
Abstract
Background
Healthcare-associated infections are a major cause for worsening in ischaemic stroke patients. In addition to increased morbidity and mortality, healthcare-associated infections also result in a potentially preventable increase in economic costs.
Aims
The aim of this study was to identify healthcare-associated infection incidence in ischaemic stroke patients in Japanese hospitals, and to conduct a risk-adjusted analysis of the associated economic and clinical outcomes.
Methods
Healthcare-associated infections were identified in 36 Japanese hospitals using an administrative database. Identification was carried out using a combination of International Classification of Diseases-10 codes and antibiotic utilisation patterns that indicated the presence of an infection. Risk-adjusted hospital charges and length of stay were calculated using multiple linear regression analyses correcting for patient and hospital factors. A logistic regression model was used to analyse the association between healthcare-associated infection infection and mortality.
Results
There was an overall healthcare-associated infection incidence of 16·4 %, with an interhospital range of 4·7–28·3%. After risk-adjustment, infected cases paid an additional US$3 067 per admission (interhospital range US$434–US$7 151) and were hospitalised for an additional 16·3-days (interhospital range: 5·1–25·1-days) when compared with uninfected patients. Healthcare-associated infections also had a strongly significant association with increased mortality (odds ratio=23·2, 95% confidence intervals: 12·5–43·2).
Conclusions
We observed a wide range of healthcare-associated infection incidence between the hospitals. Healthcare-associated infections were found to be significantly associated with increased hospital charges, length of stay, and mortality. Furthermore, the use of risk-adjusted multi-institutional comparisons allowed us to analyse individual performance levels in both infection and cost control.
Introduction
Healthcare-associated infections (HAIs) have been identified previously as having a significant impact in the worsening of ischaemic stroke patients (1–4). In addition to increased morbidity and mortality, the resulting extension in hospital stay results in increased costs to patients and third party payers, as well as a reduction in potential bed-space for healthcare providers.
The HAIs have been estimated to develop in over one-third of patients with acute stroke, with the most common infections being lung infections and urinary tract infections (1, 2). Studies have reported HAI incidences of 41·5% (5), stroke-associated pneumonia incidences ranging from 10% to 30·9% (3, 4, 6–8), and even incidences of significant bacteriuria alone reaching 39·1% (9). Reported extensions in length of hospital stay ranged from six-days (6) to 23-days (7). Risk factors found to be associated with HAIs in stroke patients have include mechanical ventilation, dysphagia, age, parenteral nutrition, poststroke disability, and urinary catheterisation (6, 10, 11). In addition, the Barthel index has been shown to be significantly associated with infections in acute ischaemic stroke patients (12, 13).
Quantifying the increases in hospital charges and length of stay (LOS) associated with HAIs would be useful for healthcare providers and third party payers when considering the cost-effectiveness of interventions aimed at reducing HAIs. While some studies have attempted to quantify the outcomes associated with HAIs in stroke patients at the hospital level (6, 7), a multi-institutional analysis that takes into account patient and hospital-related variations would allow for a more meaningful interpretation of each hospital's results.
There are currently no studies to our knowledge that have analysed HAI incidence in stroke patients in Japanese hospitals, and no studies that have attempted to quantify the economic impact and mortality associated with HAIs at a multiinstitutional level.
Aims
The objective of this study was to utilise an administrative database from multiple Japanese hospitals in order to identify HAI incidence in patients admitted for acute ischaemic stroke, and to quantify risk-adjusted economic and clinical outcomes associated with HAIs.
Methods
Hospital and patient selection
The original sample population consisted of 16 886 ischaemic stroke patients admitted during the period of April 1998 to April 2008 into 40 general hospitals (designated H1–H40) enrolled in the Quality Indicator/Improvement Project (QIP), a database of Japanese hospitals that consists of clinical and claims data. Hospitals in the QIP voluntarily join the project and provide claims and administrative data in standardised formats for analysis with the objective of improving the quality and efficiency of healthcare provision. The hospitals included in this study were drawn from this database and represent a variety of public and private, teaching, and nonteaching hospitals with different casemixes and specialties.
Clinical diagnoses were identified using International Classification of Diseases (ICD)-10 codes. Preexisting comorbidity conditions were analysed using the Charlson comorbidity index (Dartmouth–Manitoba version) (14, 15).
Patients who had infections occurring within 48 h were identified as having community-acquired infections and thus excluded from this study. Other exclusion criteria included minors (below 20-years), and cases with missing data in charge information, age, and Japan Coma Scale (JCS) (16) score. For the linear regression models used for hospital charges and LOS, and the logistic regression model used for mortality, cases with standardised residuals >3 standard deviations from the mean were considered outliers and excluded from analysis. In the regression models for hospital charges and LOS, patients who died during the hospitalisation period were also excluded.
