
Abstract
Fibromuscular dysplasia is an uncommon, segmental, nonatherosclerotic arterial disease of unknown aetiology. The disease primarily affects women and involves intermediate-sized arteries in many areas of the body, including cervical and intracranial arteries. Although often asymptomatic, fibromuscular dysplasia can also be associated with spontaneous dissection, severe stenosis that compromises the distal circulation, or intracranial aneurysm, and is therefore responsible for cerebral ischaemia or subarachnoid haemorrhage. Fibro-muscular dysplasia affects middle and distal portions of the internal carotid and vertebral arteries, and occasionally, intracranial arteries. Several pathological and angiographic patterns exist. The most frequent pathological type is medial fibromuscular dysplasia, which is associated with the ‘string of beads' angiographic pattern. Unifocal lesions are less common and can be associated with several pathological subtypes. The pathophysiology of the disease is widely unknown. Fibromuscular dysplasia may in fact result from various causes and reflect a non-specific response to different insults. The poor knowledge of the natural history and the lack of randomised trials that compared the different treatment options do not allow any satisfactory judgement to be made regarding the need for or the efficacy of any treatment.
Keywords
Fibromuscular dysplasia (FMD) is an idiopathic, segmental, noninflammatory, nonatherosclerotic vascular disease of small- to medium-sized arteries that most commonly affects the renal and carotid arteries but has been described in almost every arterial bed in the body (1 2). It occurs frequently in young individuals and women. The disease was first described as fibromuscular hyperplasia in patients with renal stenosis; however, subsequent pathological classifications used the term FMD (3–6). The first histologically proven case of FMD of the carotid artery was reported by Connett and Lansche in 1965 (7). Histologically, FMD lesions are heterogeneous, with various degrees of collagen hyperplasia, internal elastic lamina rupture, and disorganisation of the media layer. As pathological specimens are rarely obtained, the diagnosis of FMD is most often made on the basis of a characteristic angiographic appearance. Three hundred cases of FMD involving cervical or intracranial arteries were reported up until the 1980s (8 9); recent data are relatively limited and have thus provided us with little further knowledge of the disease. Conventional angiography is now rarely performed in patients with cerebrovascular disease, and the low resolution of the first generation of noninvasive arterial imaging techniques, and the vascular artefact seen at the upper level of cervical arteries on MR angiography could have resulted in an underestimation of the disease. The traditional view that FMD has a benign prognosis could also explain this apparent lack of interest in the disease. Yet, FMD can be associated with severe ischaemic or haemorrhagic stroke (10–15).
Epidemiology
Little is known about the epidemiology of cervical and intracranial FMD. The exact frequency of the disease is difficult to assess because many cases are asymptomatic. In earlier reports of consecutive angiograms performed in imaging departments, the prevalence of FMD ranged from 0.3% to 3.2% (8 16–20). However, the prevalence observed in these studies cannot be generalised to the entire population because angiograms were usually performed in patients who had neurological diseases, including cerebrovascular diseases. In addition, the definition of FMD may have varied across studies. The apparent lesser frequency of cervical and intracranial FMD compared with renal FMD may be explained by the fact that renal FMD is more likely to be symptomatic because of hypertension. However, over a 25-year period, FMD of the internal carotid artery was detected in only four of 20 244 consecutive autopsies (0.02%) performed at the Mayo Clinic (21), suggesting that cervical and intracranial FMD is indeed less common than renal FMD (1). The frequency of FMD in patients with ischaemic stroke, TIA, or subarachnoid haemorrhage (SAH) is likely to be very small but has never been estimated precisely. There are little data on the prevalence of cervical and intracranial FMD in patients with renal FMD. Using conventional angiography, Stanley et al. (22) reported a prevalence of 9% of extracranial carotid or vertebral artery dysplasia among 196 patients with renal FMD. In a study of 92 patients with FMD, Lüscher et al. (23) found that 28% had FMD involving two or more arterial sites, corresponding most commonly to combined carotid and renal lesions. Other studies found a higher prevalence of cervical artery abnormalities in patients with renovascular hypertension than in controls. However, the authors did not separate FMD from atherosclerosis in their analysis (24 25). Finally, using high-resolution echotracking, Boutouyrie et al. (26) identified an arterial phenotype of the carotid artery, defined as a ‘triple signal’, that was strongly associated with FMD. Patients with renal FMD were about 13 times as likely as controls to have this phenotype, suggesting that FMD is a systemic disease, with silent lesions being common in apparently unaffected arterial sites.
Intracranial saccular aneurysms are usually considered as a frequent finding in patients with carotid or vertebral FMD, with prevalence ranging from 20% to 50% (27). This prevalence might, however, be overestimated, as most studies did not correct their estimates for the selection bias introduced by the fact that patients who had SAH were usually investigated by cerebral angiography. In a systematic review of FMD series that reported the prevalence of intracranial aneurysms stratified according to whether patients had SAH or not (27), the unweighted prevalence of asymptomatic intracranial aneurysm was 7.3% (95% confidence interval, 5.1–9.5) after exclusion of patients who had SAH. Although lower than reported previously, this prevalence remained higher than in the general population. Interestingly, the authors of this systematic review reported that among 1084 aneurysms treated in their hospital between 1976 and 1998, 28 (2.6%) were found in patients with FMD. The ad hoc committees of the AHA Stroke Council Guidelines recommend that magnetic resonance angiography of the head should be performed in all patients with cervical FMD (28). There are no data on the prevalence of intracranial aneurysms in patients with renal FMD.
Pathological classification
The current pathological classification based on the dominant arterial wall layer involved:
intima, media or adventitia (Table 1).
