
Abstract
Background/Purpose
The aim of our study is to evaluate the frequency of aphasia and to describe the characteristics of aphasics among a large sample of acute stroke patients in Italy.
Methods
Out of the 11 572 stroke patients hospitalised within 48 h from stroke onset, included in the PROSIT study, we selected 9594 alert cases for the estimation of aphasia frequency. The presence of aphasia was accepted when registered in the clinical records at the first neurological examination. All patients/caregivers underwent to a 2-year telephone follow-up evaluation.
Results
Twenty-eight per cent of alert acute stroke patients had aphasia, which was associated with arm and/or limb weakness in 74% of cases. In our series, aphasia was more frequent in females than males, in patients older than 75 years and was associated with more severe stroke. Aphasics, compared with nonaphasics, died more frequently. Aphasia was also significantly associated with residual poststroke disability.
Conclusions
This is the first study considering the frequency of aphasia in a wide population of hospitalised acute stroke patients. The presence of aphasia is more common in patients with severe stroke and contributes to residual disability. Our findings should be considered for setting early specific rehabilitation programmes.
Introduction
Aphasia is a frequent presenting symptom of acute stroke (1,–8). The sudden onset of this communication impairment is very distressing for patients and their family and, in many cases, impairs good hospital care and management. However, so far, few studies evaluated the incidence and the burden of aphasia in hospitalised acute stroke patients. Some studies conducted many years ago used heterogeneous methodological approaches (1,–3); others were designed to define subtypes of aphasic disorder among small series of stroke patients (1, 3, 4,–8). A population-based study, conducted in 2006, found an incidence of aphasia from first ischaemic stroke of 43 for 100 000 inhabitants (9).
Thus, considering the large number of patients developing a sudden speech impairment, adequate acute and sub-acute rehabilitation programmes are required.
In the present study, we aim to evaluate the incidence of aphasia among a large cohort of hospitalised acute stroke patients. Our purpose is also to assess extent of concomitant impairments and comorbidities and to study the association between the presence of aphasia and the short- and long-term outcome.
Patients and methods
We considered 9594 conscious patients out of the 11 572 acute strokes included in the PROSIT study. PROSIT (Research PROject on acute Stroke patient care in Italy) was a study aimed at evaluating, quality and benefit of acute stroke care in seven Italian regions (Friuli-Venezia Giulia, Lombardia, Veneto, Liguria, Emilia-Romagna, Toscana, Lazio) which have a population of 29 169 811 inhabitants and a 225/100 000 hospitalisation rate for acute stroke (10, 11). The study included a sample of stroke patients hospitalised within 48 h during 2001, of whom 43% were treated in dedicated Stroke Units (SUs). We included all the SU cases admitted during the last 9 months of 2001 in the 31 SUs identified previously. The controls were a sample selected following a computer-generated random numbers list stratified by regions, representative of about 20% of cases admitted in the 393 conventional wards during the same period.
The patients' demographic and clinical characteristics were obtained by consulting the hospital clinical records. The presence of aphasia was confirmed by trained researcher neurologists, evaluating the first neurological examination as reported in the clinical records. The researcher neurologists identified aphasic patients by checking clinical records for the presence of impaired comprehension and/or paraphasias and/or word-finding difficulty in all alert cases. These researchers were trained to distinguish aphasia from dysarthria. The training process included the evaluation of a random sample of 20 clinical records from a pool of confirmed aphasic and nonaphasic patients from different hospitals before starting the study.
Information on death during hospitalisation and type of discharge (home or other, e.g. rehabilitation units or nursing house admission) was also obtained from the clinical records.
All patients were followed up after 2 years through a structured phone interview in which data on death, rehabilitation course either physical and/or language therapy, changes in living condition and Rankin scale score were registered. The full study methodology has been widely described in previous reports (11, 12).
For the present paper, factors like age, sex, side and severity of the strength motor impairment, stroke type (ischaemic or haemorrhagic at CT scan) and length of hospital stay (LOS) were selected from the initial pool of collected data. The detection of high blood pressure, atrial fibrillation and the positioning of the nose-gastric feeding tube during hospitalisation were also considered.
Statistical analysis
The data were checked for consistency and completeness. Statistical analyses to compare patients with and without aphasia were performed by means of the χ2-test for categorical data and Student's t-test for interval data; the statistical significance was set when the P value was <0·01. Multiple logistic regression analyses were performed to assess the association between aphasia and long-term outcome adjusting for age, sex, atrial fibrillation cerebral haemorrhage and severity of motor deficit. Odds ratio (OR) and the 95% confidence intervals for each outcomes were calculated (STATA 8·0).
