefits have been observed in SU care in routine clinical practice, proving that the benefits seen in clinical trials can be replicated in routine practice (9). Many studies have also shown SU to be cost effective (10–12). Despite this overwhelming evidence favoring the use of multidisciplinary SU, even well-funded health care services provide only limited access to SU care. In the United Kingdom, 46% of stroke patients access SU care while in Italy <10% do so (13, 14). Very few studies have assessed the efficacy of SU care in developing countries, and the favorable outcomes demonstrated in developed countries have not been replicated in sub-Saharan Africa.
The poor standard of stroke care available in GW in sub-Saharan Africa can be inferred from stroke mortality data. While an overall case fatality rate of 23% is reported from developed countries, in-hospital mortality rates range from 41% in Gambia to 50·3% in Ghana (15–18). Reported 1-month mortality figures exceed 30%: up to 33% in South Africa (only black Africans studied), 38% in Senegal, and 40% in Nigeria (19–23). These studies, all conducted in tertiary referral hospitals, represent the highest level of care available to stroke patients in these countries.
The first multidisciplinary SU to be established in an urban-secondary level hospital in South Africa was opened at GF Jooste Hospital in March 2002. This 200-bed hospital serves an estimated population of 1·5 million Cape Town residents; most of these residents are poor, have limited education, and are largely unemployed (24). Annually, the hospital admits approximately 6600 medical patients; approximately 400 of these admissions have stroke as a primary diagnosis (25). This study examined the impact of multidisciplinary stroke care on the in-hospital mortality, resource utilization, and access to inpatient rehabilitation facilities for stroke patients admitted to the SU since its inception in 2002.
Subjects and methods
Patient selection
All patients admitted from the Emergency Unit (EU) with a clinical diagnosis of stroke, as defined by the World Health Organization, within 7 days of onset, were reviewed (26). Stroke patients were identified from ward admission registers as any patient with a primary admission diagnosis of cerebrovascular accident, stroke, or hemiplegia. All patient records were reviewed and patients with a subsequent diagnosis of subarachnoid hemorrhage, tumor, or other nonvascular lesions were excluded from further study. Data were gathered for all stroke patients admitted 3 months before opening the SU (1 December 2001 to 28 February 2002) and 3 months after initiating multidisciplinary stroke care at the hospital (1 March 2002 to 31 May 2002). The study was approved by the Research Ethics Committee of the University of Cape Town, South Africa.
Data collection
