
Abstract
Risk factors and a high stroke mortality rate are a heavy stroke burden on Central and
Eastern European countries. The 1995 Helsingborg Declaration outlined the aim of the
coming decade was to improve patient care. In Poland it led to the foundation of the
National Stroke Prevention and Treatment Programme, (1998-2008) which later became part of
the National Cardiovascular Disease Prevention and Treatment Programme. The aim: Improve acute and postacute management Implement innovative therapies Develop poststroke rehabilitation, and Monitor epidemiology.
Establishing and equipping stroke units has raised their number from three to 111. Thrombolysis for stroke and carotid angioplasty and stenting procedures were supported and supervised. The needs in poststroke rehabilitation were assessed and services have improved due to the support of the programme. Continuous monitoring of patient care proved that the mortality and disability rates have decreased and the quality of treatment has improved.
Stroke epidemiological data provided by the World Health Organization (WHO) from the 1970s and 1980s showed that mortality and early stroke fatality in Central and Eastern Europe is exceedingly high compared with other countries of the continent (1). It was confirmed by a Polish prospective study carried out in the years 1991–1992 (2). There was an urging need for change in management and prevention of stroke, which would allow reducing individual and social burden.
The Helsingborg Declaration (1995) aimed at examining evidence-based knowledge in stroke and set aims for the next decade in organisation of care and research in Europe (3). Significant discrepancies were found between the Helsingborg Declaration and the everyday situation in Poland. Leaders in the field of Neurology and the Polish Ministry of Health took initiative and established the National Stroke Prevention and Treatment Programme (NPPiLUM) in 1998. The outcome was to achieve the aims outlined in Helsingborg. In 2003, the programme was incorporated into the National Cardiovascular Disease Prevention and Treatment Programme (POLKARD) and continued until the end of 2008 in its initial form.
The strategic goals were to recognise and monitor stroke epidemiology and care lower stroke incidence by implementing effective primary and secondary
prevention, and improve medical care in the acute stage and poststroke care.
Monitoring of stroke care was an issue primarily due to the high mortality rate and significant differences in distribution of risk factors, in-hospital care and death, and poor outcome [modified Rankin score (mRS) of three or more] rates within Poland (4).
Three registries 2001/2002, 2004/2005, and 2007/2008 showed a significant drop in mortality and poor outcome rates. This is suspected to be a result of increasing stroke unit care, earlier admission to hospital, improvement in application of evidence-based treatments (for acute stage and prevention), and education of medical staff and population.
A stroke unit network as a basis for effective stroke therapy was a major concern. In 1998, Poland had three stroke units and calculated that the countrywide needs were 120 units (as a part of neurological departments). A grading system based on the European Stroke Initiative (EUSI) guidelines comprising of four categories was introduced in order to monitor the development of the network on the basis of neurological departments (5–7).
The categories were: A – stroke units fulfilling the criteria of the NPPiLUM and
EUSI B – stroke units conditionally fulfilling criteria C – stroke units only by name, and neurological departments without a stroke unit.
We have also distinguished a supreme category of comprehensive stroke unit with on site availability of interventional neuroradiology, neurosurgery, and 24/7 availability of magnetic resonance imaging (MRI).
The stroke programmes support the purchase of appropriate equipment (e.g. cardiac monitors, defibrillators, ECG, infusion pumps, beds, wheelchairs, etc.). Three stroke units increased to 97 in 2003, and 111 in 2007 (Fig. 1).
