
Abstract
Objective
The occurrence of atrial fibrillation after percutaneous closure of a patent foramen ovale for cryptogenic stroke has been reported in a variable percentage of patients. However, its precise incidence and mechanism are presently unclear and remain to be elucidated.
Design
Prospective follow-up study.
Patients
Ninety-two patients undergoing a percutaneous patent foramen ovale closure procedure (closure group) for cryptogenic stroke were compared with a similar group of 51 patients, who were medically treated.
Methods
A systematic arrhythmia follow-up protocol to assess the incidence of AF was performed including a 7-day event-loop recording at day 1, after 6 and 12 months in patients of the closure group and compared with those of the medically treated group.
Results
The incidence of AF was similar in both study groups during a follow-up of 12 months, including 7·6% (95% CI: 3·1–15·0%) in the closure and 7·8% (95% CI: 2·18–18·9%) in the medically treated group (P = 1·0). The presence of a large patent foramen ovale was the only significant risk factor for the occurrence of AF as demonstrated by a multivariate Cox regression analysis (95% CI, 1·275–20·018; P = 0·021).
Conclusions
Our findings indicate that patients with cryptogenic stroke and patent foramen ovale have a rather high incidence of AF during a follow-up of 12 months. Atrial fibrillation occurred with a similar frequency whether the patent foramen ovale/atrial septal defect was successfully percutaneously closed or was medically managed. The presence of a large patent foramen ovale was the only significant predictor of AF occurrence during follow-up.
Introduction
Paradoxical embolism through a patent foramen ovale (PFO) is a plausible cause of cryptogenic stroke, particularly in a young patient population without cardiovascular risk factors (CVRF) (1). In this context, the percutaneous PFO closure has recently emerged as a safe and promising preventive therapy of this pathology, despite the fact that strong evidence suggesting its superiority compared with the best medical treatment, is still lacking (2,–5). Although, with the currently available technologies and devices, the procedural success rate is very high with a very low complication rate, stroke recurrences in the follow-up (FU) may occur (6, 7). It remains unclear whether these recurrent strokes may be device-related (e.g. thrombus attached on the device), due to a device failure (e.g. persistent significant right to left shunt) or finally be associated with another misdiagnosed cardiac disease, particularly paroxysmal atrial fibrillation (AF). In this sense, several reports have suggested a variable and sometimes high incidence of this arrhythmia during the FU of patients treated medically (8, 9) or patients treated with a PFO closure device (6, 10).
The present study was undertaken to assess the incidence of AF during FU and to better understand its triggering mechanisms by performing prospectively an arrhythmia FU-protocol and a systematic clinical FU to all patients with cryptogenic stroke and proven PFO, who underwent a successful percutaneous PFO closure. In addition, we compared the observed results with those of a group of patients with similar characteristics and who did not undergo the closure procedure, but were medically treated.
Methods
Study population
All patients presenting with a cryptogenic ischaemic event (cerebral stroke or peripheral ischaemic event) or transient ischaemic cerebral attacks (TIA) in whom a paradoxical embolisation via a PFO or a small atrial septal defect was retained as the most plausible aetiology of the ischaemic event, were discussed in a multidisciplinary meeting including a neurologist, a cardiologist, an angiologist, and a neuroradiologist. Before the PFO closure, a complete cardiologic examination, including an arrhythmia rule-out protocol, a transthoracic (TTE) and transoesophageal echocardiographic study (TEE) was performed associated to neurologic (carotid and transcranial Doppler (TCD) with micro-bubbles' detection) and haematologic investigations (thrombophilia screening).
Our systematic arrhythmia rule-out protocol was performed according to previously validated protocols established by our group, including in all patients a standard 12-lead ECG at hospital admission, an in-hospital 24-h 3-channel ECG recording (Holter) (Avia, Del Mar Reynolds Medical Systems, Irvine, CA, USA) and an ambulatory 7-day event-loop-recording (R-test evolution, 3rd generation: Novacor Enterprise, Physicor, Geneva, Switzerland) (11). In the absence of any potentially thrombo-embolic arrhythmias or other causes explaining the ischaemic event, the PFO/ASD closure procedure was then performed.