Patient demographic data, length of hospital stay, transfer to a tertiary hospital, and inpatient mortality were collected from ward registers. Computerized tomography (CT) brain scan data were collected from patient records and verified by reviewing CT brain scan registers (Table 2).
Demographic data, in-hospital mortality, resource utilization, and referral to inpatient rehabilitation facilities for stroke patients admitted to GF Jooste Hospital
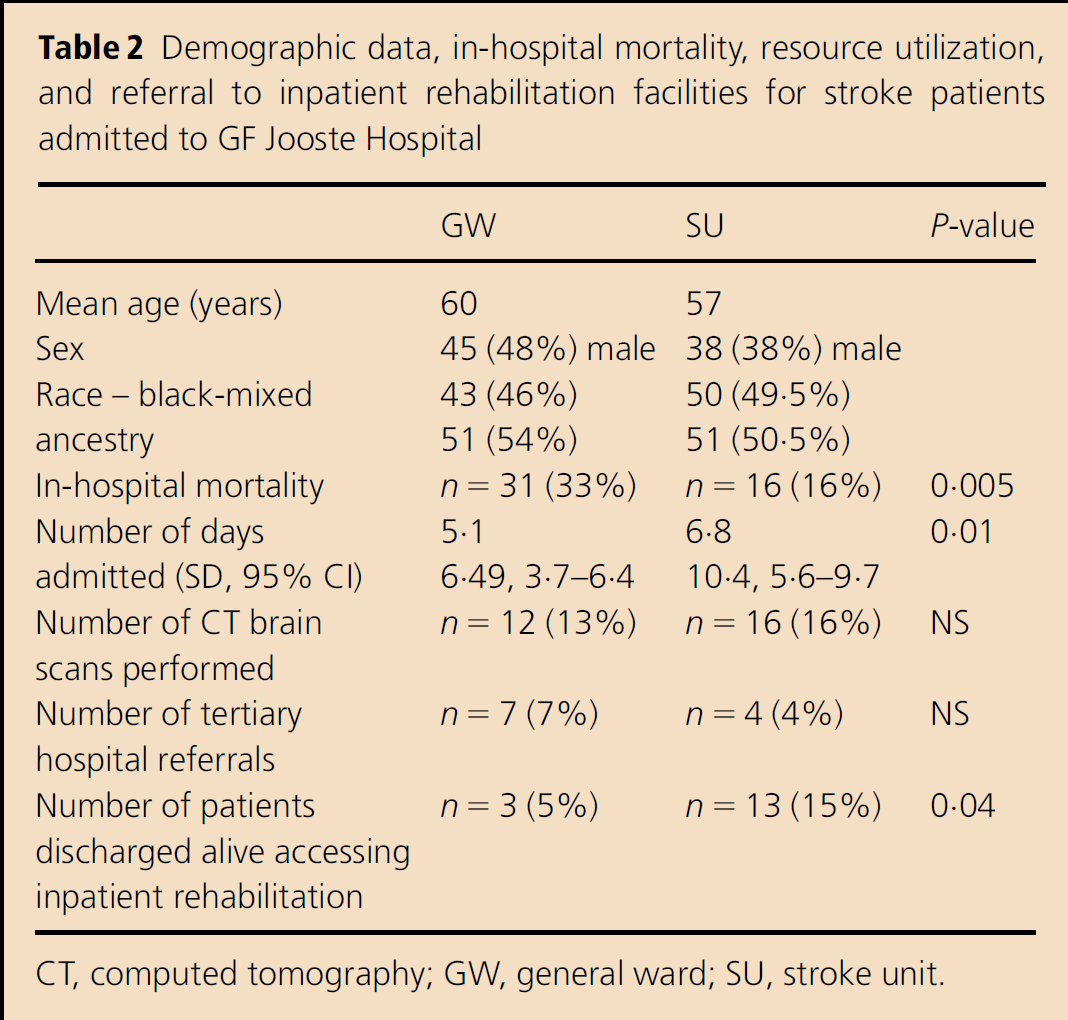
CT, computed tomography; GW, general ward; SU, stroke unit.
Outcome variables
The outcome variables measured included the length of hospital stay in days, inpatient death, transfer to a tertiary hospital, and the number of patients who had a CT brain scan performed. Inpatient mortality served as an indicator of the overall quality of inpatient care, while the length of hospital stay, number of referrals to a tertiary hospital, and the number of CT brain scans performed served as indicators of resource utilization. CT brain scans necessitated transfer by ambulance to a tertiary hospital, thereby substantially increasing the inpatient cost per admission. Patients requiring referral to a tertiary hospital for specialized management or inpatient investigations not available at GF Jooste Hospital had a prolonged hospital stay.
GW treatment
Stroke patients admitted to the GW before opening the SU were managed by medical officers under the supervision of a specialist. There were no guidelines outlining the care of and rehabilitation assessment and referral of stroke patients. Three physiotherapists, and two social workers employed at the hospital only saw stroke patients if referred by the medical staff.
SU treatment
A six-bed annex of an existing GW was allocated as the SU and a staff grade nurse, already employed in the GW, was appointed coordinator of the SU. She was assisted by the medical staff admitting stroke patients from the EU. A simple nine-page set of treatment guidelines based on the South African Medical Association Stroke Guidelines was formulated for use in the SU (25, 27). The guidelines outlined the assessment and stabilization of stroke patients by nursing and medical staff in the EU, admission criteria to the SU, and the investigation and general management of patients in the SU, including the identification and management of complications by both nursing and medical staff. Twice-weekly multidisciplinary SU rounds, led by a geriatrician, were attended by the SU nurse, the admitting medical officers, a physiotherapist, and a social worker. There was no formal training in the use of the SU guidelines, but adherence to the guidelines was stressed and reviewed on the SU rounds. The families of admitted patients were asked to attend the SU rounds so as to participate in the planning of secondary prevention, home-based care, and rehabilitation. Families were also encouraged to assist with in-hospital care, including nursing and rehabilitation therapy, so as to alleviate the burden on the nursing staff and become adept at caring for a stroke patient.