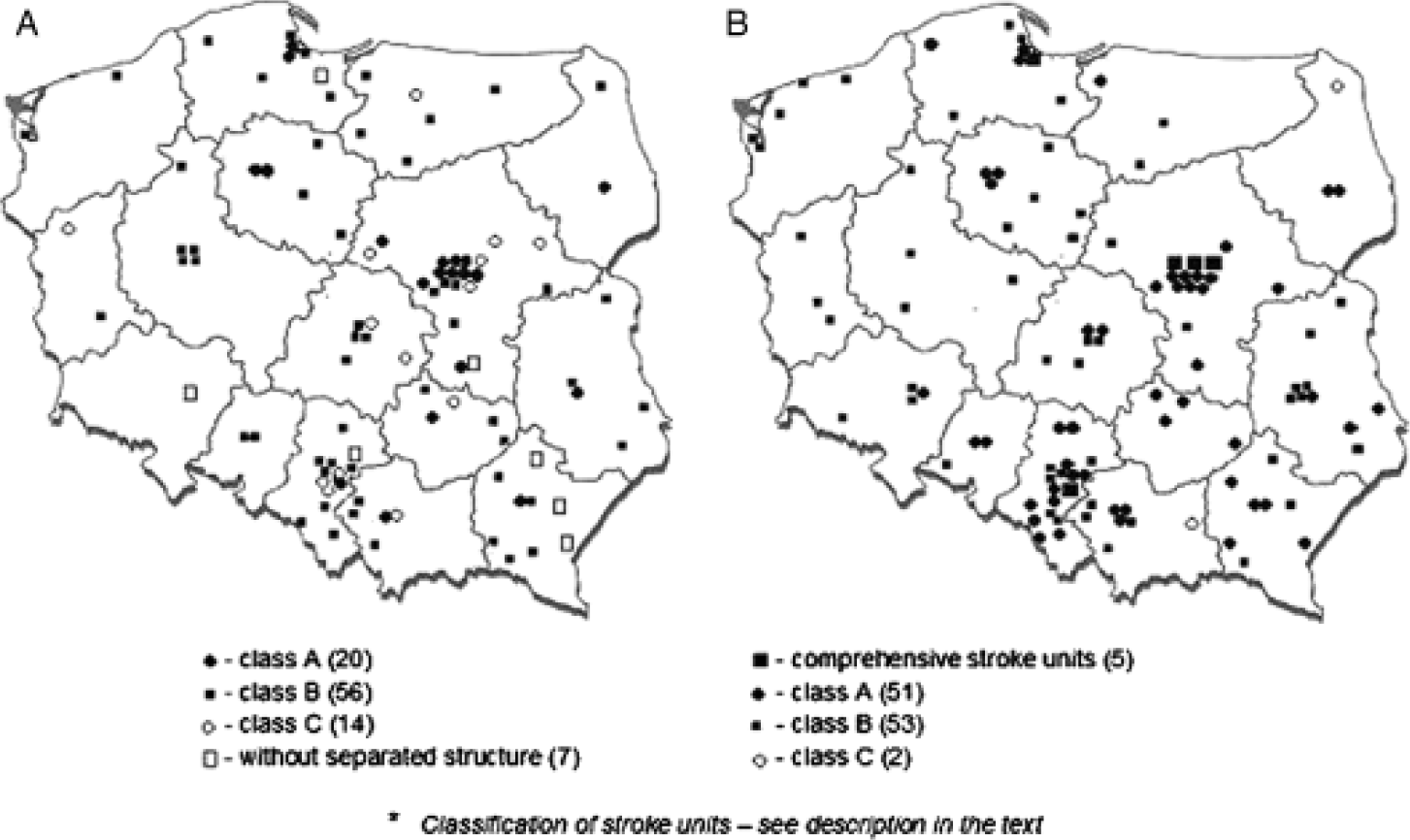
The development of stroke units in Poland: the situation in 2003 – 97 stroke units (a) and 2007 – 111 stroke units (b).
The implementation of innovative and evidence-based treatments in stroke was another aim of the stroke programmes in Poland. The number of in-patients receiving in hospital aspirin, statins and antihypertensive drugs, and oral anticoagulants at discharge increased. Fewer patients received so-called ‘neuroprotective or vasoactive drugs’ (e.g. piracetam, steroids, mannitol, vinpocetine), which were previously very widely used in the nineties. Thrombolysis, approved conditionally in 2003 in Poland was reimbursed by POLKARD until the end of 2008. Over a 6-year period <1100 patients were treated.