PFO anatomy and closure procedure
The respective PFO/ASD size was estimated according to the TTE/TEE/TCD results and was classified as: small PFO ≤ 20 micro-bubbles passages at rest or at Valsalva manoeuvre; moderate PFO = 20–50 micro-bubbles passages at rest or at Valsalva manoeuvre; large PFO ≥ 50 micro-bubbles passages at rest or at Valsalva manoeuvre (12). All ASD were considered as large PFO concerning the micro-bubbles passages, even if the micro-bubbles tests had not been systematically performed. The trans-catheter closure of the PFO with and without atrial septal aneurysm (ASA) was performed under local anaesthesia and fluoroscopy guidance; for the small ASD closure procedures a TEE or intra-cardiac echocardiographic support was also adopted. Once the PFO or the small ASD was crossed with an exchange guide wire, a sizing balloon (Amplatzer Sizing Balloon 24 mm or 34 mm in diameter, AGA Medical Corporation, Golden Valley, MN) was utilised to measure the size of the PFO/ASD, and finally the most suitable closure device was placed at the atrial septal level. According to the measured stretched PFO/ASD diameter, the best suitable closure device was implanted (13).
Study FU protocol
This protocol was approved by the local ethic committee and all patients gave written informed consent before the scheduled clinical and para-clinical FU examinations were performed. After the closure procedure, all patients received a dual antiplatelet therapy for 6 months and were systematically included in the following regular FU protocol: on day 1, a TTE was performed to assure a good device anchoring and to have an initial imaging of the device, followed by a 7-day ELR; at 1 month, a second TTE and a TEE were performed; after 6 and 12 months, a complete cardiologic and neurologic clinical evaluation was performed, including TTE, TEE, TCD and a 7-day ELR. The 12-month TEE examinations were not routinely performed in all patients, but only on clinical basis and according to the results of the scheduled 6-month FU control.
7-day ELR
The 7-day ELR was performed using automatic and manual (possibility for the patient to press on the recording key in case of symptoms) recordings and was programmed to store irregular RR-interval strips that could correspond to AF paroxysms. Parameters for event-triggered recording were as follows: 50 s (s) for absolute pauses (RR interval > 2·5 s); 175 s for relative pauses (RR interval > 150% previous RR interval); 500 s for premature beats [RR interval < (mean RR–12·5% x mean RR)]; 60s for bradycardia (R frequency<50 b.p.m.); 250 s for runs [RR interval < (RR–12·5% x RR) for >3 beats]; 120 s were devoted to patient-triggered recording (11). Atrial fibrillation was identified by manual reviewing of the ECG recordings.
Medically treated group
The medically treated group consisted in patients who presented with cryptogenic stroke or TIA during the same time period (year 2002–2006) and who did not undergo the PFO closure procedure for several reasons: (1) patient's refusal (N = 15), (2) other reasons to continue oral anticoagulation (N = 8) (e.g. thrombophilia), (3) small TIA with small PFO without high-risk characteristics (N = 11), and (4) patients with stroke presenting several CVRF and small PFO (N = 17). These patients, according to their clinical characteristics, were discharged from the hospital with an antiplatelet regimen (aspirin or clopidogrel) or oral anticoagulation.
All patients of the closure and the medically treated group study underwent the same arrhythmia screening protocol before and during FU.
Statistical analysis
Data are expressed as means ± standard deviation (SD) or as means and range for continuous variables and as numbers of patients and percentages for categorical variables. Statistical comparisons between continuous observations were made with unpaired Student's t-test. Fisher's exact test was used for categorical variables. The odds ratio for the occurrence of AF during FU in the study patients was determined among the following variables: male gender, age > 50 years, presence of arterial hypertension, presence of a large PFO and of ASA. A P value <0·05 was regarded as statistically significant. Cox regression analysis was used to identify independent predictors of AF during FU. Age, gender, presence of hypertension, of a large FOP and an ASA were introduced into the model. Calculations were performed with SPSS for Windows (Version 15·0, SPSS, Chicago, IL).