Statistical analysis
All data were entered into an Excel spreadsheet and descriptive statistics were obtained using Statistica Version 6 (Statsoft Inc., Tulsa, OK, USA). Continuous variables were compared using the Student t-test and categorical variables were compared using the χ2-test. A P-value of 0·05 or less was considered significant.
Results
Differences in the management of stroke patients in the SU, as compared with the GW, are outlined in Table 1 . Multidisciplinary stroke care resulted in standardization of investigation and initiation of secondary prevention, implementation of standardized measures to prevent and treat acute in-hospital complications, evaluation by a multidisciplinary rehabilitation team, staff education, standardized planning of discharge and rehabilitation, and involvement of the relatives in all aspects of the patient's care.
Differences in the care of stroke patients in the GWs as compared with the SU
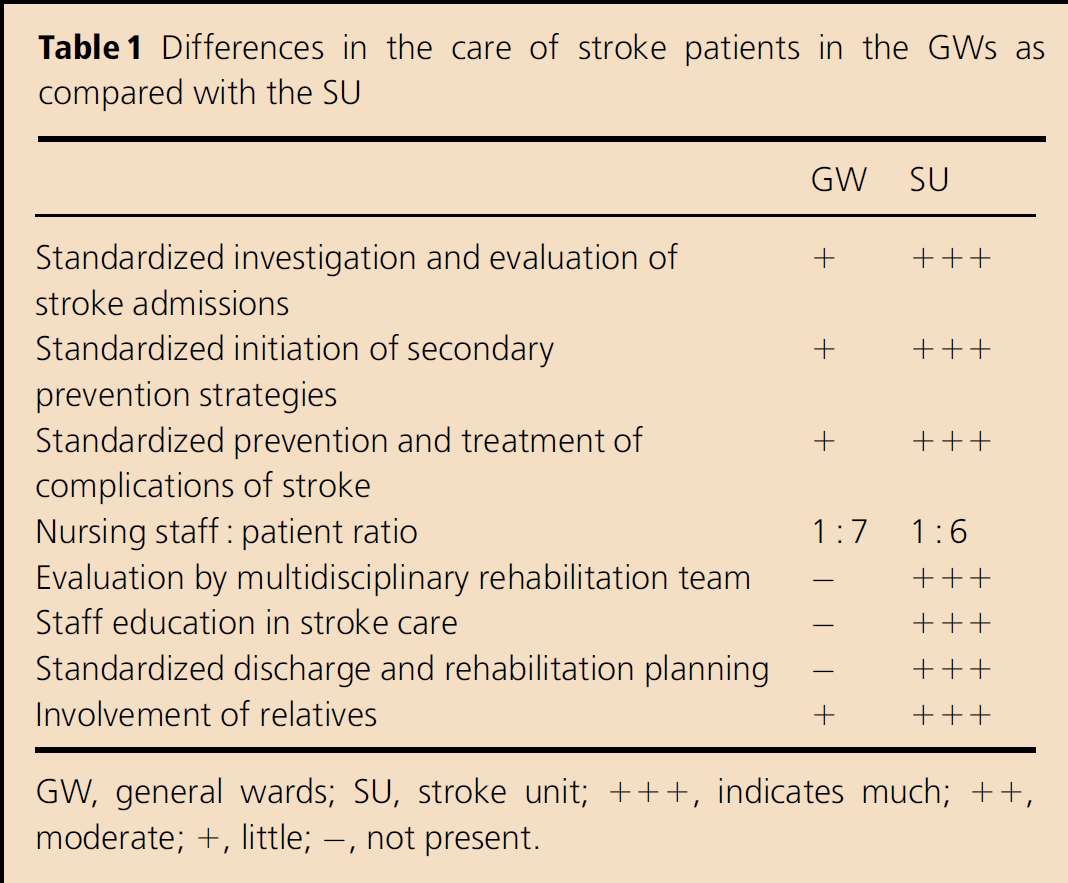
GW, general wards; SU, stroke unit; + + +, indicates much; + +, moderate; +, little; -, not present.
A total of 195 patients were studied, of whom 94 were admitted before initiating the SU and 101 thereafter. The demographic profiles of both the groups were similar. The mean (SD, 95% CI) age of admitted patients was 58·8 (14·5, 56·7-60·9); 60% were female and 46% were black Africans. The remainder were of varied ancestry.
The inpatient mortality in the group before the inception of the SU was 33% (n = 31) and it was 16% (n = 16) (P = 0·005) in the group studied after initiating multidisciplinary stroke care.