There were two concurrent registries of thrombolysis: Thrombolysis in Ischemic Stroke sponsored by POLKARD and SITS (Safe Implementation of Thrombolysis in Stroke), which is still ongoing as SITS-EAST and is now sponsored by the European Union (EU) Public Health Executive Authority. The results of the SITS Poland registry have been compared with the results of the SITS Monitoring Study performed in the ‘old’ countries of the EU (8). A higher mortality rate was noted, but without an effect on independence 3-months poststroke. Polish patients also had longer onset and door-to-needle times. These findings imply that further monitoring is required within the SITS-EAST project.
From 2003 to 2005, POLKARD supported carotid angioplasty and stenting procedures. Four hundred and twenty procedures were reimbursed and monitored. The perioperative complication rate was 10%, which complied with the results of large clinical trials (9).
Poststroke rehabilitation is a great matter of concern in Poland. In the 1990s, approximately 1% of stroke victims had access to early poststroke rehabilitation (10). Financial resources had to be dedicated to develop new rehabilitation units.
In order to assess the current status and needs, rehabilitation units performing early
poststroke rehabilitation were categorised into five classes from A to E. The categories were:
Class A – comprehensive rehabilitation: physiotherapy – minimum 60 min/day speech therapy – minimum 30 min, 5-days a week rehabilitation of other cognitive impairments - minimum 30 min, 5-days a
week group physiotherapy. Class B – having possibility of all types of therapy, but is done less
frequently Class C – physiotherapy and speech therapy Class D – physiotherapy and rehabilitation of other cognitive
impairments Class E – physiotherapy.
The stroke programmes justify the purchase of rehabilitation appropriate equipment (e.g. ergometres, treadmills, traction tables, tilt tables, computed rehabilitation programmes for neuropsychological rehabilitation, rehabilitation beds, wheelchairs, etc.). We started with 11 class A rehabilitation units in 2004, and activated 17 by 2008. The development of units providing early comprehensive poststroke rehabilitation from 2004 to 2008 is marked, but still insufficient (Fig. 2). The number of beds required to cover the needs in early poststroke rehabilitation is 763. In 2004, there were only 159 (20.8% of needs) (11) and in 2008, there were only 294 (38.5%).
