
Abstract

In their recent excellent review, Mattle et al. (1) highlight the epidemiological evidence that stroke is more common among patients with PFO, particularly if they have other features such as atrial septal aneurysm, Eustachian valve, a high degree of right-to-left shunting and hypercoagulable states.
However, for many physicians, particularly, it seems, my Cardiology colleagues, there remains a great deal of scepticism regarding the causal relationship between PFO and stroke. As ∼25% of the population has a PFO, the mere association of PFO and stroke does not establish the diagnosis of paradoxical embolism.
Besides the imaging features identified by Mattle et al., we reported in 2008 (2) that there are a number of clinical clues to paradoxical embolism. The table lists a number of features of the presentation of stroke that should raise the suspicion of paradoxical embolism. In our experience, paradoxical embolism accounts for 5.5% of new presentations with TIA or minor stroke; among younger patients without hypertension, atherosclerosis or other usual causes of stroke, the proportion is higher. In patients with truly cryptogenic stroke who present with the clues listed in Table 1, the index of suspicion for paradoxical embolism should be high.
Clinical clues to paradoxical embolism
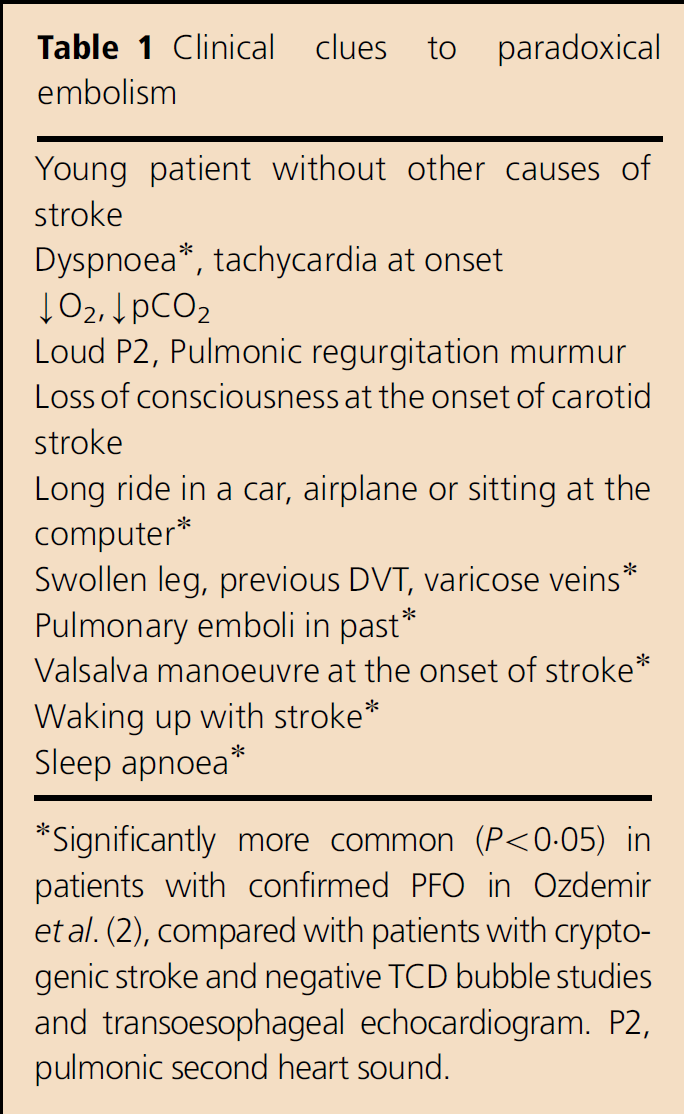
Significantly more common (P<0.05) in patients with confirmed PFO in Ozdemir et al. (2), compared with patients with cryptogenic stroke and negative TCD bubble studies and transoesophageal echocardiogram. P2, pulmonic second heart sound.