The JCS is the most widely used clinical tool for evaluating consciousness level in Japanese emergency care, and consists of a scale categorised into four levels: (i) alert; (ii) JCS levels 1–3 (disoriented: awake without stimulation); (iii) JCS levels 10–30 (somnolent: arousable only in the presence of stimulation); and (iv) JCS levels 100–300 (comatose: unarousable despite stimulation) (17).
HAI identification
The HAIs were first identified using hospital-reported ICD-10 codes adapted from the Pennsylvania Health Care Cost Containment Council (PHC4) (18). However, previous studies have shown that the use of ICD codes alone is insufficient for HAI identification (18, 19). Therefore, HAIs were also identified through the use of antibiotic utilisation patterns obtained from daily drug claims data, based on a technique adapted from our previous study (20).
Infections were identified where antibiotic utilisation did not conform to surgical prophylaxis patterns in patients who had surgeries performed. Patients were identified as having HAIs if, in addition to reported ICD codes, they fell into any of the following categories: (1) antibiotic utilisation episodes with durations of four or more days that did not overlap a day in which surgery requiring prophylaxis was performed; (2) three or more antibiotic types used within a single episode of antibiotic utilisation; (3) antibiotic types changed or a second antibiotic type added midway during an antibiotic utilisation episode; (4) prophylactic antibiotic utilisation episodes of five or more days in which the start of the episode corresponds to a day where surgery was performed.
Clinical and economic outcome indicators
Total hospital charges and LOS (days) were used as indicators for economic outcome, while mortality was used as the clinical outcome measure.
Statistical analysis
Analyses were performed using
Risk adjustment
Total hospital charges and LOS were natural logarithmically transformed before used as dependent variables in multiple linear regression analysis (stepwise). Two models were developed for each dependent variable; one in which hospital stratification was included in the independent variables, and another in which hospital stratification was excluded. The former was used to calculate overall risk-adjusted hospital charges and LOS after taking hospital variations into account. The latter model was used in the calculation of hospital-level risk-adjusted hospital charges and LOS, which enabled interhospital comparisons.
The models for hospital charges included the following independent variables: age, gender, Barthel index, atherothrombotic stroke, cardioembolic stroke; Charlson score, LOS, surgeries performed, central venous catheter (CVC) use, mechanical ventilation, dysphagia, ICU stay, and JCS score upon admission. The models for LOS included the following independent variables: age, gender, Barthel index, atherothrombotic stroke, cardioembolic stroke; Charlson score, surgeries performed, CVC use, mechanical ventilation, dysphagia, ICU stay, and JCS score upon admission. The first model for each dependent variable also included hospital stratification while the second model did not. Apart from atherothrombotic and cardioembolic strokes, patients with other types of stroke were used as a reference for the regression models. The Barthel index used by the hospitals in this sample was the 20-point Collin scoring version (21).
Exponentials of the predicted values from the regression models were calculated in order to obtain expected values in units of Japanese Yen and days, and Duan's smearing coefficient (22, 23) was applied to correct for retransformation bias. Risk adjustment was then conducted by dividing each hospital's mean observed value by the mean expected value, and the result was multiplied by the mean value of the entire dataset. Final estimates of hospital charges were adjusted for inflation using the Japanese consumer price index (adjusting all values to the 2008 yen value) and then converted to US dollars using Purchasing Power Parities (JPN 100 Yen=US$0·80 (21)).
Mortality was used as the dependent variable in the logistic regression model, and adjusted with the following independent variables: HAI status, age, gender, Barthel index, atherothrombotic stroke, cardioembolic stroke; Charlson score, surgeries performed, CVC use, mechanical ventilation, dysphagia, ICU stay, LOS, JCS score upon admission, and hospital stratification. Calibration was evaluated with a Hosmer–Lemeshow statistical analysis (24), while discrimination was evaluated with a receiver operating characteristic (ROC) curve.
Results
Patient and hospital characteristics
After excluding cases that fulfilled the aforementioned exclusion criteria, our final sample for analysis consisted of 8 861 patients from 36 hospitals, with four hospitals excluded due to a lack of patients.