Pathologic classification of FMD (adapted from (22)
This classification has been developed in patients with renal FMD, but similar lesions have been observed from autopsy reports or operative specimens of patients with cervical or intracranial FMD (29). Macroscopically, FMD is characterised by alternating areas of thickening and thinning of the arterial wall, with mural aneurysms. Less often, FMD lesions are focal and correspond to a short ring-shaped or semi-circumferential stenosis or to a tubular and regular stenosis. Intimal FMD (also called intimal fibroplasia) accounts for <10% of all FMD lesions. It corresponds to circumferential or eccentric deposition of collagen in the intima. Mesenchymal cells are arranged within a loose matrix of subendothelial connective tissue. The internal elastic lamina is identifiable but may be fragmented or duplicated. This type seems to occur primarily in children and adolescents and to affect both genders equally. Medial FMD is the most frequent subtype, accounting for about 80% of FMD lesions. Histologically, there are alternating areas of thinned media and thickened fibromuscular ridges containing collagen, resulting in multiple stenoses alternating with aneurysmal outpoutchings. The ‘string of beads’ aspect on angiogram is characteristic of this FMD subtype, with beads exceeding the diameter of the proximal unaffected part of the artery. Some areas of the internal elastic lamina have disappeared. Perimedial FMD is the first subtype of medial FMD, accounting for about 10% of all FMD lesions. It corresponds to extensive collagen deposition in the outer half of the media at the junction of the media and adventitia. Lesions do not extend outside the external elastic lamina. Perimedial FMD may also appear as arterial beading on angiogram. However, unlike medial FMD, the caliber of the beads does not exceed that of the proximal artery and the beads are usually less numerous. Medial hyperplasia is the second subtype of medial FMD corresponding to a true smooth muscle hyperplasia without fibrosis. It is observed in only 1–2% of all lesions and appears as a concentric, smooth stenosis on angiogram. Adventitial FMD is rarely observed (<1%). Fibrous tissue of the adventitia is replaced by dense collagen, whereas the other arterial layers and elastic lamina remain intact. Importantly, the different types may coexist.
Aetiology
The cause of FMD is unknown. The disease is more common among first-degree relatives of patients with the disease and it has been observed in identical twins, suggesting that FMD can be inherited (30–32). Using a high-resolution echotracking arterial score as a surrogate marker of FMD and the segregation analysis method, arterial wall subclinical lesions have been demonstrated in relatives of patients with renal FMD, with a distribution of abnormalities consistent with an autosomal dominant transmission (33). However, most patients have no family history of symptomatic FMD, and to date, the few molecular genetic studies have failed to identify the genetic polymorphisms associated with FMD (1 34). Fibromuscular dysplasia is far more prevalent in women than in men and the disease is frequently diagnosed during pregnancy, suggesting that hormonal factors may be involved. However, a case–control study failed to show an association between FMD and the number of pregnancies or the use of oral contraception (35). It has been shown that FMD patients are more likely to smoke than controls and smoking is associated with more severe FMD (1 35). However, the potential mechanisms by which smoking contributes to FMD aetiology are unknown. Mechanical factors could be involved in the aetiology of FMD (29). Indeed, in vitro, cyclic stretching of arterial smooth cells results in an increase in collagen production. FMD is more common on the right than on the left renal artery and the right kidney has an increased mobility compared with the left one (1). However, no association between kidney mobility and FMD was found in a case–control study (35). Similarly, during extension and rotation of the head, the distal segment of the internal carotid artery (i.e. the cervical site preferentially involved by FMD) is particularly prone to stretching and shearing around the bony margins of the uppermost cervical vertebrae. Vasa vasorum of muscular arteries invariably originate from branches of the parent vessel. The renal and extracranial carotid arteries have relatively few branches compared with other vessels of similar calibre. It has been suggested that a vasa vasorum disease may result in mural ischaemia, leading to FMD lesions. This hypothesis is supported by the frequent involvement of the outermost part of the media where ischaemia predictably would be the greatest (22). A congenital origin is also plausible. During foetal life, the tunica muscularis develops first on the main trunk and later on its branches. The proximal portion of the internal carotid artery is derived from the third aortic arch and the rest of the artery is derived from the left dorsal aorta. It has also been suggested that focal lesions encountered in adulthood may represent persistent embryonic intimal cushions (22). Finally, the pathophysiology of intimal FMD may differ from that of medial FMD (22). Indeed, intimal FMD may represent sequelae of arterial injuries, including external trauma as well as intraluminal insults arising from local alterations in blood flow. Long, irregular, tubular stenosis seen in infancy may reflect the aftermath of an arteritis. In fact, FMD may result from various causes and reflect a non-specific response to different insults.
Clinical presentation
Renal FMD, cervical and intracranial FMD typically occur in young women; however, in most series of patients with cervical FMD, the mean age at diagnosis was over 50 years (Table 2) (9). Fibromuscular dysplasia is associated with focal ischaemic symptoms due to either a thromboembolic mechanism or a haemodynamic compromise of the distal circulation (36). In addition, some patients develop complications of this disorder, including spontaneous dissection (37–39), aneurysms and carotid-cavernous fistulas (40 41), or vertebral arterio-venous fistulas, all of which are sometimes associated with focal neurologic deficits (42). Subarachnoid haemorrhage usually results from intracranial aneurysm rupture. However, SAH has also been described in patients with no visible aneurysm at angiography, but in whom autopsy showed basilar artery FMD associated with ruptured microaneurysm (43). Arterial dissections occur in patients with FMD (44), and up to 15% of patients with cervical artery dissection have signs of FMD on imaging (45). However, the diagnosis of FMD can be challenging in case of acute dissection, as angiographic features of both diseases can be similar. It is likely that, in the past, FMD was overdiagnosed in patients with cervical artery dissection, as mural haematoma was not investigated with appropriate imaging techniques. Horner's syndrome is also a classical manifestation of FMD (8). However, it is possible that these patients in fact suffered from an acute carotid artery dissection. Finally, some patients hear pulsatile tinnitus and most patients have a cervical bruit on physical examination.
