
Abstract
Stroke is a leading public health problem, causing significant disability and premature mortality, particularly in low- and middle-income countries (LMIC). A public health strategy is required for the prevention and care of stroke in LMIC. Although specific estimates are difficult to calculate, increasing cost-effective interventions that reduce cardiovascular risk in the population can have a substantial impact on stroke burden. Public health interventions that address tobacco use, unhealthy diet (salt and transfat), and physical inactivity of the population need to be complemented with equitable stroke services. The main components of an equitable stroke service include:
• assessment and management of cardiovascular risk in primary care,
• assessment and follow-up of transient ischaemic attack (TIA) patients,
• provision of secondary prevention through a primary health care approach,
• education of the public, health care staff and patients with stroke,
• equitable access to acute stroke care and stroke rehabilitation and
• community and family engagement for support to care givers and stroke patients.
Unless services for stroke care are complemented with prevention programmes to reduce stroke risk in the population, health care costs will continue to escalate due to increasing rates of stroke.
Keywords
Global burden of stroke
Stroke is classified into five subtypes:
ischaemic stroke,
haemorrhagic stroke,
subarachnoid haemorrhage,
central venous thrombosis and
spinal chord stroke (1).
Atherosclerosis and cardiac thromboembolism are the main causes of stroke. In 2004, cerebrovascular disease was the second leading cause of death, contributing to 5·7 million (9·7%) deaths globally. Stroke contributed to 1·5 (rank 5), 3·5 (rank 1), and 0·8 (rank 2) million deaths in low-income, middle-income and high-income countries, respectively (2). In 2004, stroke was the sixth leading cause of the global disease burden, contributing to 3·1% of the total disease burden (measured in DALYs) (2). By 2030, lower respiratory infections, ischaemic heart disease, road traffic accidents and stroke will be the four leading causes of diseases burden, stroke alone contributing to 4·3% of the total DALYs (2) (Fig. 1).
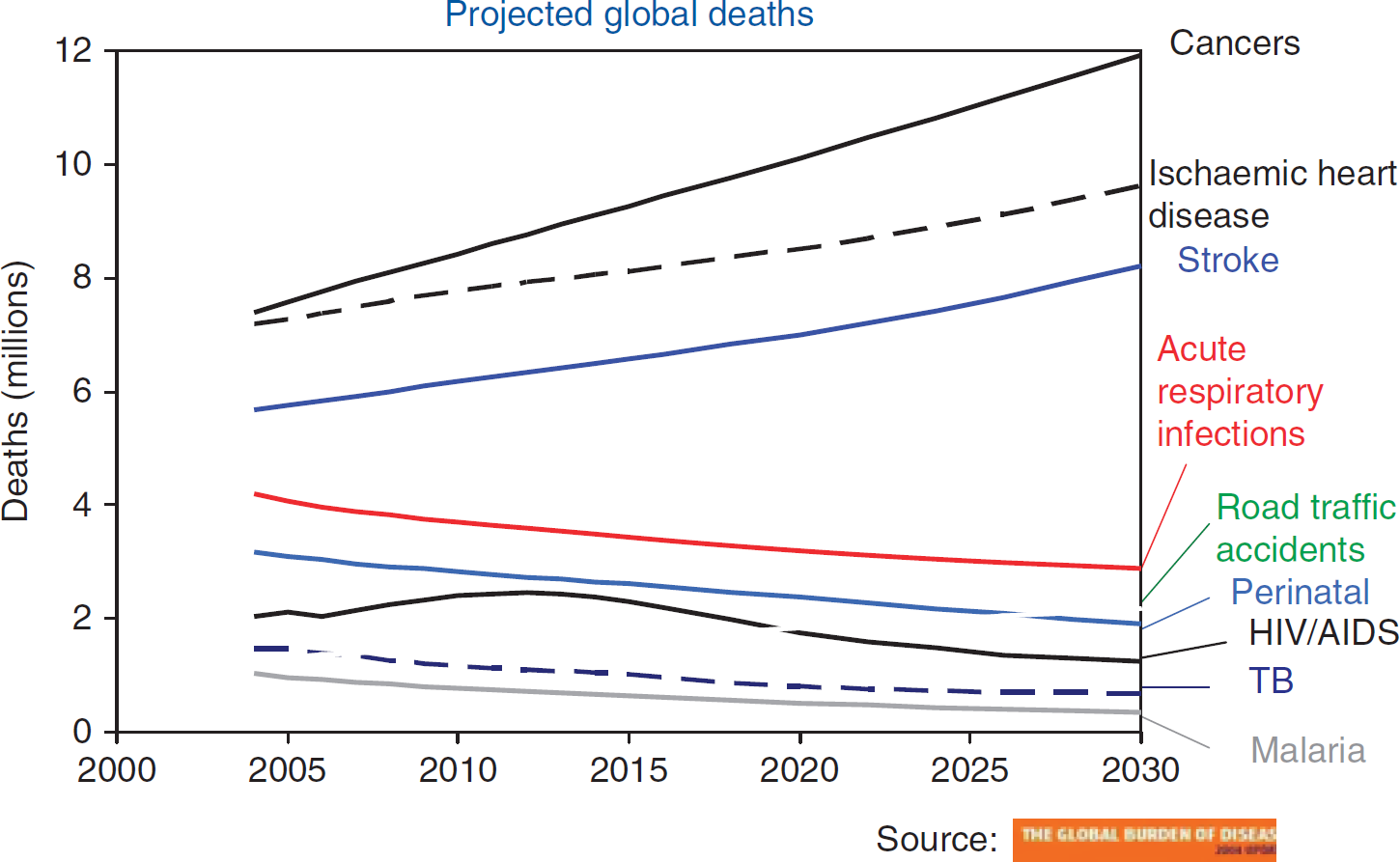
Projected global deaths due to stroke, ischaemic heart disease, cancer and other conditions.