General characteristics of the patients in our sample are shown in Table 1. Elderly patients were heavily represented in the study population, with almost half of the patients older than 75-years of age. There were more men than women at 58·3% vs. 41·7%. Of the patients in our sample, 68% were originally admitted to either neurosurgery or neurology departments, 17·3% were admitted to internal medicine departments, and the remainder in various other departments. The Barthel index showed that upon admission, 20·1% of the patients had no form of disabilities, while 43·3% had relatively severe disabilities. Over 21% of the patients were classified as having an atherothrombotic stroke 10·3% of the patients had a cardioembolic stroke, and 68·5% had strokes that did not fall into either of the above two categories. Almost 70% of the patients were completely lucid upon admission according to the JCS, and more than half were admitted without existing comorbidities. Unadjusted mean hospital charges were US$6 471, with a mean LOS of 21·97-days.
Patient characteristics and pre-risk-adjusted total hospital charges and length of stay (N=8 861)
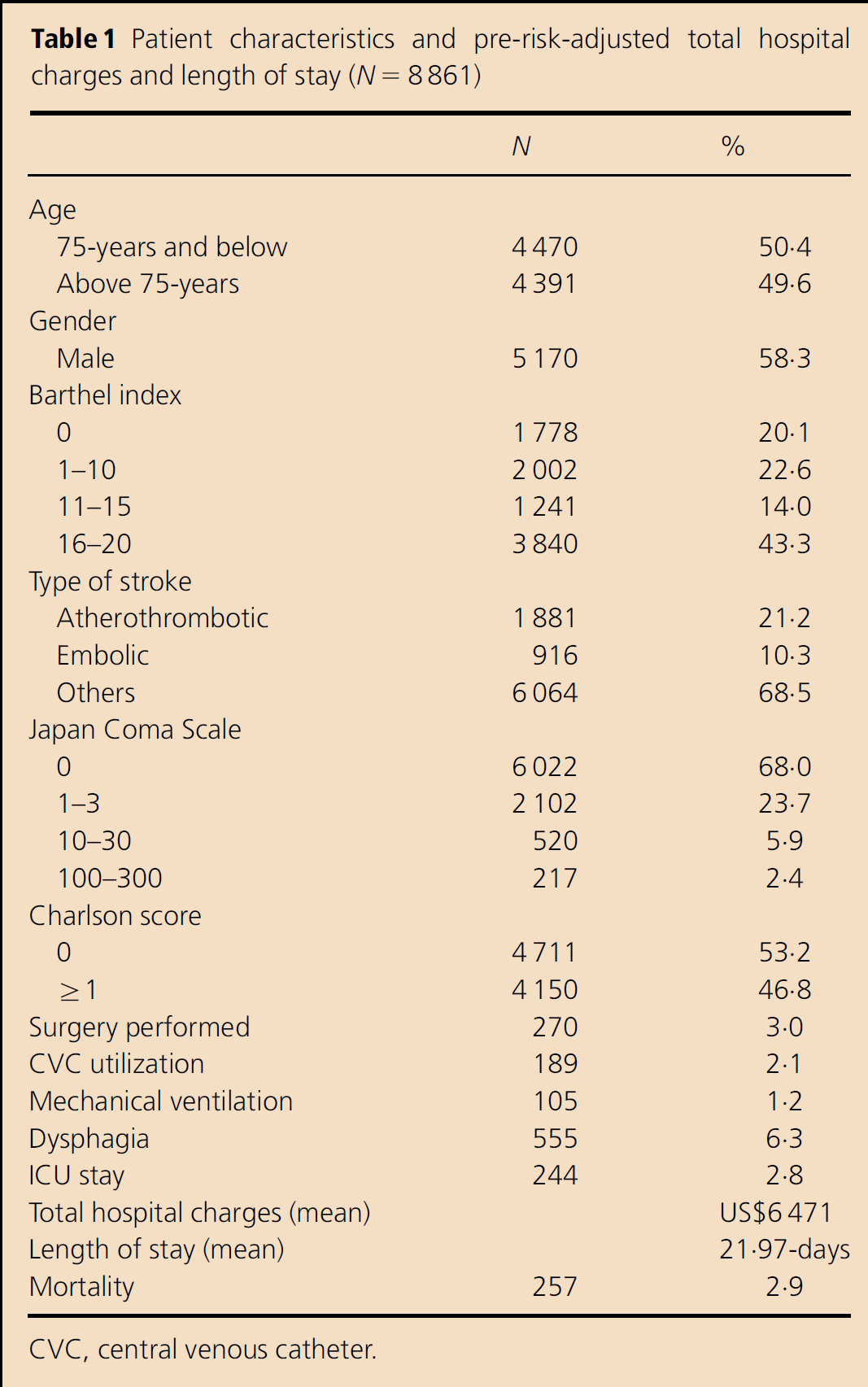
CVC, central venous catheter.