Circumstances of the diagnosis of cervical and intracranial FMD in the main series (>10 patients) from the literature
*Isolated tinnitus that led to diagnosis of FMD. FMD, fibromuscular dysplasia; NA, not assessable.
The majority of patients, however, seem to be asymptomatic (46). In the literature of the 1980s, cervical FMD was often found in patients who had non-specific symptoms including headaches, vertigo, syncope, seizures, or several neurological diseases (notably brain tumours) that required cerebral angiography at that time. However, those circumstances are likely to be less frequent nowadays because such patients are no longer investigated by angiography.
Angiographic features and pathological correlations
Fibromuscular dysplasia affects the middle and distal portions of the internal carotid and vertebral arteries at the level of the C1 and C2 vertebrae (i.e., the distal extracranial artery), arterial areas usually spared by atherosclerosis. The majority of cervical FMD cases involve the internal carotid artery (95%), often bilaterally (60–85%). Vertebral artery involvement is less common and usually coexists with carotid FMD. While the correlations between pathological and angiographic features have been assessed formally in renal FMD (47 48), data on cervical and intracranial arteries are based on isolated case reports or small series (9 13 16). Four angiographic subtypes have been described in renal FMD. The multifocal type, with multiple stenoses and the ‘string of beads’ appearance is the most common angiographic subtype and is generally associated with a medial FMD on histology. Unifocal FMD includes the tubular subtype, corresponding to a long concentric stenosis, and the focal type, corresponding to a short isolated stenosis <1 cm in length. These unifocal subtypes cannot be related to specific histological lesions, although intimal FMD seems to be more common. Finally, up to 20% of patients have mixed-type stenoses. Most data are from conventional angiography.
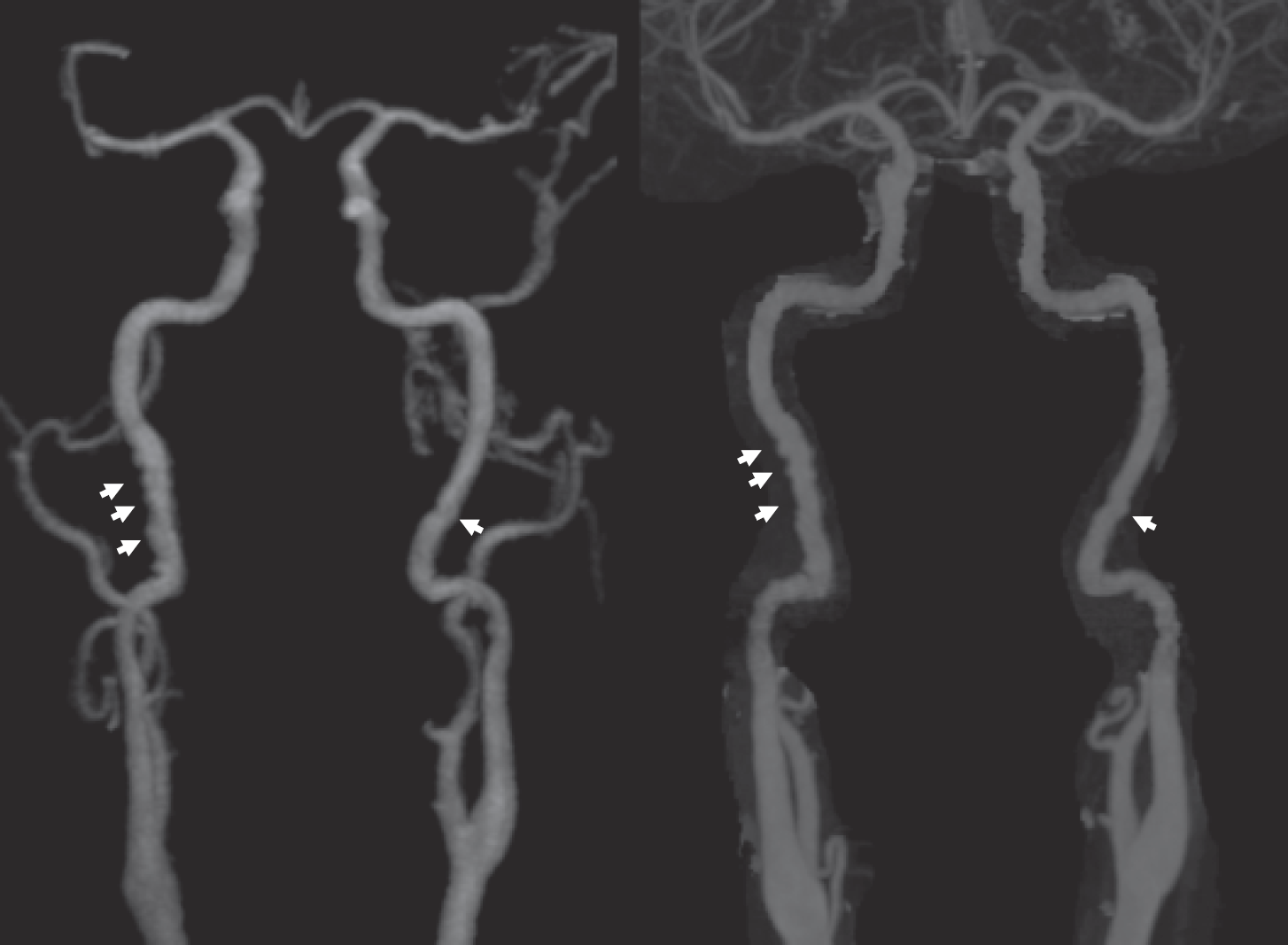
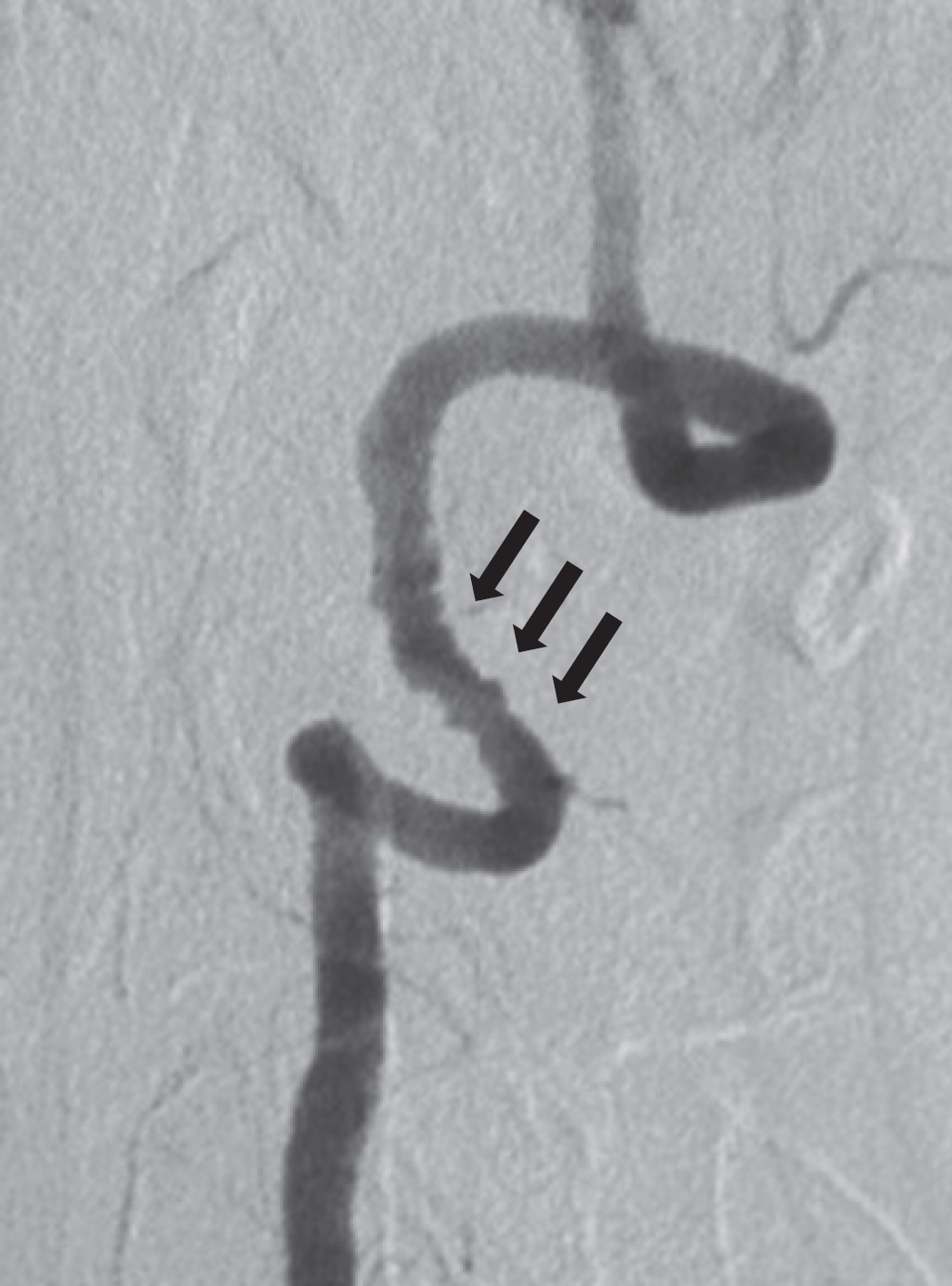
As for renal FMD, the ‘string of beads’ pattern is the most frequent angiographic pattern, accounting for about 80% of patients in most series (Figs 1–4) (13), and is usually associated with a medial FMD on histology. The diseased arterial segment generally has a greater diameter than the normal distal and proximal segments. Tortuosities and kinking are common. The ‘bristling’ appearance reflects the presence of mural microaneurysms (Fig. 5). The angiographic differential diagnosis includes stationary waves or circular spastic constrictions of the extracranial carotid and vertebral arteries. However, the constrictions are more regular, evenly spaced, and occur without the dilatation of intervening segments so typical of FMD.
