
Abstract
Background
An uncontrolled clinical study of the Penumbra™ system showed high rates of recanalisation and relatively poor functional outcomes that were inadequately compared with historic controls. We aimed to compare the findings in Penumbra with intravenous tissue plasminogen activator trials that determined recanalisation (Combined Lysis Of Thrombus in Brain ischaemia using transcranial Ultrasound and Systemic tissue plasminogen activator and Transcranial Ultrasound in Clinical Sonothrombolysis).
Methods
Control patients treated with intravenous tissue plasminogen activator and intermittent ultrasound surveillance had National Institutes of Health Stroke Scale scores >7. The Penumbra trial definition of symptomatic intracranial haemorrhage was used. Revascularisation was defined using thrombolysis in brain ischaemia scores predictive of thrombolysis in myocardial infarction flow grades and compared with thrombolysis in myocardial infarction data from Penumbra. Favourable functional outcomes was defined as a modified Rankin Scale of 0–2.
Results
Pretreatment stroke severity (National Institutes of Health Stroke Scale score) was 17·6 ± 5·2 points in Penumbra patients (n=125) and 16·3 ± 5·3 in controls (n=68; P=0·101). The control group was older compared with Penumbra (68·8 ± 13·4 vs. 63·5 ± 13·5-years; P=0·010). Time-to-treatment initiation was on average 2 h later (2·3 ± 0·6 vs. 4·3 ± 1·5 h; P<0·001) in Penumbra. The rate of any revascularisation after treatment with Penumbra was higher than that following intravenous thrombolysis: 82% (54% thrombolysis in myocardial infarction II and 27% thrombolysis in myocardial infarction III) vs. 40% (25% partial, 15% complete revascularisation), P<0·001. Symptomatic intracranial haemorrhage tended to be higher with Penumbra (11·2% vs. 4·4%; P=0·182, Fisher's exact test). At three-months, mortality with Penumbra was higher (32·8%) than controls (14·1%; P=0·006). Favourable functional outcomes were higher in historic controls (39% vs. 25%; P=0·046).
Conclusions
Despite lower revascularisation rates, patients treated with systemic thrombolysis achieved better functional outcomes likely due to earlier treatment initiation. These data indicate that it is unrealistic to expect primary intraarterial revascularisation to be any better than systemic plasminogen activator within the 3-h time window. Improvements in the speed of delivery and performance of intraarterial reperfusion are needed.
Introduction
The use of intraarterial (IA) reperfusion for acute ischaemic stroke is based on the premise that a catheter-based approach can target large thrombi directly to achieve more complete revascularisation. The development of novel IA technologies is also fostered by the need to accomplish reperfusion as fast as possible.
A clinical study that led to FDA approval under the 510 k mechanism of a novel aspiration thrombectomy device (1) was a prospective clinical registry without concurrent controls. This study showed high rates of recanalisation with the Penumbra™ system and relatively poor functional outcomes three-months after IA intervention. The study design did not require a concurrent control arm and no direct comparisons with intravenous tissue plasminogen activator (IV tPA) for stroke are available. The safety and outcomes of Penumbra were descriptively compared with historic controls from other trials of acute revascularisation therapies (1). In addition, partial and complete revascularisation rates with a Penumbra device were compared with complete recanalisation rates of sonothrombolysis (Table 1) (1) without including partial recanalisation rates in patients treated with ultrasound-enhanced thrombolysis nor any recanalisation rates in patients treated with IV tPA alone.