The hospitals in our sample consisted of general hospitals providing a range of services not limited to stroke care. Of the 36 hospitals, 27 were privately owned and nine were publicly owned. Twenty-nine of the hospitals were teaching hospitals, while seven of the hospitals were not. The hospitals had a mean of 435 beds, with an interhospital range of 98–1 125 beds. More than half of the hospitals had ICUs, but only two of the hospitals had dedicated stroke care units. There was a mean of 98 doctors (range: 9–392) and 337 nurses (range: 45–1 138) in each hospital. Fourteen of the 36 hospitals in our sample had both neurosurgery and neurology departments, 15 hospitals had only one of the two departments, and seven hospitals had neither (in which case stroke patients were warded in internal medicine or other departments).
HAI incidence
The overall HAI incidence in our sample was 16·4%. As seen in Fig. 1, there was a large variation of HAI incidence at the hospital level, with a range from 4·7% to 28·3%. Seventeen of the 36 hospitals had HAI incidence proportions lower than the overall mean.
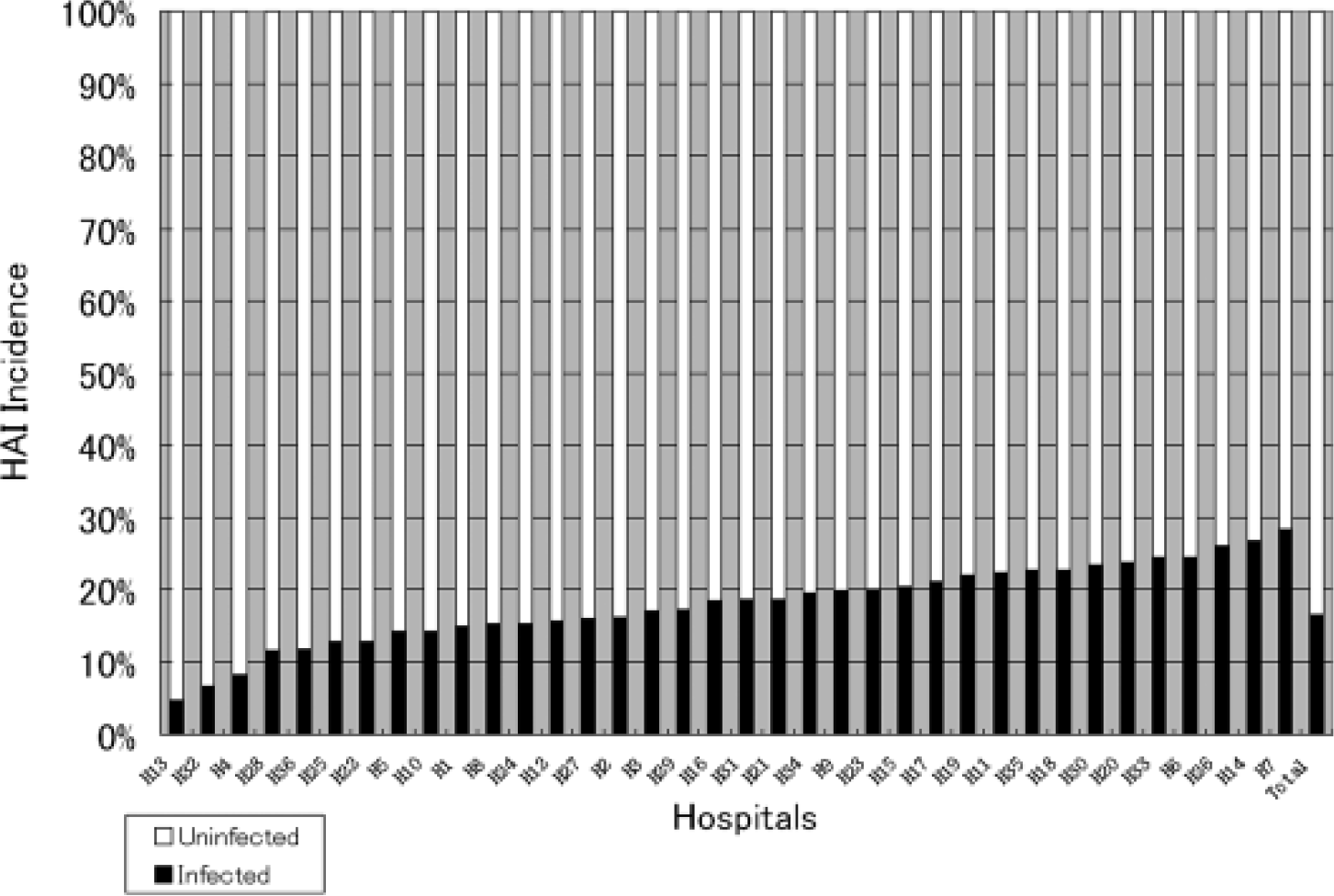
Healthcare-associated infection (HAI) incidence at hospital level and in total.