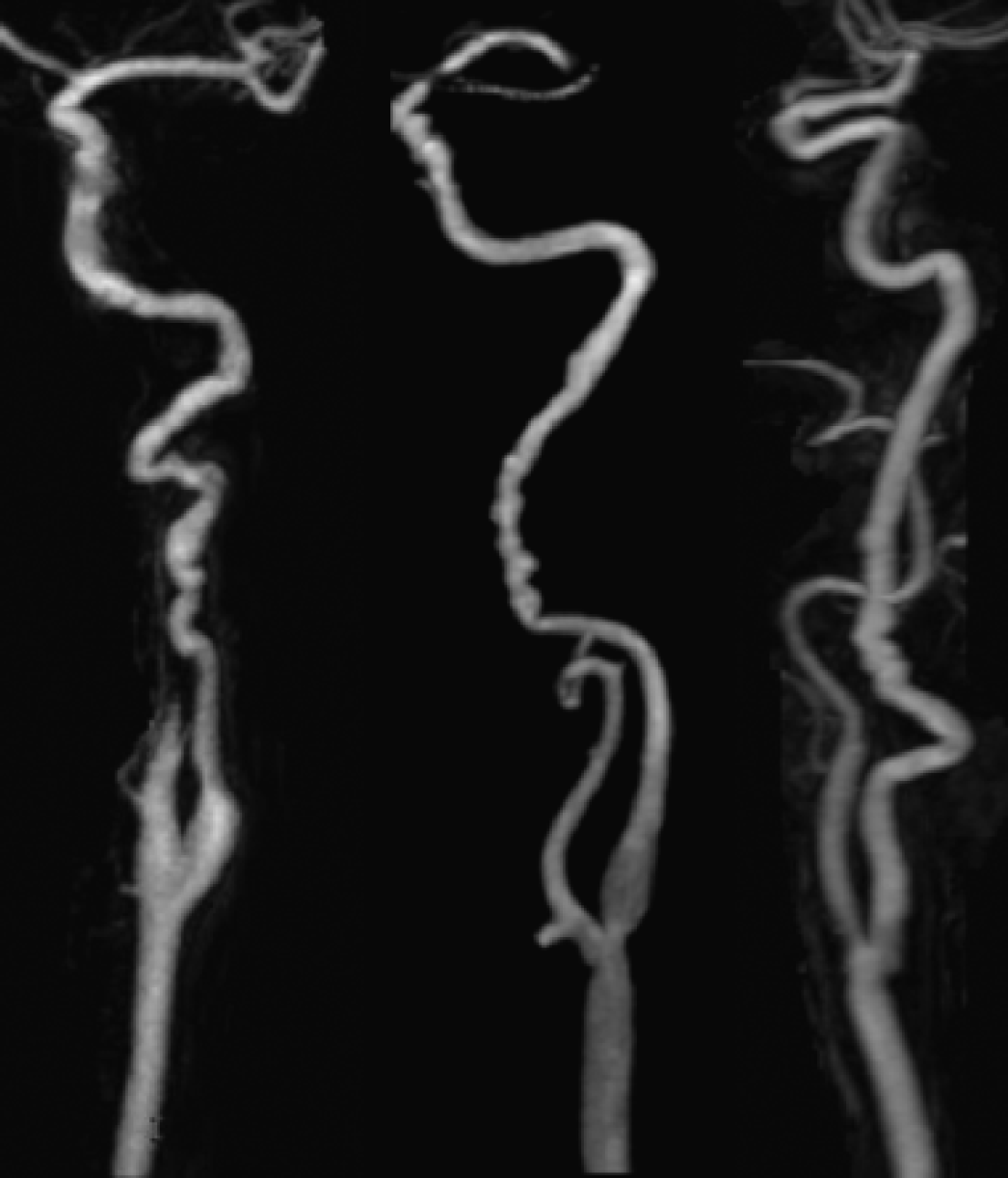
Typical aspects of carotid fibromuscular dysplasia (magnetic resonance angiography).

Typical aspects of vertebral fibromuscular dysplasia (magnetic resonance angiography).
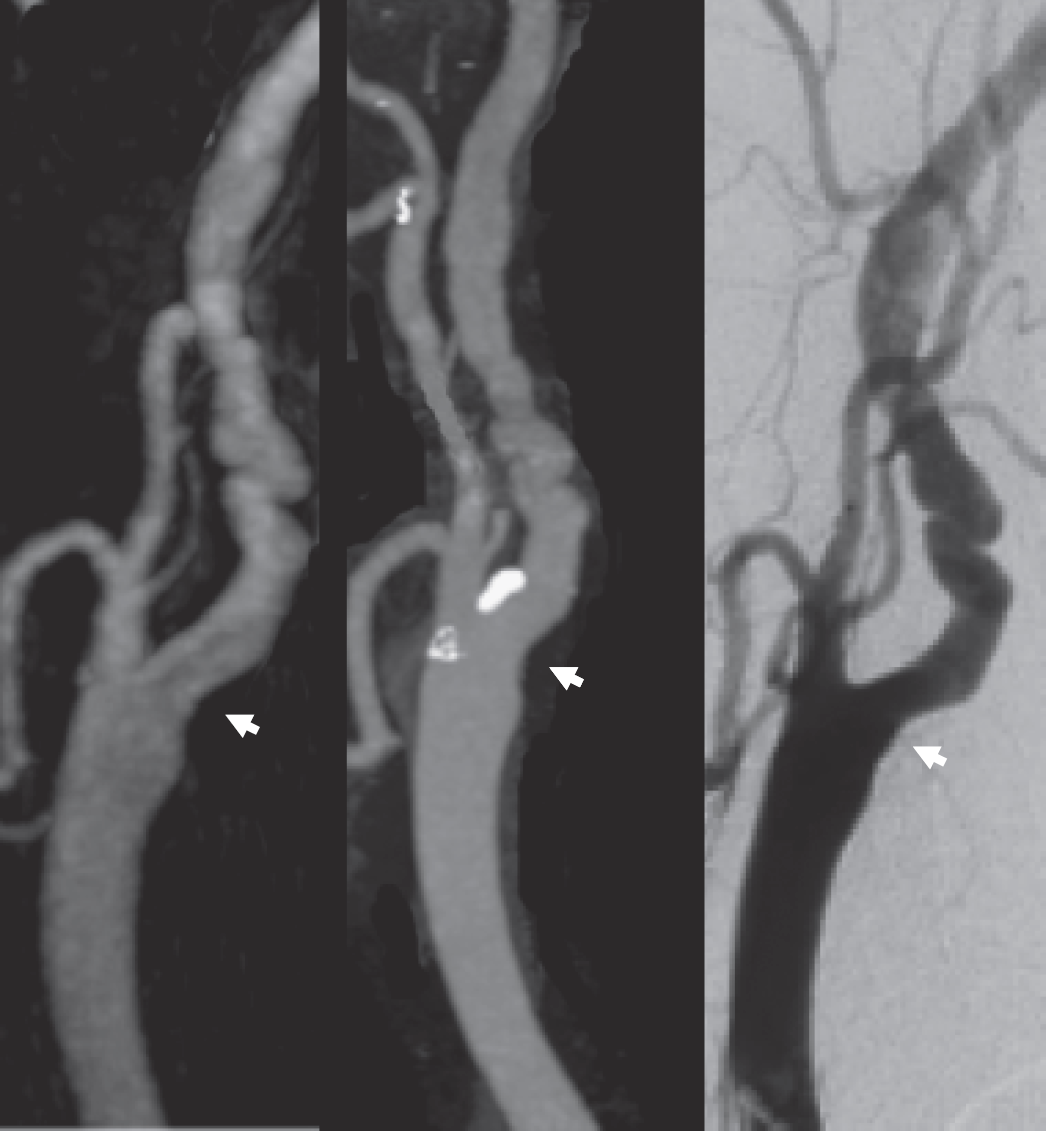
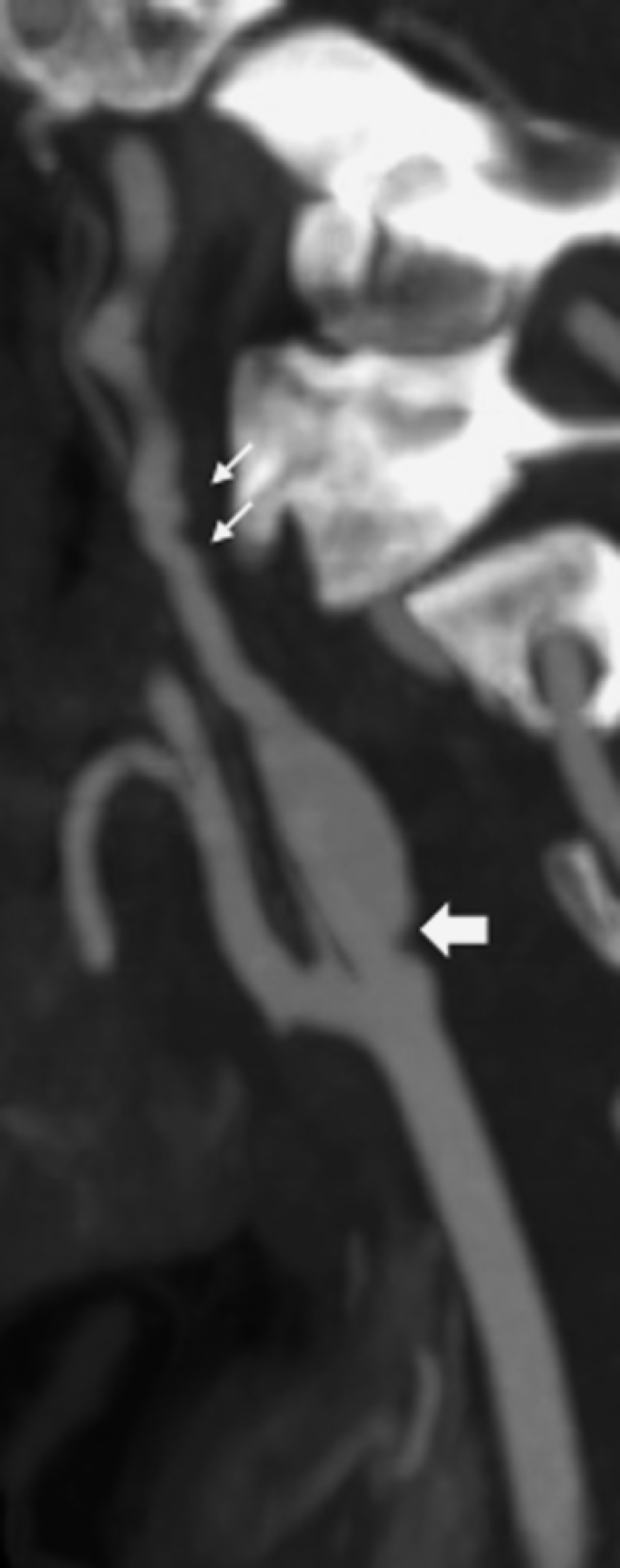
Typical aspect of carotid fibromuscular dysplasia (magnetic resonance-angiography, computed tomography scan, conventional angiography) in a 61-year-old man with recurrent strokes. Note the presence of an atherosclerotic plaque at the bifurcation.
Mild carotid fibromuscular dysplasia on magnetic resonance angiography and computed tomography scan.
Mural microaneurysms on a vertebral artery (conventional angiography) with a ‘bristling’ aspect.
The second, much less common, angiographic pattern is unifocal stenosis that can be tubular or localised (Fig. 6). Those smooth concentric lesions are less specific than the ‘string of beads’ pattern and can be associated with any histological type of FMD (8 13). FMD diagnoses in patients with focal or tubular lesion are difficult as atherosclerosis, arteritis, external compression, or carotid hypoplasia can mimic FMD.