Comparison of IV tPA and Penumbra data
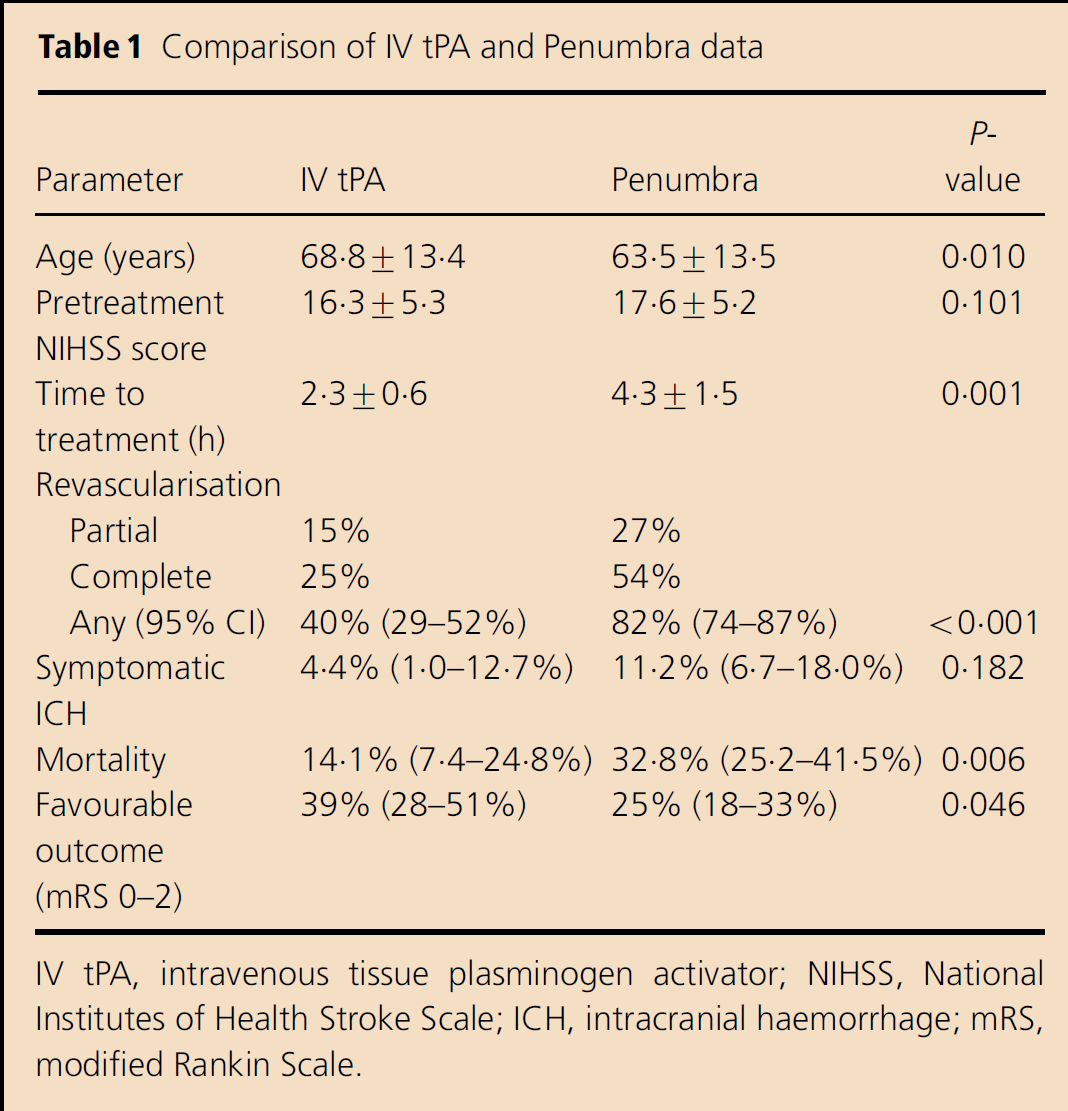
IV tPA, intravenous tissue plasminogen activator; NIHSS, National Institutes of Health Stroke Scale; ICH, intracranial haemorrhage; mRS, modified Rankin Scale.
The only IV tPA trials that provide information about what happens with the middle cerebral artery (MCA) occlusion treated with IV tPA are controlled trials of sonothrombolysis including Combined Lysis Of Thrombus in Brain ischaemia using transcranial Ultrasound and Systemic tPA (CLOTBUST) and Transcranial Ultrasound in Clinical Sonothrombolysis (TUCSON) (2, 3). Patients who were enrolled in the control arm of these two randomised trials were treated with IV tPA as the standard of care within 3 h of symptom onset and received minimal amounts of ultrasound energy with intermittent vessel patency surveillance (4). Therefore, we aimed to analyse recanalisation rates, symptomatic intracranial haemorrhage (sICH), mortality and favourable functional outcome rates between patients enrolled in Penumbra and patients treated with IV tPA.