Risk-adjusted hospital charges and LOS
The results of the linear regression analyses are shown in Table 2. The first model for both hospital charges and LOS (as dependent variables) included hospital stratification, while the second model excluded hospitals as independent variables. Tests for multicollinearity were performed and all variance inflation factors values were found to be below 2·1 (data not shown).
Results of multiple linear regression models with hospital charges and length of stay as dependent variables, and a logistic regression model using mortality as the dependent variable
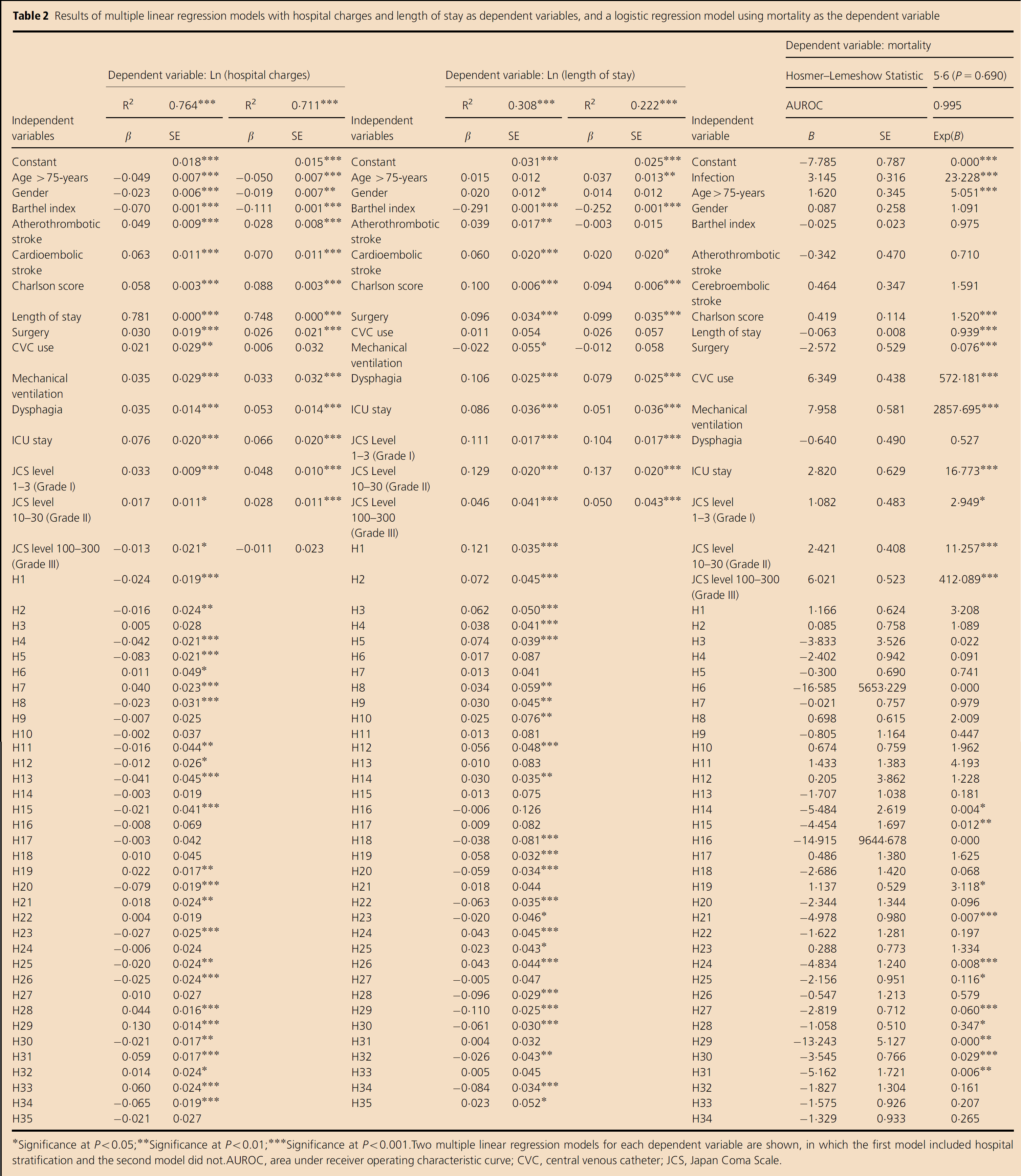
Significance at P<0.05;
Significance at P<0.01;
Significance at P<0.001.