Over the last four decades, stroke incidence has decreased in high-income countries and increased by over 100% in low-income, middle-income countries (LMIC). Currently, the overall stroke incidence rate in LMIC exceeds the levels of stroke incidence seen in high-income countries by about 20% (3).
The rates of stroke mortality and stroke burden vary; however, LMIC are most affected (4). Eastern Europe, North Asia, Central Africa, and the South Pacific are the most affected regions of the world. The main determinants of the stroke epidemic are ageing populations and unhealthy dietary habits, physical inactivity, and tobacco use driven by globalisation and urbanisation. Because of these relentless forces, the stroke burden in LMIC is likely to increase in the next 20 years. If secular trends continue, it is estimated that there will be 23 million first-ever strokes and 7·8 million stroke deaths in 2030 (5, 6).
Increased blood pressure, increased blood cholesterol and tobacco use explain 54%, 15% and 12% of the stroke mortality, respectively (7). These risk factors also accelerate ischaemic cerebrovascular dementia and associated cognitive impairment (8), important health issues in ageing populations.
There are cost-effective interventions to reduce these modifiable risk factors both at population and individual levels, which are applicable to LMIC (9, 10). Cost-effective interventions are also available for the secondary prevention of stroke (11). These primary and secondary prevention and interventions have been implemented effectively in many high-income countries, resulting in a downward trend in stroke mortality (2).
Primary prevention of stroke
Although stroke is eminently preventable in all LMIC, there is inadequate investment in stroke prevention. In LMIC, primary prevention is the only sustainable solution for stroke. Primary prevention should receive top priority, given that even in settings with advanced technology and facilities, the case fatality and disability from stroke is high. Poststroke, 58% of stroke victims either die or become dependant on the family or the society (12).
Primary prevention has two approaches, which have synergistic effects:
Population-wide approaches to reduce stroke risk factors and
Approaches for early detection and management for high cardiovascular risk, through a primary health care approach.