Results
Patient characteristics
Table 1 depicts the clinical characteristics of the patients of the closure group retrospectively compared with those of the medically treated group. A total of 92 patients presenting with a cryptogenic ischaemic event were included in the closure group and retrospectively compared with 51 patients of the medically treated group. The mean FU period was of 12·1 months (range 1–48 months). As shown in Table 1, patients' characteristics were similar in both groups except for arterial hypertension which was significantly more present in the medically treated group (P = 0·0054). In both groups no AF paroxysms were clinically suspected or detected at baseline. The indication for the initial closure procedure for the 92 patients in the closure group was the first episode of cerebral stroke/TIA in 63 patients (68·5%), recurrent stroke/TIA episodes in 24 (26·1%) and a peripheral ischaemic cryptogenic event in three patients (3·2%), including one in the finger, one in the small intestine and one in the eye. One additional patient had a scuba diving accident and another one a symptomatic platypnea–orthodeoxia with recurrent strokes. Before PFO/ASD closure most study patients (95·6%) were receiving either anticoagulation or antiplatelet regimen: 50 patients (55·5%) were treated with oral anticoagulation; 20 (22·2%) with either aspirin or clopidogrel; 13 (14·4%) with both aspirin and clopidogrel and 3 patients (3·3%) received low-molecular-weight heparin.
Clinical characteristics of the patients of the closure group compared (retrospectively) with those of the medically treated group
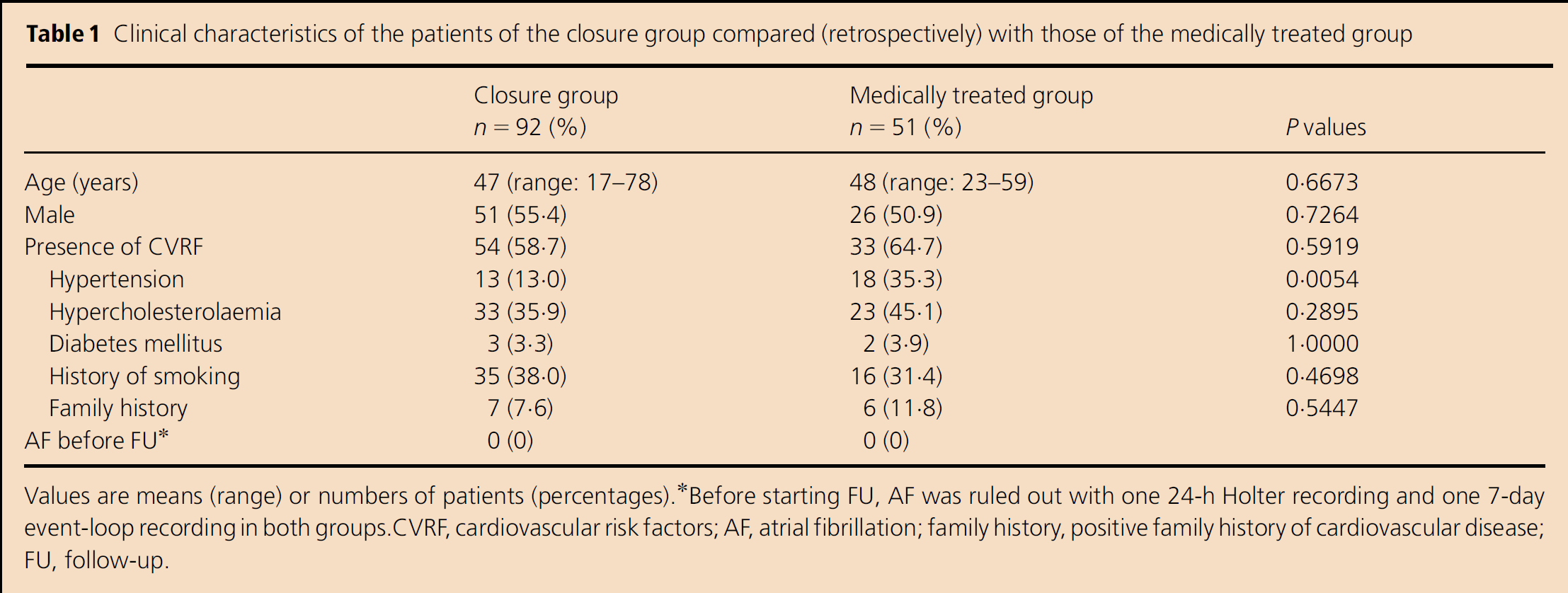
Values are means (range) or numbers of patients (percentages).