Subjects and methods
Patients enrolled in Penumbra as well as sonothrombolysis trials had to have evidence of a proximal arterial occlusion in the anterior circulation such as MCA, terminal internal carotid artery (ICA) or tandem ICA/MCA (1–3). In CLOTBUST and TUCSON, all subjects had ultrasound evidence of the pretreatment MCA occlusion such as abnormal thrombolysis in brain ischaemia (TIBI) flow grades (5). Thrombolysis in brain ischaemia flow grades were validated previously against invasive angiography with an excellent (90–100%) agreement particularly for the proximal MCA occlusion location as well as determining partial (Fig. 1) or complete (Fig. 2) recanalisation (5–9).
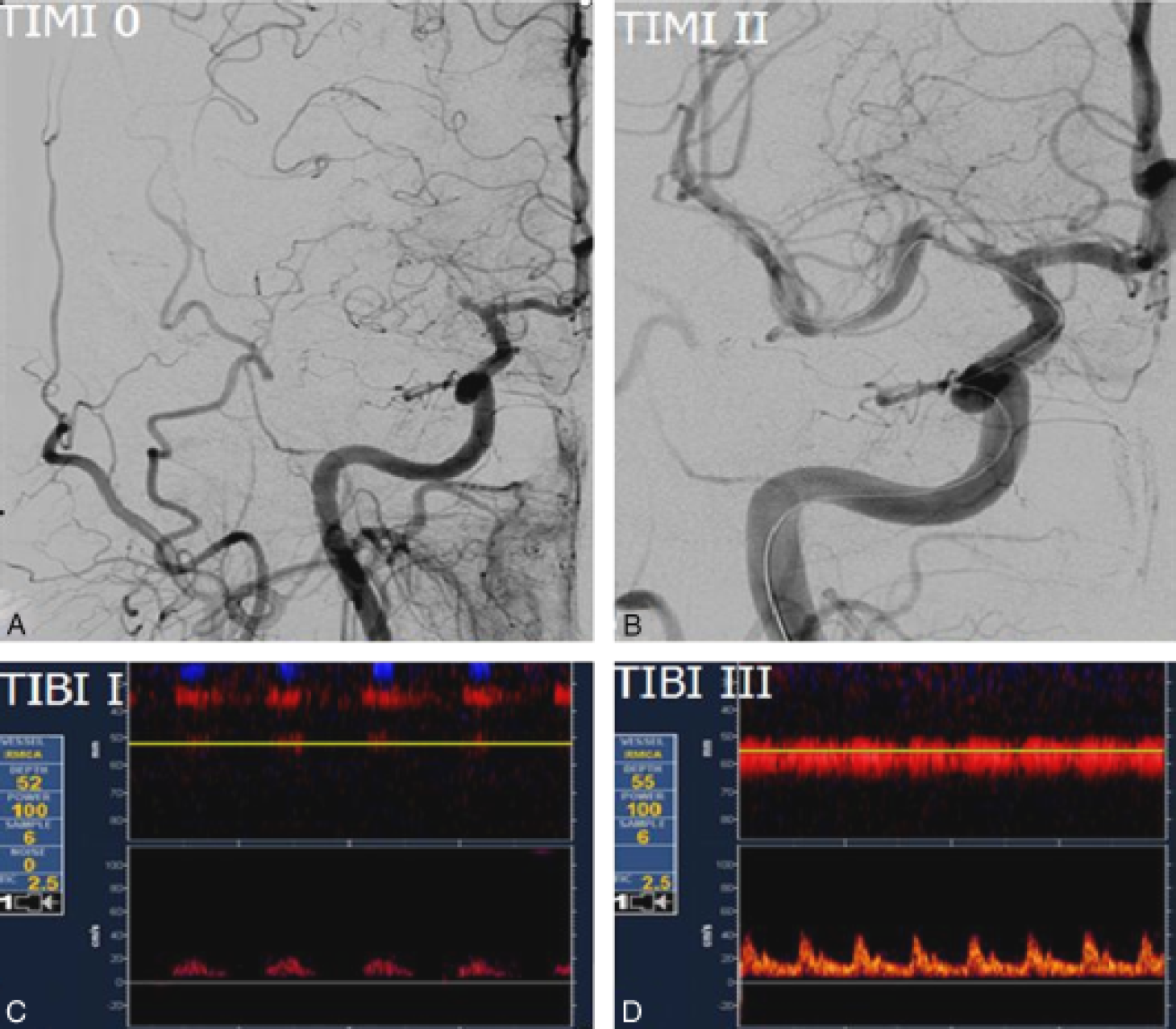
Corresponding TIBI and TIMI grades during partial recanalisation [(c) TIBI I⇒(d) TIBI III and (a) TIMI 0⇒(b) TIMI II]. TIBI, thrombolysis in brain ischaemia; TIMI, thrombolysis in myocardial infarction.