We need a global co-ordinated prevention effort to address major noncommunicable diseases (NCDs), under the leadership of the government health departments. Populationwide primary prevention has been shown to be very cost effective. The early detection and care of those at a high risk of stroke is cost effective and affordable for LMIC only when an absolute risk approach is used (10, 13). This calls for a paradigm shift from vertical programmes targeting single risk factors (which are not cost effective) to a total risk approach. The total risk approach relies on risk stratification based on risk factors measurable even in low-resource settings, e.g. age, gender, tobacco use, blood pressure, blood glucose and blood cholesterol (13).
Primary and secondary prevention of cardiovascular disease and diabetes have many shared elements and need to be integral components of a national prevention programme for NCDs (cardiovascular disease, diabetes, cancer and chronic respiratory disease). A national policy for the prevention and control of NCDs can provide the overarching framework for this integration. Development and implementation of a national NCD policy is therefore one of the key steps in addressing the prevention and control of NCDs including stroke (14).
Lack of reliable data is one of the major challenges for assessing the current level of stroke risk in the population and for monitoring the impact of stroke programmes. Institutionalising the collection of accurate and reliable national mortality data and risk factor surveillance data is therefore a priority.
The perspective of the World Health Organization (WHO)
Recognising the global public health challenge posed by stroke and other NCDs, the World Health Assembly (WHA) endorsed a global strategy for the prevention and control of NCDs in May 2000 (15). This global strategy calls for the surveillance, prevention and management of all major NCDs including stroke through an integrated approach that recognises tobacco, unhealthy diet, physical inactivity and harmful use of alcohol as risk factors shared by major NCDs. In 2008, the WHA also endorsed an action plan for the implementation of the global NCD strategy (16, 17). The action plan outlines the priority activities for WHO, its member states and the international community and provides a roadmap for the prevention and control of NCDs including stroke.
Stroke shares behavioural risk factors (tobacco use, unhealthy diet and physical inactivity) and intermediate risk factors (increased blood pressure and increased blood cholesterol) with other major NCDs (16, 17). A public health approach that addresses stroke as one of the major NCDs is absolutely essential for addressing the stroke epidemic in LMIC. In this context, an integrated national NCD policy, which is aligned with the national health development plan, can provide a firm platform for launching a coherent and sustainable public health response for all major NCDs including stroke.
Determinants of modifiable risk factors (unhealthy diet, physical inactivity, tobacco use, increased blood pressure, increased blood sugar, increased cholesterol and harmful use of alcohol) of stroke mainly lie outside the health domain in the jurisdictions of trade, food and agriculture, sports, urban planning and finance. These determinants can only be addressed by managing the impact of government policies related to these domains through intersectoral collaboration. Multisectoral strategies that cut across different disciplines are required to create structural changes and better environments for promoting healthy behaviours in childhood and throughout life.
Strategies for the primary prevention of stroke
Cost-effective primary prevention strategies include tobacco control, action against an unhealthy diet and encouragement of physical inactivity (9, 10, 15). WHO's Framework Convention on Tobacco Control (18) and the global strategy for diet, physical activity and health (20) are excellent resources for these strategies.
A modest reduction in salt intake has a significant effect on blood pressure in both individuals with normal and increased blood pressure (19). There is also a correlation between the magnitude of salt reduction and blood pressure reduction within the daily intake range of 3–12 g/day; the lower the salt intake, the lower the blood pressure (21).
The WHO has set a global target for maximum intake of salt for adults at 5 g/day (i.e., 2000 mg/day of sodium) or lower if specified by national targets (22). Several countries in the European Union have agreed to reduce salt intake by 16% over the next 4 years (23).
Rural areas in LMIC countries, where most of the salt consumed comes from, need a public education campaign to encourage less salt use. Urban areas in LMIC also have increased salt intake due to increased consumption of processed and prepared food. In these areas, a combination of measures including a food industry response to reduce the amount of salt added to food, food labelling and consumer education will be required to reduce the population intake of sodium.
Aspirin reduces stroke risk although not myocardial infarction in women; in men, only the risk of myocardial infarction is reduced but not stroke significantly (24). Aspirin also increases the risk of bleeding (25). The expected benefits might not exceed the risk of major bleeding, particularly among those at a low cardiovascular risk (<20% over 10 years) or among older patients (>70 years) at a high risk of bleeding even in individuals with diabetes (26). As such, aspirin is recommended for primary prevention in only those with a high cardiovascular risk (>30% over 10 years) (10).