The mean length of hospital stay before establishing the SU was 5·1 (6·5,3·8–6·4) days as compared with 6·8 (4·5, 5·9–7·6) days after initiating multidisciplinary stroke care (P = 0·01). Referral of those who were alive at discharge to inpatient rehabilitation increased from 5% (n = 3) to 19% (n = 13) (P = 0·04). The number of CT brain scans performed 13% (n = 12) vs. 16% (n = 16) and the number of referrals to the tertiary academic hospital 7% (n = 7) vs. 4% (n = 4) did not change significantly.
Discussion
This study provides evidence that multidisciplinary stroke care can be successfully implemented in a limited resource setting in a developing country in Africa. Secondly, the data suggest that there may be benefit in reduced in-hospital mortality and improved access to inpatient rehabilitation facilities. The study, however, has several limitations. Although the mortality benefit was statistically significant, the short duration of observation and study design requires that these results be interpreted with caution. In order for an observational study of the impact of SU care to be interpreted with confidence, there should be adequate matching of baseline characteristics (stroke type and severity) between the two groups being compared in order to allow for case-mix adjustment during analysis of the data (9, 28). Unfortunately, this was not possible due to limited CT scan facilities (stroke-type) and limited data capture (stroke severity) when the SU first opened. Despite these limitations, the study is important as it shows that improved stroke care can be achieved despite:
limited resources,
no additional funding, or
additional staff.
The most important factor in establishing an SU was a commitment from the nursing staff and the support of nursing management: firstly, to care for the stroke patients in one defined geographical area within the hospital and then to act as the co-ordinators of the multidisciplinary team, and liaise with the family. Provision of standardized assessment and care, including secondary prevention, by both junior medical officers and nursing staff was achieved by the introduction of a set of clinical management guidelines and regular review of adherence to those guidelines on multidisciplinary stroke rounds. In order to improve adherence to these guidelines, they were kept short and very simple. Each area of management such as EU triage and stabilization; EU medical assessment; criteria for admission and CT head scanning; inpatient management and investigation and general nursing and coordinating nurses' function was limited to a single A4 page of information. Posters of these guidelines were placed in the appropriate areas and both medical and SU nursing staff were issued with pocket-size copies of the complete set of guidelines. Furthermore, the active involvement of relatives in the inpatient care of stroke admissions alleviated the nursing workload and provided an opportunity to train families to take care of patients without having to allocate staff time to dedicated family training sessions.
The possible reduction in in-hospital mortality demonstrated in this study is of critical importance. A study in Brazil, a developing country similar to South Africa, did not demonstrate a mortality benefit (15). Although our study did not determine the cause of in-hospital death, published data suggest that the mortality benefit observed in developed world SU may be attributed to a reduction in poststroke complications (29, 30). It is likely that the improved early mortality, within 7 days of admission, in our SU is largely due to better attention to the prevention of early complications of stroke such as aspiration, dehydration, deep venous thrombosis, drip site sepsis, and urinary tract infections in catheterized patients. This can mostly be attributed to guideline-driven care and dedicated nursing staff, who are responsible for monitoring glycemic control, treatment of fever, swallow assessments and feeding, early mobilization, limiting the use of intravenous lines, pressure care, and regular urine checks.
The cost of organized stroke care in SU has been shown to be no more expensive than GW care (10–12, 30). The cost of care in an SU is predominantly determined by the length of hospital stay (31–34). As no additional staff were employed to run our SU and the use of CT brain scan facilities and tertiary hospital referrals were not significantly increased, it can be concluded that the difference in cost of care was largely determined by the length of hospital stay. As the length of stay in our SU was significantly longer than that of the GW, we recognize that admission to the SU incurred a greater cost per patient than management in the GW. Cost of care and access to health care are of critical importance in sub-Saharan Africa, and further cost analysis is warranted to determine whether the improved mortality outcome demonstrated justifies the extra cost incurred.
In summary, we have demonstrated the successful implementation of multidisciplinary stroke care using minimal additional resources in an urban secondary hospital in South Africa. In this study, the data suggest that multidisciplinary stroke care resulted in a reduction in in-hospital mortality and improved access to inpatient rehabilitation facilities. The lengthened hospital stay implies greater admission cost per patient. This requires further study.