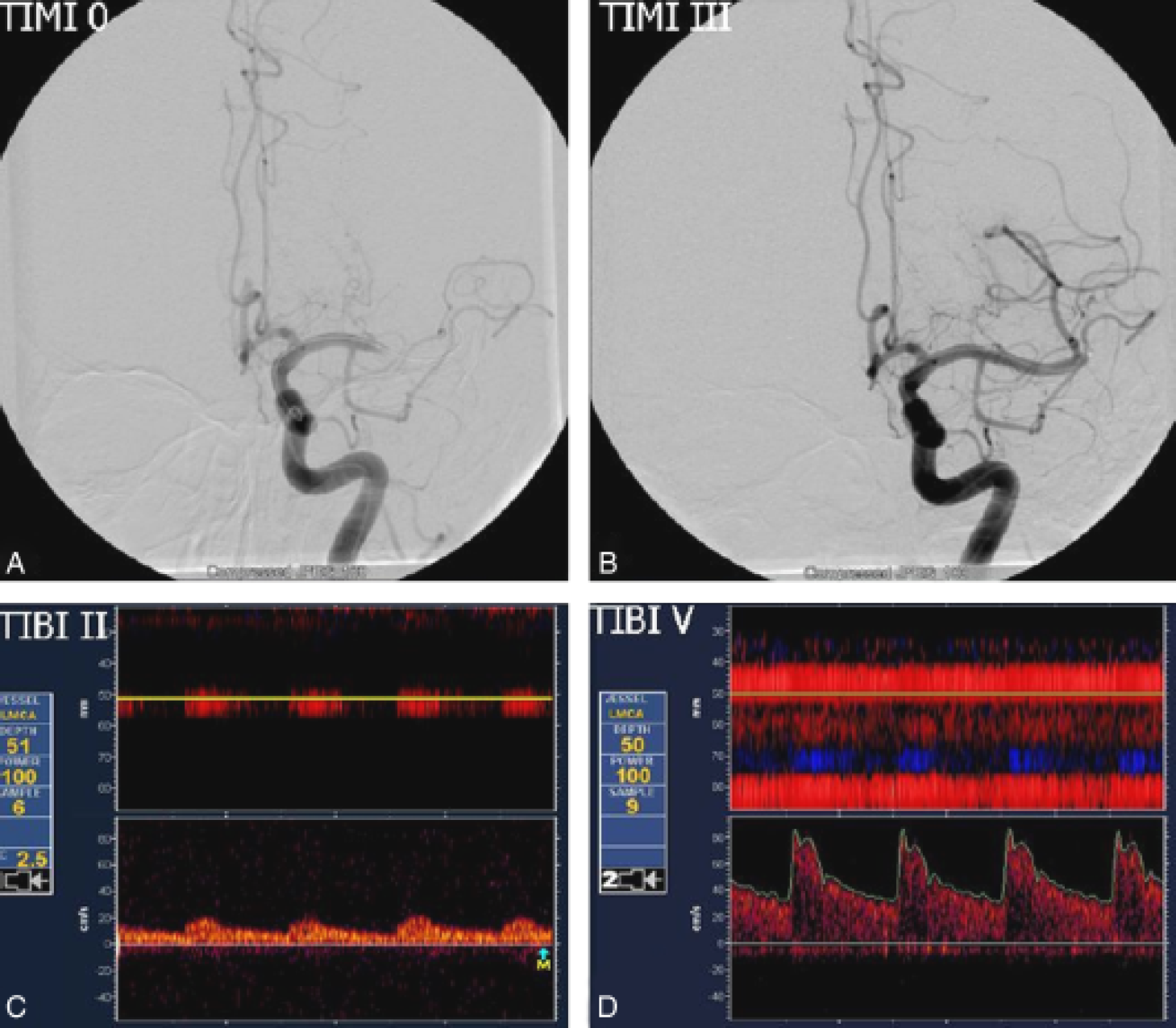
Corresponding TIBI and TIMI grades during complete recanalisation [(c) TIBI II⇒(d) TIBI V and (a) TIMI 0⇒(b) TIMI III]. TIBI, thrombolysis in brain ischaemia; TIMI, thrombolysis in myocardial infarction.