Other evidence-based primary prevention interventions targeting individuals include pharmacological and nonpharmacological interventions for tobacco cessation, and blood pressure and cholesterol reduction (10).
These evidence-based interventions are cost effective, particularly when targeted at high-risk groups.
Acute stroke care and secondary prevention of stroke
For patients with acute stroke, aspirin within 48 h of stroke onset, management in a stroke care unit, thrombolytic therapy within 3 h or/and decompressive surgery for supratentorial malignant hemispheric cerebral infarction are interventions of proven benefit (27). Aspirin has been shown to be safe and effective in the first 48 h after an ischaemic stroke (28). In suspected ischaemic stroke, aspirin reduces the risk of death and dependence by 12 individuals per 1000 treated. Thrombolytic therapy is associated with 12% fewer deaths or dependent individuals overall, but 7% more fatal and nonfatal brain haemorrhages and 6% more early deaths (29).
Proven secondary prevention interventions are tobacco cessation, antihypertensive therapy, antiplatelet agents, cholesterol reduction with statins, warfarin for patients with atrial fibrillation and endarterectomy for symptomatic carotid stenosis (11). Tobacco cessation, combined with aspirin and reduction of cardiovascular risk with antihypertensive and statins, have the potential to reduce recurrent vascular events by nearly 75% (11). Aspirin/dipyridamole and clopidogrel both reduce the risk of a combined cardiovascular outcome in long-term secondary prevention compared with aspirin alone (30). However, more potent antiplatelet drugs or a combination of aspirin and clopidogrel also cause more bleeding complications.
Prompt assessment and investigation of a TIA, followed by initiation of secondary prevention measures is effective in reducing recurrent stroke (11). The risk of early stroke following a TIA may be as high as 12% at 7 days and 20% at 90 days (31). The TIA therefore requires urgent medical attention. All patients with suspected TIA should be assessed at the first contact level of health care, for their risk of stroke and referred for specialist care.
In patients with atrial fibrillation, oral anticoagulation is superior to aspirin in stroke prevention (32). The choice between oral anticoagulants and aspirin in these patients depends on age and the individual risk factor profile (32–34).
The beneficial outcomes of organised care for stroke have been recognised both in observational studies and in clinical trial settings (35). The benefits include improved survival, increased chances of returning home and regaining independence. Co-ordinated care in stroke units reduces mortality and dependence by 56 per 1000 receiving such treatment.
Challenges of the prevention and management of stroke in LMIC
Stroke is a leading cause of death, disability and dependence in LMIC (16, 17). At present, the age-specific mortality in some LMIC is higher than that in high-income countries (36). With ageing of populations in LMIC, a further increase in stroke mortality can be expected in the future. Stroke often results in loss of employment as well as catastrophic spending on health care. This is particularly the case in LMIC, where the majority of individuals have no health insurance and health care is expensive (37).
Acute stroke care requires guidance for early identification of eligible patients by health care workers and their urgent transfer to expert treatment centres. Thrombolysis, if indicated, and aggressive supportive care need to be provided in emergency care units. Such centres must also be able to offer imaging, admission to a stroke unit and access to a neurologist.
Low- and middle-income countries are ill equipped to provide such care for acute stroke, for many reasons.
First, the high costs of thrombolytic therapy are a major barrier for LMIC introduction. In most LMIC, such therapy would be unaffordable for unemployed and uninsured patients; this is the case for 2 billion of the world's population who live on <US$2 a day. Even if thrombolytic therapy and acute stroke care are made available at heavy societal costs, most patients seen in emergency departments in LMIC are unlikely to be eligible for thrombolysis due to delay in seeking care due to lack of awareness or lack of access (38).
Second, unlike high-income countries, where there may be 24-h access to CTscanning (39), in LMIC, imaging facilities are not available for most individuals (40).
Third, there is a critical shortage of neurologists and general health workers (41).