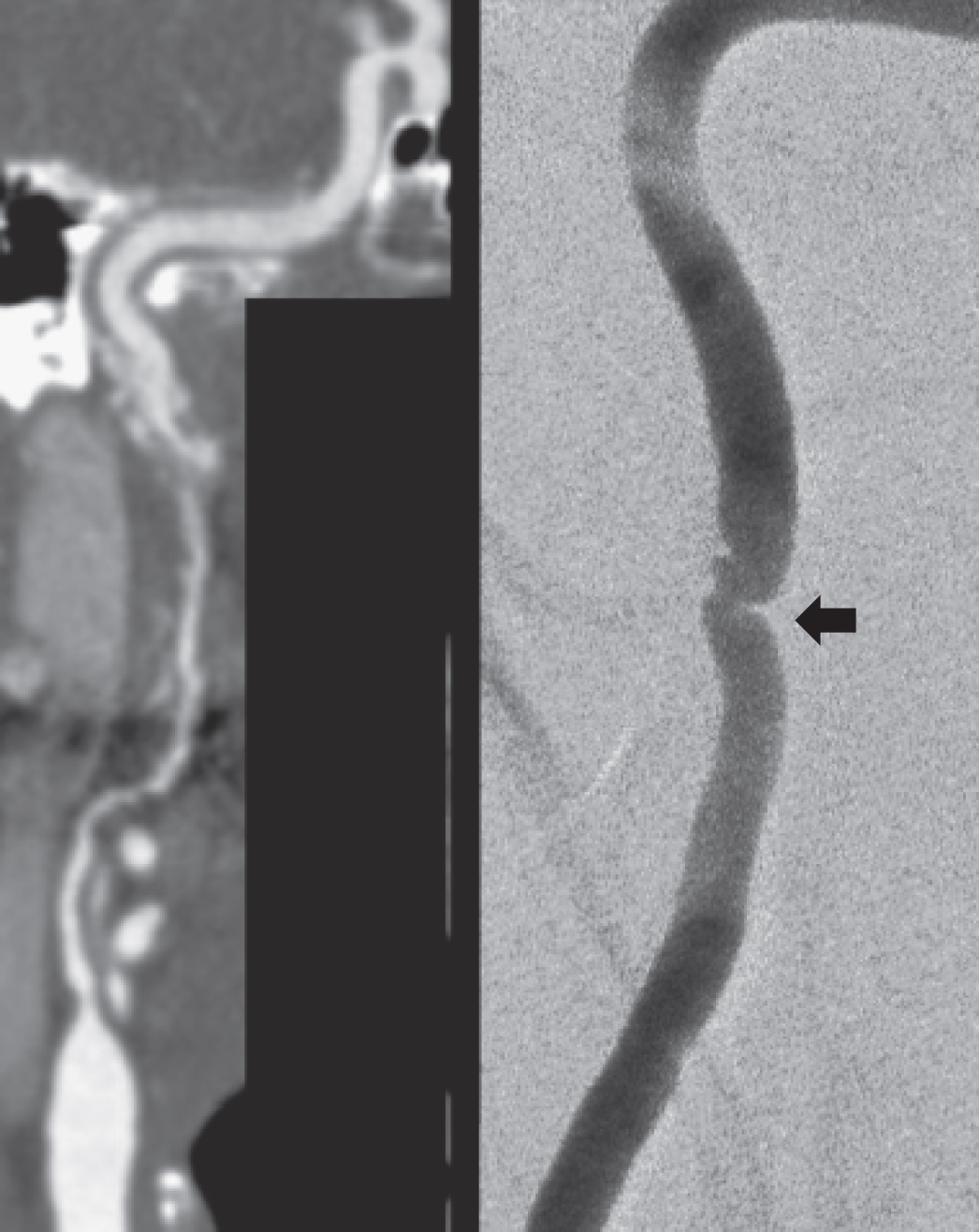
Unifocal carotid fibromuscular dysplasia lesions – Left: long lesion (computed tomography scan) – Right: short, diaphragm (conventional angiography)
The third well-documented pattern of FMD corresponds angiographically to a ‘web-like’ defect at the origin of the internal carotid artery (Fig. 7) (12 13 49–51). This particular feature is rare, with <20 cases reported in the literature, and seems to be associated with a black-ethnic origin and responsible for quite severe strokes (12). Histologically, this form corresponds to intimal FMD.
Web-like fibromuscular dysplasia lesion at the origin of the right internal carotid artery in a 40-year-old African women with no risk factors and who suffered from a severe right hemispheric stroke (large arrow). Typical aspect of FMD above.
Unilateral involvement of the arterial wall ranging from a corrugated diverticulum-like outpouching with noncircumferential narrowing to a true aneurysm has been attributed to FMD, usually because patients had a typical aspect of FMD on the contralateral artery (8 20). However, this subtype has not been proven to correspond to FMD histologically and was likely to correspond to acute dissecting aneurysm or the aftermath of a dissection.
Interestingly, histologically proven involvement of the external carotid artery has been reported occasionally (15 52–55). However, data on angiographic FMD patterns of the external carotid artery are very limited. Andersen (53) reported a typical ‘string of beads’ aspect of the main occipital artery in one patient, but without FMD involving the internal carotid or vertebral arteries.
Intracranial FMD
Apart from intracranial aneurysms, intracranial FMD seems to be rare. Most often, intracranial FMD corresponds to an intracranial extension of extracranial FMD (13 15 36 52 55–57). However, a few cases of isolated intracranial FMD with a typical ‘string of beads’ appearance on angiography, with or without histological verification (Fig. 8), involving the basilar artery (58), the distal carotid artery, and the middle cerebral artery have been reported (15). There are also a few reports of patients with histologically proven FMD revealed by fatal intracranial artery dissection (59) or subarachnoid haemorrhage due to middle cerebral artery or basilar artery rupture (43 60–62). Some patients have multiple aneurysms distributed along a single arterial segment and extensive dilatation of the intracranial internal carotid artery with multiple tortuosities (54 63). This latter angiographic pattern does not correspond to any classical type of FMD mentioned above and intimal FMD was found in the only histologically proven case (54). In some young patients, FMD has also been associated with the moya–moya syndrome (14 64). In contrast to FMD of extracranial arteries, in which the media is involved in most cases, the intimal form of FMD seems as common as the medial form when intracranial vessels are affected (65). Interestingly, most paediatric cases of FMD involved intracranial vessels (6 65–67).

Intracranial carotid artery fibromuscular dysplasia in a 37-year-old smoker women with no other risk factors. The patient otherwise had a typical pattern of FMD on high-resolution echotracking.
Prognosis
The natural history of this disorder is not well known. The risk of ischaemic stroke or TIA ranged from 0% to about 5% per year in the few studies that assessed the prognosis of patients with extracranial FMD (Table 3). However, these studies included heterogeneous populations (symptomatic or asymptomatic FMD and no standardised treatment) and some had a high proportion of loss to follow-up patients. No study has systematically assessed the arterial prognosis of extra- or intracranial lesions of FMD. The progression of cervical lesions has been documented in a few patients (13 68 69). In patients with renal FMD, progression of disease is also well established, although not well quantified (1). Finally, although up to 15% of patients with cervical artery dissection have FMD, the risk of dissection in patients with FMD is unknown. A study has suggested that patients with cervical artery dissection have a higher risk of recurrent dissection when associated with FMD (70).