Before starting FU, AF was ruled out with one 24-h Holter recording and one 7-day event-loop recording in both groups. CVRF, cardiovascular risk factors; AF, atrial fibrillation; family history, positive family history of cardiovascular disease; FU, follow-up.
Echocardiographic data
Table 2 shows echocardiographic data in patients of the closure group retrospectively compared with those of the medically treated group. Left atrial size was similar in both groups. Small PFOs were more frequently present in the medically treated group (P < 0·0001), while PFOs of large size were more often found in the closure group (P = 0·0080). No significant differences were observed between groups for the presence of PFOs of moderate size (P = 0·1347). Associated ASAs were more frequently seen in the closure group (P = 0·0016). All included ASDs had no haemodynamic repercussion, and thus were considered as the most plausible source for the paradoxical embolism leading to the cryptogenic stroke. In both groups, left and right ventricular size and function were normal and there were no significant valvulopathies.
Echocardiographic characteristics of the patients of the closure group compared (retrospectively) with those of the medically treated group
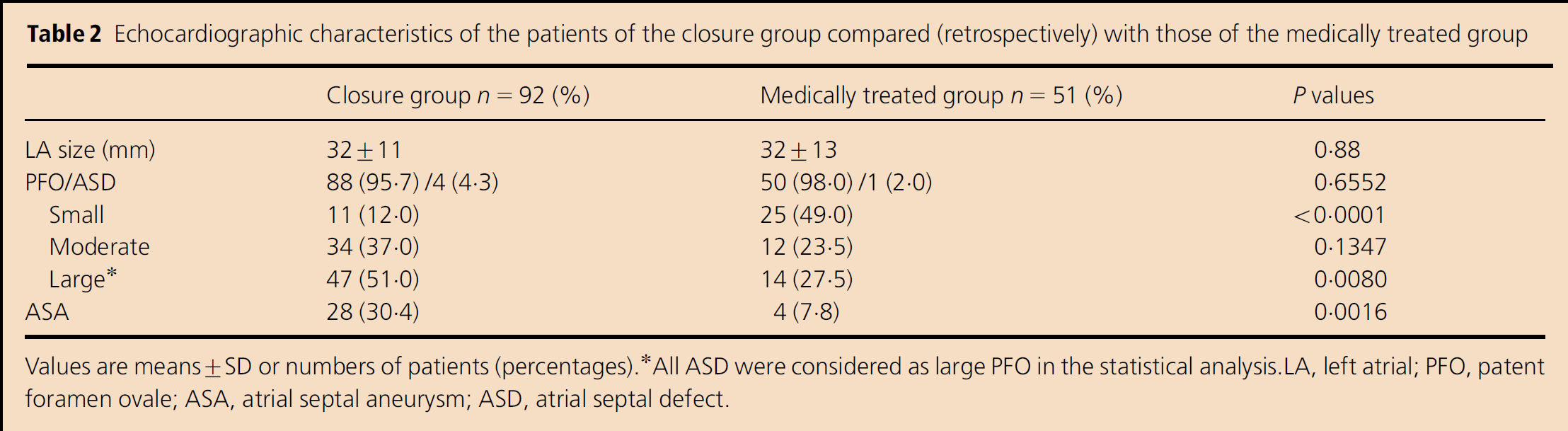
Values are means ± SD or numbers of patients (percentages).