The outcome of stroke can be improved by organised care in stroke units. Stroke unit care, however, is a complex intervention and there are many challenges in implementing stroke unit care in resource-constrained settings (42). Further cost implications of wide implementation of organised stroke care maybe unaffordable to many LMIC as most of them invest too little on health (Fig. 2).
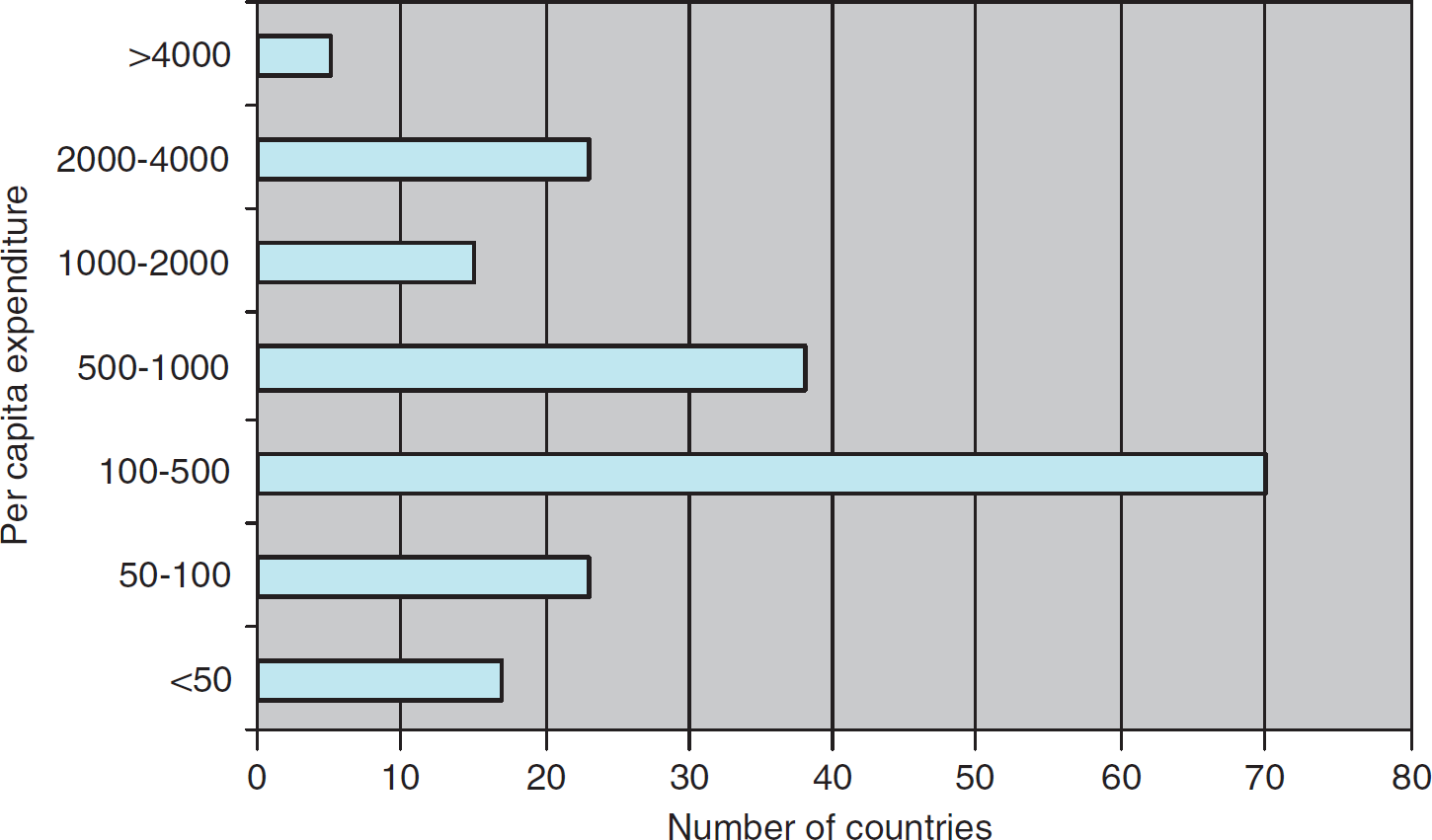
Per capita total expenditure on health 2006 in 193 countries (PPPint.$): http://www.who.int/whosis/data/Search.jsp?countries=[Location]
Opportunities for the prevention and management of stroke in LMIC
Emphasis needs to be given to upstream public policy measures for population-based prevention programmes, improving consumer access to information, improving clinical practice patterns in primary care through education and clinical support tools, strengthening provider, carer and patient communication and promoting self-management.