In addition to the presence of a proximal arterial occlusion, patients were matched by the pretreatment stroke severity. To match subjects in the Penumbra trial, we selected control patients from CLOTBUST and TUCSON trials with baseline National Institutes of Health Stroke Scale (NIHSS) scores >7 points.
We compared Penumbra subjects and historic IV tPA controls in terms of age, baseline NIHSS scores, time to treatment, revascularisation, sICH, mortality and favourable functional outcome rates at three-months. The sICH was defined using Penumbra definition as imaging evidence of ICH with clinical worsening (NIHSS>3 points) within 24 h from stroke onset (1). Persisting occlusion, partial and complete revascularisation were defined on the basis of our validated TIBI scores predictive of thrombolysis in myocardial infarction (TIMI) flow grades and compared with TIMI data from Penumbra study. A favourable functional outcome was defined as a modified Rankin Scale (mRS) score of 0–2 at three-months posttreatment.
Statistical comparisons were performed between Penumbra patients and controls using the χ2-test, Fisher's exact test, unpaired t-test and the Mann–Whitney U-test as indicated for dichotomous or continuous variables. The adjusted Wald method [which provides the best coverage for binomial confidence intervals (CI) when samples are < 150] (10) was used for the computation of 95% CI for the rates of recanalisation, mortality, sICH and favourable functional outcome. The
Results
A total of 68 IV tPA-treated patients with MCA occlusions (33 men and 35 women) constituted the historic control group from the CLOTBUST (n=59) and TUCSON (n=9) trials. The baseline TIBI scores on pretreatment TCD assessment were as follows: TIBI 0 (22%), TIBI I (25%), TIBI II (21%) and TIBI III (32%). Patient characteristics are summarised in Table 1.
Baseline stroke severity was similar between patients enrolled in Penumbra (mean NIHSS score 17·6 ± 5·2 points, n=125) and historic controls (16·3 ± 5·3 points, n=68, P=0·101). The Penumbra subjects were younger than historic controls: 68·8 ± 13·4 vs. 63·5 ± 13·5-years, P=0·010. Time-to-treatment initiation was on average 2 h later in Penumbra (4·3 ± 1·5 vs. 2·3 ± 0·6 h, P<0·001).
The rate of any revascularisation after treatment with Penumbra was higher than that following intravenous thrombolysis: 82% [95% CI: 74–87% (54% TIMI II and 27% TIMI III)] vs. 40% [95% CI: 29–52% (25% partial, 15% complete revascularisation)], P<0·001. The rate of sICH tended to be higher with Penumbra: 11·2% (95% CI: 6·7–18·0%) vs. 4·4% (95% CI: 1·0–12·7%), P=0·182 by Fisher's exact test. Mortality at three-months was higher with Penumbra: 32·8% (95% CI: 25·2–41·5%) vs. 14·1% (95% CI: 7·4–24·8%); P=0·006 by Fisher's exact test. The favourable functional outcome (mRS 0–2) rate was higher in historic controls compared with Penumbra patients: 39% (95% CI: 28–51%) vs. 25% (95% CI: 18–33%); P=0·046 by Fisher's exact test.
Given the fact that 96% of patients treated with Penumbra had a baseline TIMI score of 0 (with the remaining 4% having a TIMI score of 1), we repeated all analyses in the subgroup of patients (n=32) treated with IV tPA who had baseline TIBI scores of 0–1 (equivalent to TIMI 0).