AII ASD were considered as large PFO in the statistical analysis. LA, left atrial; PFO, patent foramen ovale; ASA, atrial septal aneurysm; ASD, atrial septal defect.
Incidence of AF
As shown in Table 3, the incidence of AF was similar in both study groups during FU, including 7·6% (95% CI: 3·1–15·0%) in the closure and 7·8% (95% CI: 2·18–18·9%) in the medically treated group (P = 1·0). In the closure group, a total of 7 (7·6%) patients presented nine different episodes of AF. Five patients had a PFO associated with an ASA; two had a moderate PFO and the remaining five a large one. All used devices were Amplatzer PFO or ASD Occluders™ (AGA medical Corp.) and one was a PFO-Star device™ (Cardia, Burnsville, MN).
Characteristics of patients in both groups with AF occurrence during follow-up
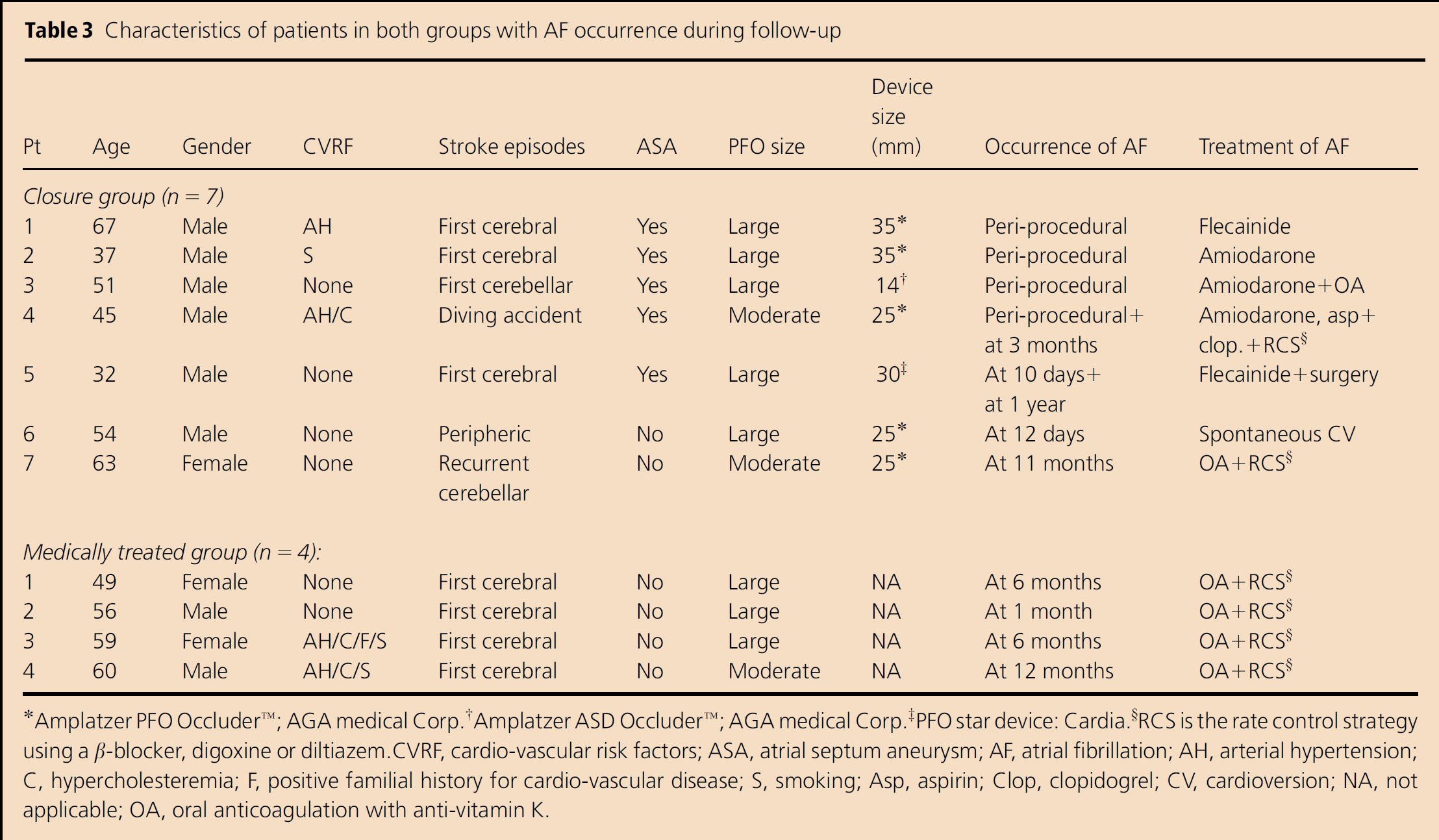
Amplatzer PFO Occluder™; AGA medical Corp.