Results
Out of 11 572 acute stroke patients considered initially, the language deficit was evaluated in 9594 conscious patients. Seven hundred and forty-six additional cases (8%), in whom the language condition was undeterminable, were excluded. We did not find any statistically significant difference in age, sex and other risk factors between the 8848 included and the 746 excluded cases, except for intracranial haemorrhage and atrial fibrillation, both of which were less frequent in the included group (11 vs. 14% P<0·0001 and 16 vs. 17% P<0·0001, respectively).
Out of the 8848 included cases, 6374 (72%) were nonaphasics and 2474 (28%) were aphasics. In 1843 (74%) aphasics, language disorder was associated with arm and/or limb weakness, which was in 1506 (82%) subjects on the right side, in 301 (16%) on the left side and in 29 (2%) bilateral. Age and gender distribution of aphasics is presented in Table 1.
The analysis of regional distribution revealed that the number of aphasic patients was higher in some (Friuli-Venezia Giulia, Emilia–Romagna and Liguria) of the seven Italian regions evaluated. Crude data on the regional frequency of aphasia are important to check local needs and to plan language rehabilitation at the regional level. However, after performing an age-population corrected analysis, we observed that the percentage of aphasic patients was similar in the different regions and did not differ from the global incidence (28% range 26·31–28·13).
Age and sex frequency of aphasia attributable to acute strokes
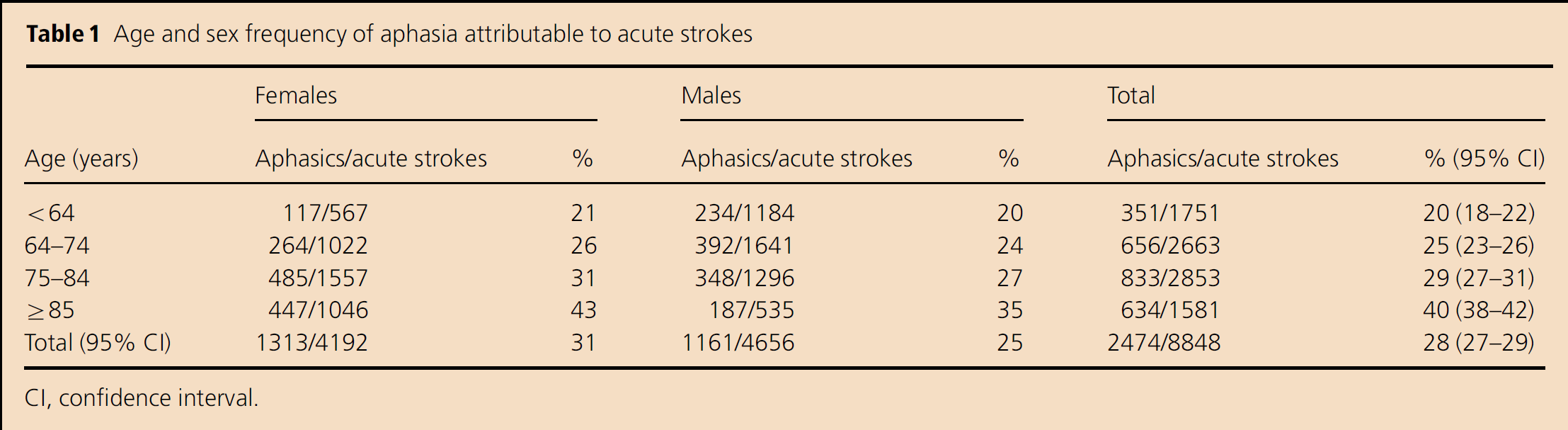
CI, confidence interval.
Compared with nonaphasic patients, aphasic patients seem to be more frequently females than males (53 vs. 47%). Age was also associated with the presence of aphasia, so that 59% of aphasic vs. 46% of nonaphasic patients were over 75 years old (P<0·0001). They had equal access to SU beds (43% of aphasic vs. 45% of nonaphasic patients had access to an SU). Aphasic patients had a more severe stroke than nonaphasics. In fact, the 25% of aphasics compared with 10% of nonaphasics (P<0·0001) had a severe motor deficit in arm and/or limb and a haemorrhagic lesion was detected at brain CT in 13% of aphasics' scan compared with 11% of nonaphasics (P<0·0001). Twenty-three per cent of aphasic patients vs. 13% of nonaphasics had an embolic source (atrial fibrillation) (P<0·0001), while the frequency of hypertension was similar in the two groups (29 vs. 27%; NS). The major severity of stroke in aphasic patients is confirmed by the more frequent use of nose-gastric feeding tube than in nonaphasic patients (10 vs. 3%; P<0·0001), longer LOS (73% of aphasic vs. 65% of nonaphasic patients (P<0·0001) have a LOS above 7 days) and higher in-hospital mortality rate (11% in aphasic patients compared with 4% in nonaphasic patients; P<0·0001) (Table 2).