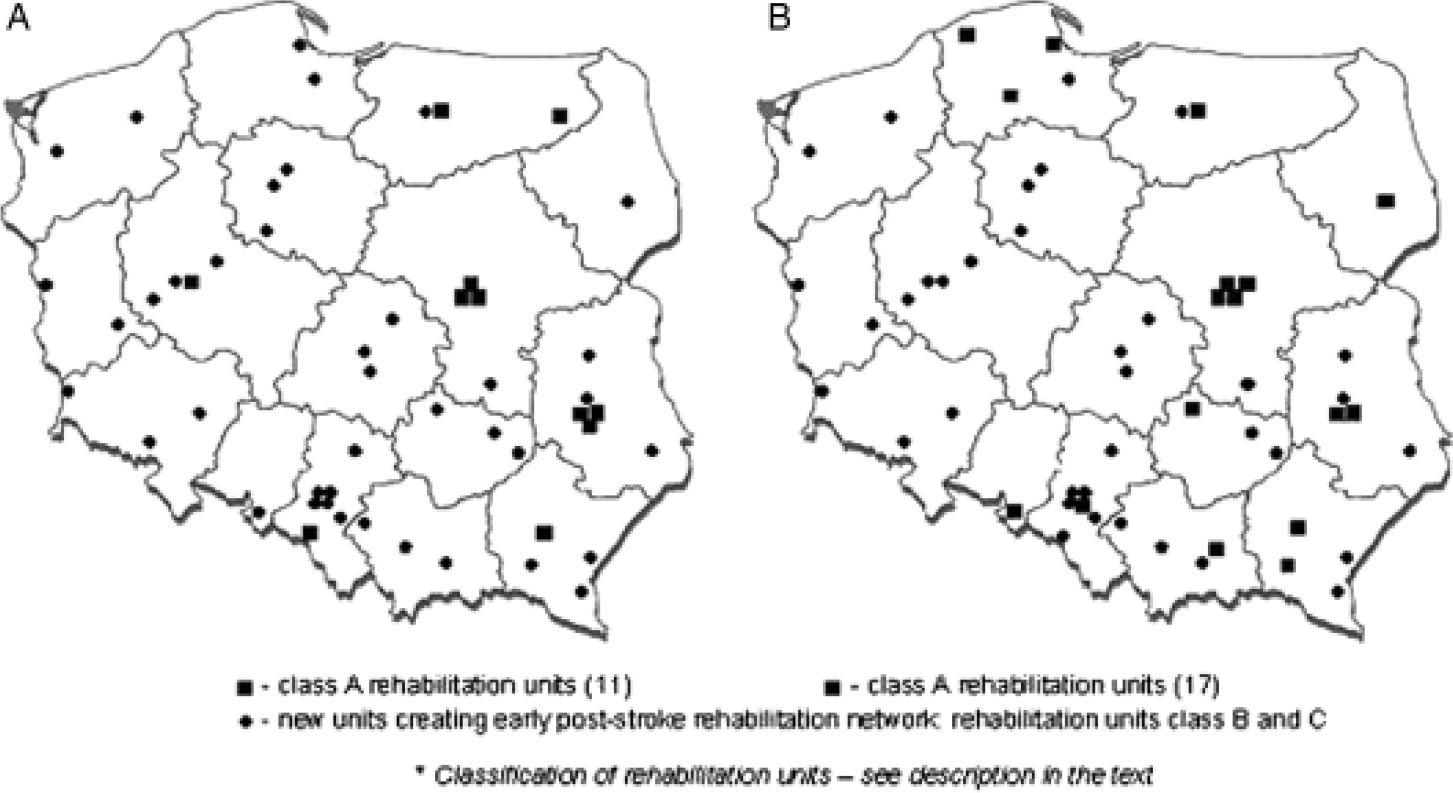
Rehabilitation units conducting comprehensive post-stroke rehabilitation in 2004 (a) and in 2008 (b) and the needs in poststroke rehabilitation.
Over the last 10-years we prepared several guidelines for stroke prevention, treatment, and organisation of care, which we systematically updated. The last edition was published in 2008 (12). We organised many teaching courses for physicians, nurses, physiotherapists, neuropsychologists, and also published many information leaflets about stroke for lay people.
Stroke programmes in Poland have positively influenced stroke treatment organisation. This is an example for other countries (Fig. 3).

POLKARD Executive Committee meeting in 2007 (standing from left: Ryglewicz D., Krawczyk M., Paprot E., Opolski G., Skowroñska M., Członkowska A., Zdrojewski T., Niewada M., and lower row – Kobayashi A.).
These developments would have progressed without support, but the rate of improvement would have been much slower.
Despite the achievements there are still problems to be solved like, developing comprehensive stroke centres with interventional neuroradiology, wider safer and more effective implementation of thrombolysis, and improving and increasing the number of rehabilitation facilities.
Acknowledgements
The authors would like to thank all experts who were working in years 1998–2008 in both stroke programmes (Drozdowski W., Gasecki D., Hertmanowska H., Klimek A., Kochanowski J., Kozubski W., Krawczyk M., Kuczyñska-Zardzewiały A., Kwieciñski H., Kwolek A., Mazur R., Milewska D., Nowacki P., Nyka W. M., Opala G., Opara J., Pierzchała K., Rożniecki J., Ryglewicz D., Seniów J., Słowik A., Stelmasiak Z., Stroiñska-Kuś B., Szczepañska-Szerej A., Szczudlik A., Ṥwiat M., Wiszniewska M.), and all centres in Poland who participated in stroke units and rehabilitation registries.