Amplatzer ASD Occluder™; AGA medical Corp.
PFO star device: Cardia.
RCS is the rate control strategy using a β-blocker, digoxine or diltiazem.CVRF, cardio-vascular risk factors; ASA, atrial septum aneurysm; AF, atrial fibrillation; AH, arterial hypertension; C, hypercholesteremia; F, positive familial history for cardio-vascular disease; S, smoking; Asp, aspirin; Clop, clopidogrel; CV, cardioversion; NA, not applicable; OA, oral anticoagulation with anti-vitamin K.
Six of the nine episodes of AF occurred in the early FU (i.e. < 1 month), the rest in the late FU (i.e. 1–12 months). Four of these early episodes were observed during the PFO closure procedure or in the hours immediately thereafter (Patients 1–4). These very early AF episodes could have been secondary to procedural related mechanical factors. However, they persisted for at least 24 h up to 1 week and difficultly could be explained only by the instrumental atrial irritation occurred during the closure procedure. All these AF episodes were described by the patients as an uncomfortable palpitation; all episodes were associated with a rapid ventricular response and they all necessitated the use of intravenous antiarrhythmics (e.g. amiodarone or flecainide). The other two early AF episodes were observed in the first 2 weeks after the procedure (Patients 5 and 6). Patient 5 required intravenous flecainide for successful conversion and Patient 6 spontaneously converted into sinus rhythm few days after the AF onset.
The remaining three episodes of AF were detected at later terms (Patients 4, 5 and 7). Two of these episodes were asymptomatic and one was symptomatic. All of the episodes of late AF were paroxysmal (i.e. < 24 h) and all were confirmed by ECG or by 7-day ELR. Of interest, two of these late AF episodes occurred in patients who had already experienced an early AF (Patients 4 and 5). Patient 5 presented, 1 year after the PFO-Star device implantation, AF recurrence, acute dyspnoea, syncope and cardiac tamponade secondary to a device's strut protrusion through the left atrial roof into the aortic wall (14). Patients 4 and 7 were both refractory to the attempted antiarrhythmic regimen, therefore, a rate control strategy was adopted and an oral anticoagulation was associated to the dual antiplatelet regimen. However, oral anticoagulation was refused by Patient 4 (the scuba diving patient), who therefore remained on long-term aspirin and clopidogrel regimen. In the medically treated group, four (7·8%) patients presented at least one AF episode during the FU period. In these four patients, it was decided not to close the PFO, because Patient 1 refused the procedure; Patient 2 had an associated thrombophilia necessitating long-term anticoagulation and Patients 3 and 4 had a relatively low-risk PFO. All four patients presented paroxysmal AF episodes during FU after hospital discharge. Three patients were symptomatic (i.e. palpitation), one was asymptomatic. All were treated with long-term oral anticoagulation and a rate control strategy.
Maybe thanks to an early AF detection, none of the patients in both groups experienced a recurrent ischaemic event secondary to the new onset AF.
Risk factors for the occurrence of AF during FU
Firstly, we performed an univariate analysis of the most important potential risk factors for the occurrence of AF during FU in patients with cryptogenic stroke and PFO: male gender, age > 50 years, presence of arterial hypertension, presence of a large PFO and of ASA.