Comparisons of acute stroke with and without aphasia for basal characteristics and outcome
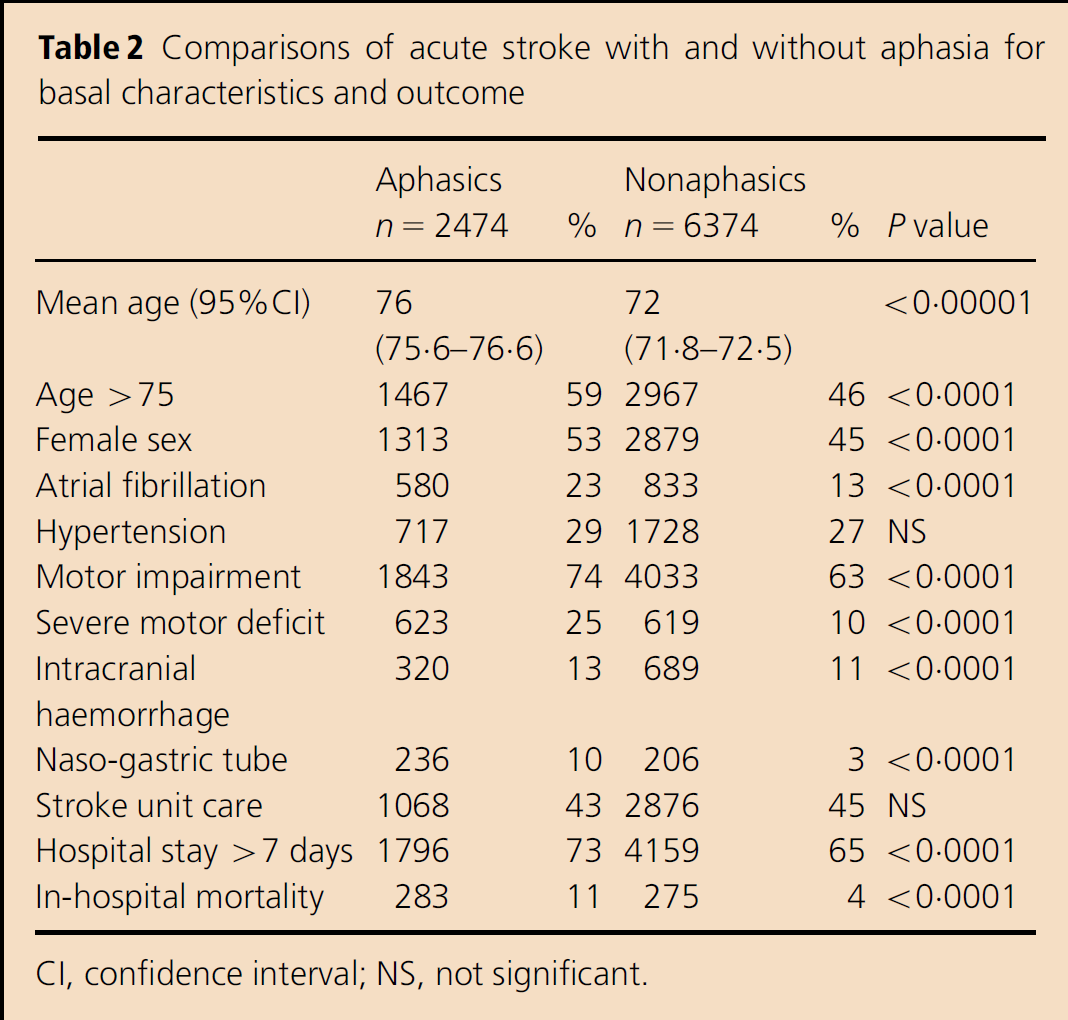
CI, confidence interval; NS, not significant.