Prognosis of patients with extracranial FMD

Management
The poor knowledge of the natural history and the lack of randomised trials that compared the different treatment options do not allow any satisfactory judgement to be made regarding the need for or the efficacy of any treatment. In patients who had an ischaemic event, antithrombotic drugs are generally used, although their efficacy has never been demonstrated in this particular context. A variety of surgical options have been proposed. The most commonly used was graduated or balloon intraluminal dilatation either isolated or associated with resection–anastomosis, endarterectomy, or other reconstructive techniques (71). The perioperative risks of surgery seem to below (Table 4) and anatomical results are maintained in the long term. It has been suggested that patients with symptomatic FMD, accessible lesions, and low operative risks would be good surgical candidates (72), but this assumption is not based on strong evidence, and most of the techniques are no longer available. Despite recent advances in interventional radiology techniques including percutaneous angioplasty and stenting, there are still only very few reports of patients treated with these techniques, most often without complications (72–77). Percutaneous angioplasty–stenting is nevertheless currently considered as a reasonable treatment option in patients with recurrent symptoms, particularly resulting from haemodynamic impairment, despite medical treatment (2 78). The long-term results of percutaneous angioplasty-stenting are, however, still unknown.
Risk of surgical and endovascular treatments in patients with carotid FMD (series that included <10 patients)
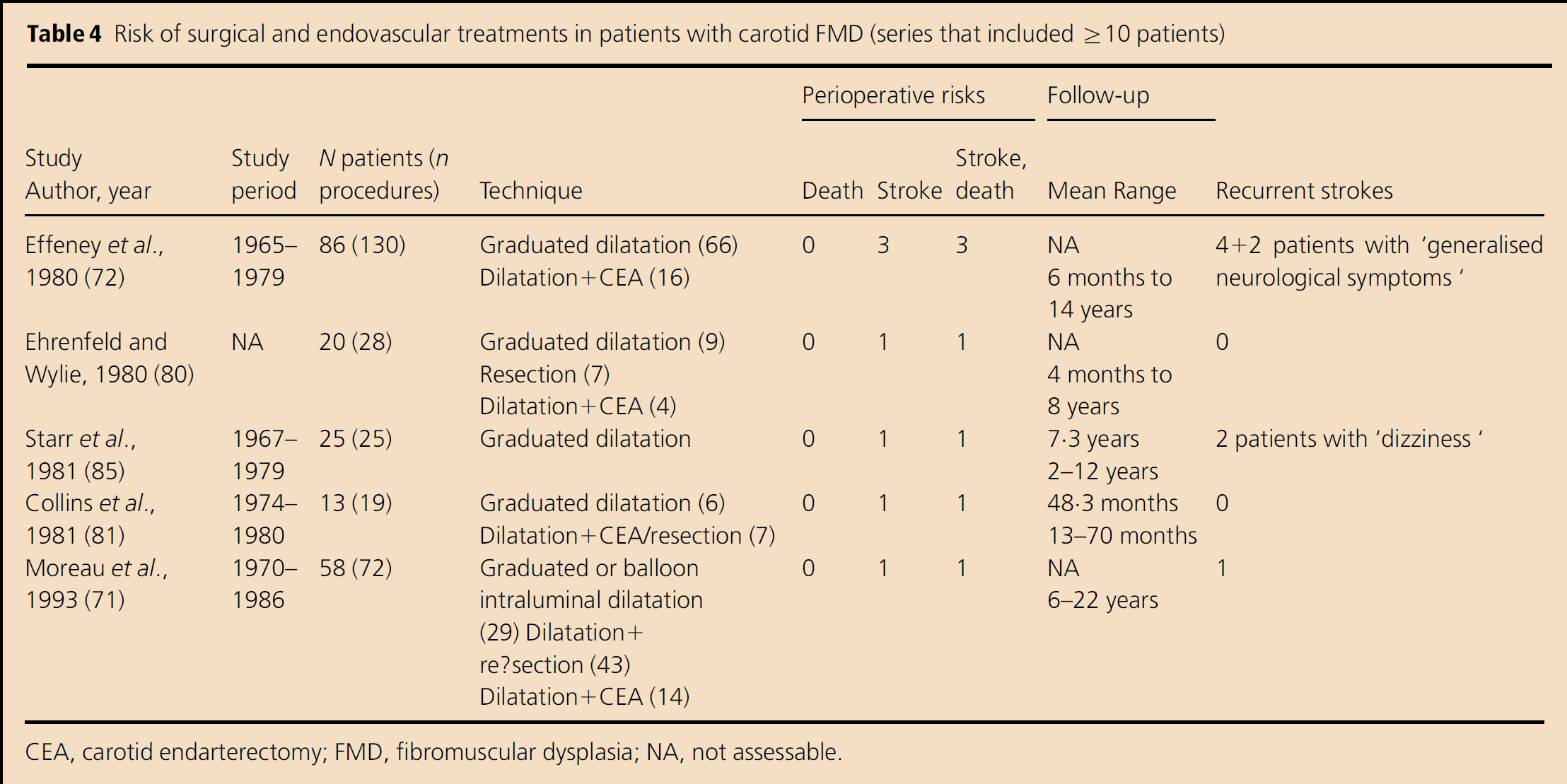
CEA, carotid endarterectomy; FMD, fibromuscular dysplasia; NA, not assessable.
Conclusion and perspectives
Over the past few decades, there have only been limited advancements in the knowledge of FMD of cervical and intracranial arteries. Clinical presentation is very heterogeneous and many patients are paucisymptomatic. Angiographic features are miscellaneous and the disease may remain undiagnosed because angiographic patterns may be atypical or lesions very mild. The major aims of the current research are to unravel the pathophysiological mechanisms of FMD, to assess the risk of disease progression in focal and multifocal FMD, and to define the best treatment options.