The presence of a large PFO (odds ratio: 3·975, 95% CI, 1·008–15·68; P = 0·0545) and of an ASA (odds ratio: 3·241 (95% CI, 0·9190–11·43; P = 0·0689) were the only two nearly statistically significant factors in this univariate analysis. Secondly, we performed a multivariate Cox regression analysis of the same five elements (age as continuous variable), to better elucidate the clinical relevance especially of large PFOs and ASA, and this time the Cox analysis confirmed that only the presence of a large PFO was a statistically significant predictor of AF (relative risk = 5·051, 95% CI, 1·275–20·018; P = 0·021) (Table 4).
Risk factors for the occurrence of AF during follow-up (multivariate analysis)
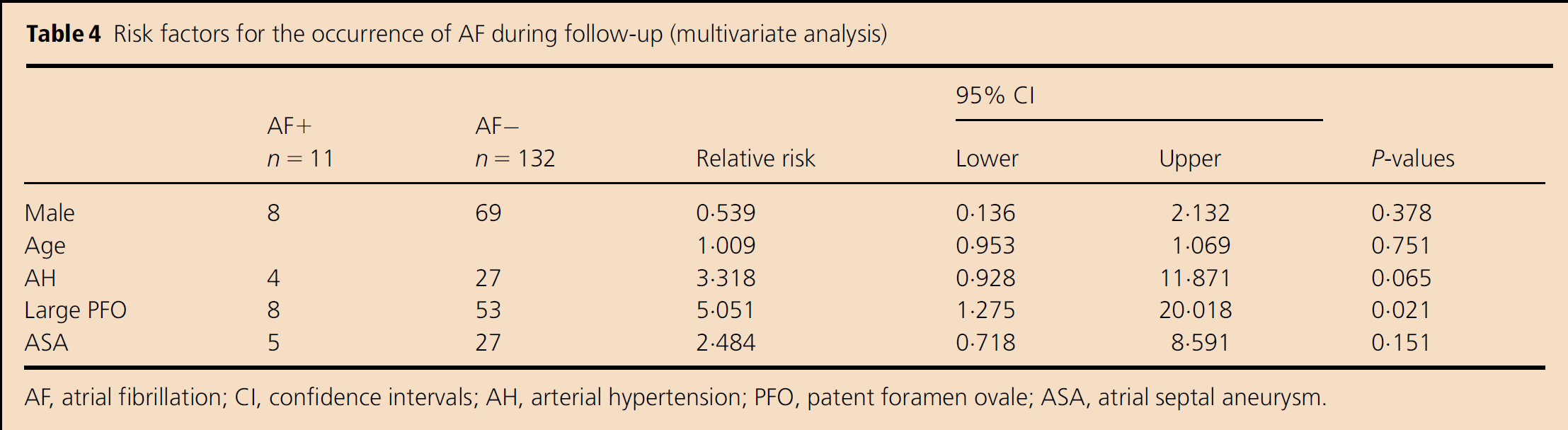
AF, atrial fibrillation; CI, confidence intervals; AH, arterial hypertension; PFO, patent foramen ovale; ASA, atrial septal aneurysm.
Discussion
Our findings indicate that patients presenting with cryptogenic stroke due to the presence of a PFO/ASD may have underlying associated episodes of paroxysmal AF. The incidence of AF was similar in the closure and in the medically treated group, thus suggesting that closure procedure and PFO devices are not significantly implicated in AF development, nor do they reduce its occurrence. The presence of a large PFO was the only significant risk factor for the occurrence of AF during FU.