The persistent long-term disability in aphasic patients is confirmed by the finding that aphasics live less frequently at home than nonaphasics (87 vs. 91%), even if with assistance, and also by the fact that aphasics have more frequently a Rankin scale score >2 than nonaphasics (61 vs. 48%). The aphasic patients needed more rehabilitation courses (37 vs. 29% of nonaphasics), performed both in outpatient departments and through specific hospitalisations in the rehabilitation department. The frequency of further hospitalisations for poststroke complications was the same in the two groups (24 vs. 23% in aphasics and nonaphasics). The multivariate analysis, corrected by age, sex, atrial fibrillation, cerebral haemorrhage and severity of motor deficit, confirmed that aphasia was a predictor of long-term mortality and disability in surviving cases (Table 3).
Long-term mortality and outcome in survived aphasic and nonaphasic strokes
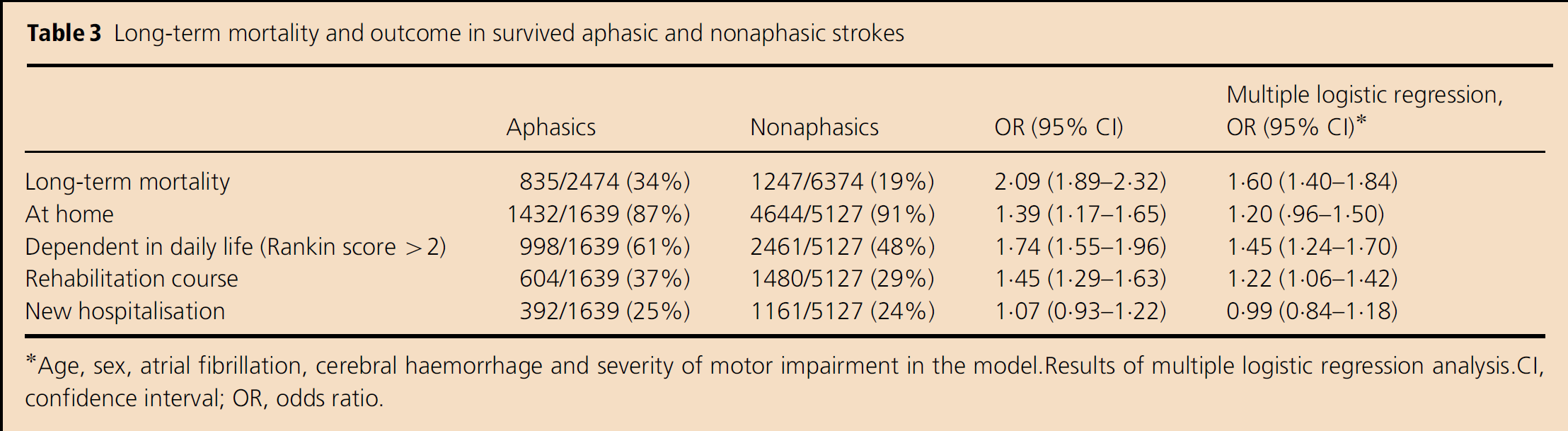
Age, sex, atrial fibrillation, cerebral haemorrhage and severity of motor impairment in the model. Results of multiple logistic regression analysis. CI, confidence interval; OR, odds ratio.
Discussion
According to previous reports, our findings support the evidence that aphasia represents a frequent impairment in acute stroke patients (Table 4). The incidence range from a lower value (15%) in a Japanese hospital-based study (8) to a higher value (37%) in a community-based study (6). A recent population-based study indicated aphasia in 30% of stroke patients, of whom 4% were nonhospitalised subjects (9) We obtained results very similar to this last study (9), reporting 28% aphasics from a large series of unselected acute stroke patients belonging to a random sample of an in-hospital population, largely distributed on Italian territory.