Two multiple linear regression models for each dependent variable are shown, in which the first model included hospital stratification and the second model did not.
AUROC, area under receiver operating characteristic curve; CVC, central venous catheter; JCS, Japan Coma Scale.
With regard to hospital charges, the first model had an R2 value of 0·764 (P<0·001). Independent variables which showed significant association with hospital charges included age, gender, Barthel index, both types of stroke, Charlson score, LOS, surgery, CVC use, mechanical ventilation, dysphagia, ICU stay, all JCS levels, and 25 hospitals. Length of stay showed the strongest association with increased hospital charges (β=0·781; P<0·001). All independent variables in the second model (R2=0·711; P<0·001) except for CVC use and JCS levels 100–300 showed significant associations with hospital charges.
The first model for LOS (R2=0·308; P<0·001) showed that gender, Barthel index, both types of stroke, Charlson score, surgery, mechanical ventilation, dysphagia, ICU stay, all JCS levels, and 24 hospitals had significant associations with increased LOS. Mechanical ventilation, CVC use and JCS levels 100–300 had the highest standardised coefficients among the independent variables. In the second model, (R2=0·222; P<0·001), gender, atherothrombotic stroke, CVC use, and mechanical ventilation showed no significant association with increased LOS.
After conducting risk-adjustment based on data from the first model, the overall mean hospital charges were US$6 009 for uninfected patients and US$9 076 for infected patients, resulting in an additional US$3 067 associated with HAIs. Length of stay after risk-adjustment was 19·0-days in uninfected patients and 35·3-days in infected patients, with an additional 16·3-day increase associated with HAIs. Mean hospital charges per day for uninfected and infected patients were thus US$317 and US$257, respectively.
Using data from the second model for both hospital charges and LOS, risk-adjustment was calculated at the hospital level. Figure 2 shows box-plot graphs of the risk-adjusted hospital charges and LOS for uninfected patients and infected patients by hospital.
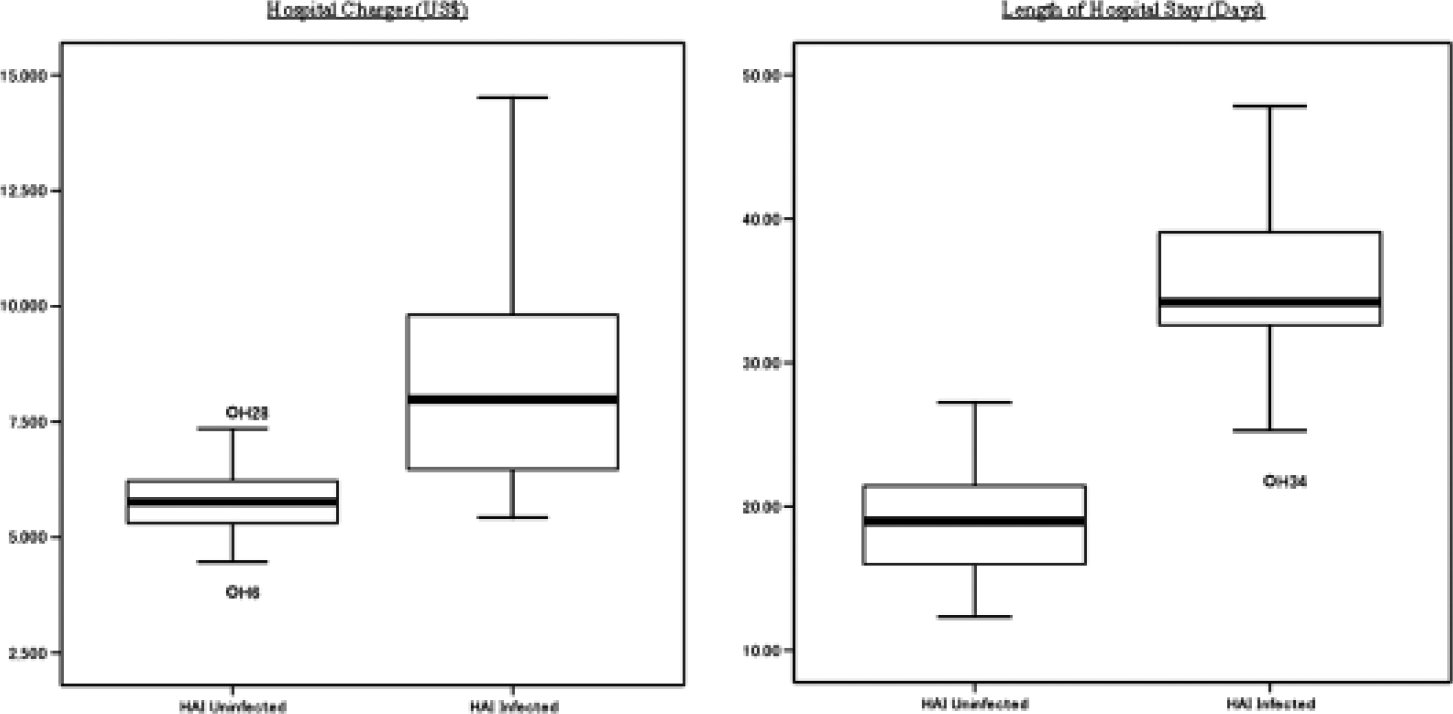
Box-plot graphs of risk-adjusted hospital charges per admission (in US$) and length of stay (in days) for infected and uninfected patients at the hospital level. HAI, healthcare-associated infection.