The rate of any revascularisation was lower in historic controls with TIBI 0–1: 41% (95% CI: 25–58%) compared with 82% with Penumbra (95% CI: 74–87%, P<0·001). The rate of sICH was 9·4% (95% CI: 0–25%) in historic controls and 11·2% with Penumbra (95% CI: 6·7–18·0%, P=0·999). Mortality at three-months was higher in patients treated with Penumbra 32·8% (95% CI: 25·2–41·5%) compared with historic controls 13% (95% CI: 5–30%; P=0·043). Favourable functional outcome (mRS 0–2) was reached by 37% of historic controls (95% CI: 22–55%) and 25% among Penumbra patients (95% CI: 18–33%, P=0·252).
In addition, Table 2 summarises currently available recanalisation, safety (in terms of sICH) and clinical efficacy (in terms of favourable functional outcome) data from reperfusion randomised clinical trials (1–3, 10–13).
Comparison of revascularisation stategies
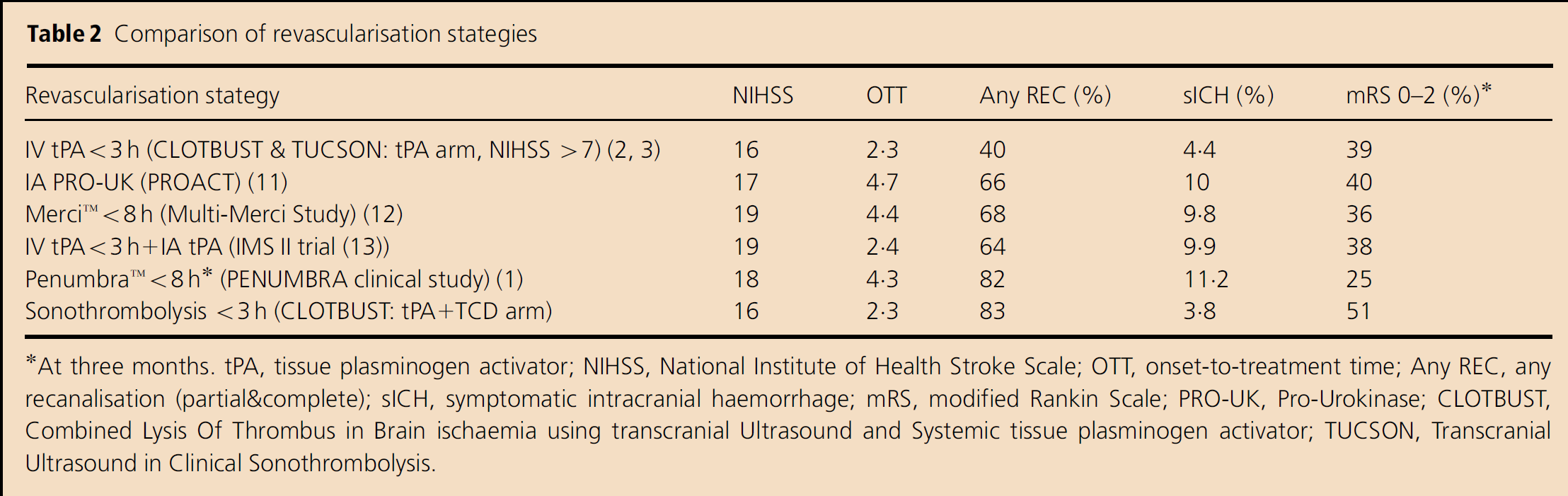
At three months. tPA, tissue plasminogen activator; NIHSS, National Institute of Health Stroke Scale; OTT, onset-to-treatment time; Any REC, any recanalisation (partial&complete); sICH, symptomatic intracranial haemorrhage; mRS, modified Rankin Scale; PRO-UK, Pro-Urokinase; CLOTBUST, Combined Lysis Of Thrombus in Brain ischaemia using transcranial Ultrasound and Systemic tissue plasminogen activator; TUCSON, Transcranial Ultrasound in Clinical Sonothrombolysis.