Incidence of aphasia in acute stroke
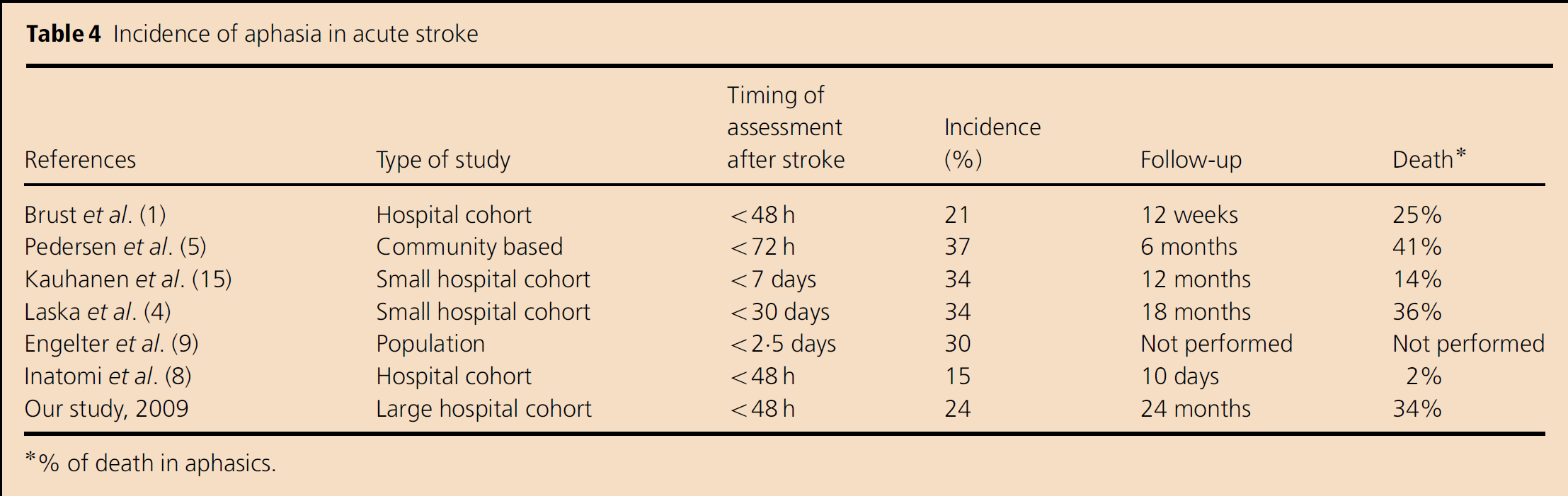
% of death in aphasics.
In comparison with previous reports, our study used less specific tests to assess aphasia. However, the diagnosis of aphasia was always confirmed by two groups of neurologists, the first one performing neurological evaluation during the hospitalisation and the second one retrieving neurological examination from the hospital clinical records. This methodology mostly reflects clinical practice, in which aphasia is clinically assessed during the stroke acute phase and specific tests confirm diagnosis or characterise aphasia subtype. Therefore, we expect that our study has better result validity (positive predictive value) than other studies such as the report of Thommessen et al. (13), in which the assessment of aphasia was performed by a nurse using the aphasia items of the Scandinavian Stroke Scale. However, the validity of our diagnostic approach has never been formally tested.
In our population, aphasia increased from 20% in patients aged <65 years to 40% among those older than 85 years. Females showed a higher risk of aphasia compared with males in any class of age. Aphasic patients were not only older but also had a higher frequency of severe motor impairment and cardiologic comorbidity than nonaphasics, as observed previously (8). At the end of about 2 years, 61% of surviving aphasic patients were dependent for everyday life activities.
The worst outcome of aphasic patients, which has already been reported in literature (1, 3, 4), seems to be independent from stroke subtypes (embolic/nonembolic) and motor severity at the multifactorial logistic regression analysis.
This severe clinical profile of aphasic patients, which is frequently associated with significant depression, could not only interfere with acute care and management but may also impair a good rehabilitation programme (14, 15). Although the benefit of speech therapy has been a matter of controversy for a long time (16,–18), recently it has been documented that acute (16, 17) and intensive speech therapy (19) has a significant effect on recovery of aphasic disorders. Acute-phase language rehabilitation could support spontaneus recovery due to the establishment of new functional pathways, before the compensatory strategies of chronic phase develop (20). A rehabilitation course in the chronic phase was feasible only in two-third of our patients, probably due to the presence of comorbidities and motor impairment. However, although the best model of speech therapy is still under discussion (21,–23), our findings would suggest that language therapy could be more easily practiced in the acute phase.
Thus, a comprehensive model of stroke care including, other than the management of acute phase, the initiation of rehabilitation is considered the best way to approach acute stroke patients in most guidelines (24). For the best stroke care, acute hospitalisation extending for about 2 weeks is recommended, which is the same as that in our stroke population.
Therefore, according to previous reports (8), we suggest that a language assessment and therapy should be considered for all aphasic patients in the acute phase during hospitalisation. For this purpose, a speech therapist should be available in the hospital stroke services as part of multidisciplinary stroke team. He should assess the language condition in the acute phase and plan short- and long-term rehabilitation programmes.
Footnotes
Acknowledgements
The Italian Ministry of Health supplied the databases on National Register of Discharge (DRG) for 1999 and 2001.