After risk-adjustment, there was a hospital-level range of US$3 824 (Hospital H6) to US$7 710 (Hospital H28) for hospital charges in uninfected patients. For infected patients, this range was US$5 438 (Hospital H6) and US$14 505 (Hospital H24). Therefore, additional charges associated with HAIs ranged from US$434 to as high as US$7 151 at the hospital level. The 25th, 50th, and 75th percentile hospital charges for the uninfected patients were US$5 305, US$5 764, and US$6 232, respectively. The 25th, 50th, and 75th percentile hospital charges for infected patients were US$6 379, US$7 983, and US$9 865, respectively. Hospitals H6 and H28 were identified as outliers with inordinately low and high hospital charges, respectively, for uninfected patients.
At the hospital level, the minimum risk-adjusted LOS for uninfected patients was 12·3-days (Hospital H34) and the maximum LOS was 27·2-days (Hospital H1). The 25th, 50th, and 75th percentiles for the uninfected patients were 15·9, 19·0, and 21·4-days, respectively. For patients who had an HAI, the risk-adjusted LOS ranged from 21·8-days (Hospital H34) to 47·9-days (Hospital H8). The 25th, 50th, and 75th percentiles for infected patients were 32·6, 34·2, and 41·7-days, respectively. Additional LOS associated with HAIs ranged from 5·1-days (Hospital H4) to 25·1-days (Hospital H8). Hospital H34 was identified as an outlier with exceptionally low LOS in infected patients.
Risk-adjusted mortality
After adjusting for patient and hospital variations, the adjusted odds ratio for the association of HAIs and mortality was 23·2 (P<0·001; 95% confidence interval: 12·5–43·2). The area under the ROC was calculated to be 0·995, while the Hosmer–Lemeshow statistic had a χ2-value of 5·6 (P=0·69). Healthcare-associated infection status, age, Charlson score, LOS, surgery, CVC use, mechanical ventilation, ICU stay, JCS levels 1–3, and JCS levels 10–30 were all positively associated with increased mortality.
Discussion
In this study, we identified HAI incidence in ischaemic stroke patients from 36 Japanese hospitals, and conducted a multi-institutional analysis of the risk-adjusted economic and clinical outcomes associated with HAIs. Our data showed that 68% of the patients were alert upon admission, which was slightly less than the 74·8% reported in 2004 by Kimura et al. (25).
The HAI incidence observed in our study (16·4%; range: 4·7–28·3%) was fairly similar to infection rates reported in other studies (3–9). We also found significant increases in both overall hospital charges and LOS associated with HAIs. In order to verify the accuracy of our HAI identification method (20), we conducted a validation study using gastrectomy patients. Healthcare-associated infections identified by our method were compared with those identified by chart review. At the current sample size (n=425), there is an 89% level of agreement of between the two methods, and Cohen's κ coefficient is 0·73, which is generally considered as having a ‘substantial agreement’ (26). Sensitivity and specificity are 0·86 and 0·91, respectively, showing a high level of accuracy in identification (unpublished data).
At the hospital level, we observed wide variation between healthcare institutions in both hospital charges and LOS. Hospitals such as H4 maintained a relatively low HAI incidence (8·3%), and also managed to control mean hospital charges for both uninfected and infected patients (US$5 304 and US$6 250, respectively). Hospital H4 also showed the lowest increase in LOS associated with HAIs at 5·1-days.