Discussion
Our retrospective analysis showed that IV tPA has lower overall recanalisation rates compared with Penumbra. However, higher recanalisation rates at a later time window with this IA approach may not necessarily translate into better outcomes. It may be argued that our findings further support a notion that earlier treatment initiation should be the key in delivering stroke therapies.
Our study provides more details for partial and complete recanalisation and recovery rates that can be expected in patients with proximal anterior circulation occlusions treated with IV tPA alone as well as ultrasound-enhanced systemic tPA. These data should be kept in mind when considering a primary IA intervention instead of systemic tPA therapy when a large vessel occlusion is found in a patient presenting within the 3-h window. Systemic tPA is able to induce early recanalisation and lead to favourable outcomes at three-months in almost 40% of patients with MCA occlusions, including tandem ICA+MCA obstructions. If a direct clinical trial is planned to compare primary IA reperfusion vs. systemic tPA, these data should be taken into account when the sample size is being determined. Should sonothrombolysis be considered as a comparator to primary IA, these numbers increase to over 80% (any recanalisation) and 50% (favourable outcomes) (14).
Given unavoidable delays in the initiation of IA procedures (that could decrease the amount of salvageable tissue) and higher rates of haemorrhagic complications, IA technologies need to be further refined and studied in early-phased-controlled studies before primary IA procedures are subjected to efficacy trials against systemic therapy. Interestingly, two intravenous thrombolysis studies, in which the time course of recanalisation was monitored using repeated TCD assessments, have provided preliminary evidence that the rate of symptomatic and asymptomatic ICH following reperfusion therapies may increase with delayed (>6 h) recanalisation (15, 16). Thus, it may be hypothesised that the higher sICH rates caused by delayed recanalisation in Penumbra trial may account for some of the poor three-month functional outcomes. In the future, a combined IV IA approach would likely prove most practical when the advantages of both are considered and no time is lost initiating treatment.
Differences in other baseline characteristics including pretreatment systolic blood pressure, pretreatment blood glucose levels and a history of diabetes mellitus that have been shown to affect outcome in patients treated with systemic thrombolysis (17, 18) may account for the differences in the functional outcomes between the two groups. There were procedural complications/events in up to 12·8% of patients treated with a Penumbra catheter (1). Although most were considered not serious, they may affect the functional outcome. Unlike trials of sonothrombolysis (CLOTBUST/TUCSON) (2, 3), the Penumbra trial failed to report the exact location of MCA occlusion (proximal vs. distal), and only provided information regarding TIMI grades on MCA. However, it should be noted that at 5–8 h, some M1 occlusions might turn spontaneously into M2 without clinical improvement due to deep MCA infarction. In these cases, the impact of M2 thromboaspiration (easier than M1) on stroke outcome may be limited.
Our study has limitations because it is a retrospective analysis with a limited number of historic controls. In addition, a limited number of patients were enrolled in IA trials within the first 3 h of symptom onset and we did not have access to these data. Moreover, we were unable to perform multivariate analyses adjusting for potential confounders (baseline stroke severity, age, onset-to-treatment initiation) because we did not have access to the database of Penumbra trial. However, it should be noted that a recent pooled analysis of all patients enrolled in The Mechanical Embolus Removal in Cerebral Ischaemia (MERCI) and Multi MERCI trials has shown that onset-to-treatment time was not associated with higher recanalisation or functional independence rates, while it did not affect the mortality of patients undergoing endovascular thrombectomy (within 8 h of stroke symptoms’ onset) in the setting of acute proximal intracranial arterial occlusions (19). Consequently, it may be postulated that the differences in the functional outcome and mortality documented in patients treated with primary revascularisation in comparison with historic controls (treated with IV tPA) may not be related to the earlier onset-to-treatment time of historic controls. Given the recent extension of tPA window up to 4·5 h (20, 21), a similar comparison should be made in the future as the average time to treatment in Penumbra was 4·3 h.
In conclusion, despite lower revascularisation rates, patients treated with systemic thrombolysis within the first 3 h from symptom achieved better functional outcomes than individuals with similar baseline stroke severity treated with Penumbra systems. These data indicate that it is unrealistic to expect primary IA revascularisation to be any better than systemic tPA within the 3-h time window. Improvements in the speed of delivery and performance of IA reperfusion are needed.