Comparison with previous studies
A variable incidence of paroxysmal AF has been reported in patients with cryptogenic stroke after PFO closure, most often ranging between 2 and 3% (4, 5, 15). However, similar to our data, Anzola et al. (16). and Krumsdorf et al. (7) have found AF in up to 8% of their patients after the PFO closure and in the Burow et al. (17) patients' cohort, AF was even highly observed (up to 15%) in the 1-year FU. The reasons for these differences in AF incidence are not clear, but probably due to the fact that, in some of these studies, this arrhythmia was not systematically sought by strict preoperative AF rule-out protocols, a pre-existing underlying AF could have been misdiagnosed and thus discovered only in the FU once the PFO was already closed. In our study, despite the pre-operatively meticulous arrhythmia rule-out protocol, AF may still not have been sufficiently revealed by the adopted current technologies, suggesting that further improvements in AF detection algorithms should be made in all cryptogenic stroke patients, especially in those scheduled for a PFO-closure.
Potential mechanisms of AF
An underlying atrial vulnerability hypothesis, as already suggested by Berthet et al. (18) and Rouesnel et al. (19), is one of these possible AF-triggering mechanisms. In fact, these studies concluded that patients presenting an atrial septal abnormality (i.e. ASA, PFO or ASD) have an increased atrial vulnerability during electrophysiological studies. This hypothesis is corroborated by the fact that during the procedure itself, the right/left atrium and the pulmonary veins instrumentation with guide-wires and other utilised material (e.g. catheters, delivery sheath) may often unmask some underlying and misdiagnosed pre-existing atrial arrhythmias.
Another potential AF mechanism lies in a device-related atrial irritation hypothesis, which suggests that PFO closure devices, especially the large ones, may be the triggering mechanism for the development of newly diagnosed AF. This hypothesis was recently suggested by Alaeddini et al. (20) who found that larger PFO devices were more frequently associated with the development of supra-ventricular arrhythmias in the FU of patients who underwent a successful PFO closure procedure. However, our and other similar data (17) do not support this irritation hypothesis, especially if one considers the finding that AF also occurred in our and other medically treated cryptogenic groups of patients (8, 9, 21, 22).
Risk factors for the occurrence of AF
According to the echocardiographic data, the closure group presented a higher risk PFO anatomy compared with patients of the medically treated group, especially if one considers the higher incidence of associated ASA (30·4% vs. 7·8%; P = 0·0016). However, only the presence of a large PFO size appeared to be a significant risk factor for the AF occurrence (P = 0·021). In this sense, even if our data are based on a small patients' collective (N = 11 patients with AF), they corroborate the possibility that patients with PFO, and particularly those with larger PFOs, may be predisposed to future AF development. Even if not formerly confirmed by larger PFO trials, these findings are in line with what recently suggested by other reports (8, 9, 18, 19, 21, 22).
Clinical implications
Taking into account that cryptogenic stroke represents almost 25% of all strokes and that approximately half of these strokes may be secondary to a paradoxical embolism through a PFO, strict AF rule-out protocols using 24-h Holter recordings and ambulatory 7-day ELRs should be largely used (11, 23), especially before the percutaneous PFO closure and according to our data particularly in patients with large PFOs. These rule-out protocols should be performed in order to better detect silent AF episodes, thus probably avoiding unnecessary PFO closure procedures.
Study limitations
Because this study was not randomised, differences between the closure and the medically treated group could exist and be related to the initial patients' selection criteria. Owing to the retrospective nature of this comparison, the obtained AF incidence in the analysed groups should therefore be interpreted with caution. However, even if, unmeasured clinical factors in subjects treated medically might have predisposed them to develop AF, whereas device placement could have increased the risk in those having PFO closure, only the prevalence of arterial hypertension was statistically higher in the medically treated group. No significant echocardiographic differences for left atrial or ventricular size and function were noted between the two groups.
Finally, it should also be pointed out that patients with cryptogenic stroke and a high-risk PFO anatomy can difficultly nowadays be randomised into a medically treated group because in this situation the PFO closure seems clearly indicated.
Conclusion
Our findings indicate a rather high incidence of AF during a 12-month FU of patients with cryptogenic stroke presenting with PFO/ASD. Atrial fibrillation occurred with a similar frequency in case the PFO/ASD was successfully percutaneously closed or was medically managed. The presence of a large PFO was the only significant risk factor for the occurrence of AF during FU in both groups.