Hospital H32, on the other hand, had a low HAI incidence at 6·7%. Furthermore, HAIs were associated with an increase of only 13·6-days in LOS in this hospital. Despite this, mean hospital charges, while relatively low for uninfected patients (US$4 922), was one of the most expensive for infected patients at US$11 908. In comparison, Hospital H6 had a lengthy 21·2-days increase in LOS associated with HAI, but had the lowest hospital charges for both uninfected and infected patients (US$3 824 and US$5 438, respectively). Therefore, while the regression models show that LOS had the largest association with hospital charges, it is evident that other factors are also important.
Furthermore, in addition to having a high odds ratio associated with increased mortality, Hospital H28 was one of the most expensive hospitals for both infected and uninfected patients, at US$7 710 and US$12 387, respectively. The mean age of the infected patients was 77-years in this hospital, while that of the uninfected was 70-years, and in general it was the older patients (aged >85-years) that resulted in the longer LOS. This high representation of the elderly may explain the high values observed.
The mean hospital charges per day were found to be slightly higher in uninfected patients (US$317 vs. US$217). This could represent a possible loss of income to hospitals, as infected patients occupy bed-space that could potentially be offered to new patients. With an already lengthy LOS in Japanese acute care hospitals (27), the reduction of unnecessarily protracted LOS would be beneficial to an already strained healthcare system.
The LOS has been an issue with Japanese acute care hospitals, and Japan has the longest mean LOS among the OECD countries (28). However, this may be due in part to acute care hospitals in Japan frequently including rehabilitation and palliative care among the provided services. This mixture of acute, subacute, and chronic healthcare provision may also explain the wide variations that we observed between hospitals in hospital charges, LOS, and mortality.
Dedicated stroke units are a rarity in Japan, despite strong recommendations for the use of such units in the treatment of acute stroke patients published in guidelines in 2004 (29). Most hospitals in Japan manage acute stroke patients in general medical wards, and when intensive care was required, these patients were treated in standard ICUs. Because the patients who have had a stint in the ICU would represent more severe cases who required ICU treatment in addition to baseline stroke treatment, it would therefore be unsurprising for ICU stay to have significant and strong associations with hospital charges, LOS, and mortality, as shown in our regression models.
The HAIs have been previously shown to have positive associations with mortality (30). Our data corroborate these findings, although we observed a stronger association between HAIs and increased mortality. While the clinical complications associated with stroke have been looked previously at (2, 6), most of these studies focused on single-institution databases. The use of a multiinstitutional database in this study helps to increase the generalisability of our results, as well as allow for the interpretation of the results from each individual hospital within the context of other hospitals. Downstream studies could include qualitative studies in which particular characteristics in hospitals with low HAI incidences are identified, as well as elucidating problem areas in hospitals with higher HAI incidences. In this way, the quality of HAI control measures may be increased. Furthermore, the approximate cost-effectiveness of subsequent interventions to reduce infections may benefit from the estimations provided in this study.
The limitations of this study are that the identification method used is unable to specify the types of infections that occurred; therefore, the infections identified in this study would potentially include cases of severe pneumonia together with relatively milder infections. As there were no standard stroke severity scales like the Japan Stroke Scale or the NIH Stroke Scale, we were unable to adjust for severity directly, but instead had to use the Barthel index and JCS as approximate proxies. Also, our database did not include the duration after onset at the time of admission, which may have an effect on the results. A multicentre study in Japan conducted by Kimura et al. (25) has shown that almost 37% of patients were admitted within 3 h of onset, and 73% within 24 h. However, due to database limitations, we were unable to include this variable in our analysis. Finally, the hospitals used in this study are voluntarily part of a programme known as the QIP, in which participating hospitals voluntarily provide data for analysis for the purpose of improving healthcare outcomes. As such, there may be some selection bias involved and the hospitals used in this study may not be indicative of all hospitals in Japan.
Summary
In this study, the use of risk adjustment allows for a more meaningful interpretation of the economic and clinical outcomes from a multicentre database. Quantification of the increases in resource utilisation associated with HAIs allows for more precise policy making and planning for interventions.
Owing to the use of hospital charges, the economic outcomes here may be interpreted as cost estimation from a third party payer perspective, which in an insurance-centric healthcare payment system such as the one existing in Japan, may be highly useful.
With a rapidly ageing population in Japan, diseases such as ischaemic stroke that are usually associated with the aged will become more prominent. This study analyses the incidence and impact of HAIs in stroke patients, and highlights the salient need for interventions for their reduction in Japanese hospitals. Possible interventions could include further hand hygiene practice, dedicated infection control staff, high-risk patient identification, and promoting antimicrobial stewardship protocols.
Footnotes
Acknowledgements
The authors are grateful to the staff at the hospitals that participated in the QIP, and their generosity in allowing the use of their data for this analysis.