Stroke prevention and treatment cannot be addressed cost effectively through a vertical disease-oriented programme. The intermediate risk factors, increased blood pressure, increased blood sugar and increased blood cholesterol are common to vascular disease of different vascular territories; stroke, coronary heart disease and peripheral vascular disease. Programmes for the prevention of these diseases can therefore be well integrated, particularly, in primary care (43).
Stroke services, including primary prevention in high-risk individual, rapid diagnosis, early use of aspirin (44), preventing aspiration, addressing swallowing difficulties, treating fever and pulmonary infections and prevention of stroke recurrences, are feasible in primary care.
Transient ischemia attack can also be diagnosed by primary care physicians if the history confirms; sudden onset of symptoms, with maximal neurological deficit at onset; symptoms typical of focal loss of brain function such as unilateral weakness or speech disturbance; and rapid recovery usually within one hour. Once diagnosed, individuals at a high risk of stroke can be referred for specialist assessment quickly. Diabetes is becoming increasingly prevalent in LMIC and is associated with an increased risk of stroke. Early diagnosis, risk stratification and reduction of cardiovascular risk through optimal blood pressure control and glycaemic control are critical for reducing the risk of stroke; these measures can also be implemented in primary care (43).
The public needs education on stroke risk factor reduction and the importance of seeking prompt medical attention after TIA/stroke. Doctors need to be trained and made aware of the importance of a correct diagnosis, timely referral and evidence-based primary and secondary prevention of stroke.
Secondary prevention strategies for stroke include lifestyle management, the use of antithrombotic and antihypertensive agents and lowering of blood cholesterol (11). The WHO is providing technical support to integrate essential interventions for primary and secondary prevention of stroke and other NCDs into PHC in low-resource settings (43). The objective is to develop context-specific models of care that engage communities and are suitable to local needs.
Stroke unit care delivered by trained multidisciplinary teams working within a dedicated stroke unit may be too costly for wide implementation in LMIC. Other models need to be explored including ‘mobile stroke services’ with multidisciplinary teams that manage stroke patients in different wards in a hospital to ‘care’ in medical wards provided by general physicians and their support staff.
Low- and middle-income countries should also explore the use of telemedicine tools to strengthen stroke care. Telemedicine tools that have been shown to facilitate stroke care in remote settings include telephone consultation between a peripheral centre and a stroke centre, low-cost videoconferencing and radiological transfer of CT images (45).
Summary
A public health strategy is required to address stroke in LMIC. The key components of such a strategy include:
a national stroke programme within an overarching national NCD policy framework,
survey of stroke risk factors and a risk factor surveillance system institutionalised within the national health surveillance system,
a stroke prevention service integrated with NCD prevention focusing on implementation of the FCTC, and platforms to reduce salt and transfat in processed foods,
school, community and worksite health programmes to reduce risk factor levels by making structural changes and providing incentives to promote healthy behaviours,
primary and secondary prevention of stroke through a PHC approach and integrated with other NCDs,
early detection of high-risk individual in worksites and communities through an absolute risk approach,
public education campaigns to create awareness of risk factors of stroke and symptoms of TIA and stroke,
evidence-based clinical practice for management of individuals with high stroke risk, TIA, acute stroke and stroke rehabilitation,
strengthened capacity for acute stroke care and stroke rehabilitation services: shorten time to admission, improve access to imaging and intensity of therapy and discharge planning,
assessment (and modification) of the impact of government policies on stroke and NCDs, e.g. policies related to transport, trade, finance, education and sports, agriculture and food.