
Abstract
Background
Intravenous thrombolysis for acute stroke is more efficient the earlier the treatment is initiated. In-hospital delays account for a significant proportion of avoidable time loss before treatment is initiated. Paradoxically, studies have reported longer door-to-needle times the earlier the patients arrive (‘three-hour effect’).
Hypothesis
We hypothesized that a standardized thrombolysis procedure carried out in a specialized neurological emergency room can minimize in-hospital delays and erase the ‘three-hour effect’.
Methods
Onset-to-door and door-to-needle times of 246 consecutive thrombolysis patients were analyzed. A standardized protocol designed to minimize in-hospital delays was tested using a resident-based stroke team within a neurological emergency room. Correlation of onset-to-door and door-to-needle times was measured as well as differences in treatment times for daytime versus night hours and weekend vs. weekday. Outcome, rate of symptomatic intracranial hemorrhage and mortality were compared with the results of SITS-MOST.
Results
Median door-to-needle time was 25 min compared with a mean of 68 min in SITS-MOST. door-to-needle time did not correlate with onset-to-door time (Pearson's r=−0·097; P=0·13) and patients arriving within 90 min from symptom onset showed comparable door-to-needle times with patients arriving within 90–180 min. Neither treatment on weekends nor during night hours led to significant in-hospital treatment delays. Outcome and safety parameters were comparable with those observed in SITS-MOST.
Conclusions
By applying a standardized and diligently monitored thrombolysis protocol, carried out by a specialized stroke team within a neurological emergency room, in-hospital delays can be minimized. This allows improvement of door-to-needle times irrespective of the time to arrival and treatment during off-hours.
Introduction
In acute ischemic stroke, the infarction expands within minutes and hours from a pure functional lesion to a progressively growing infarct core if reperfusion is not established. It has been estimated that every minute nearly two million neurons are lost in this process (1). Therefore, time to reperfusion therapy is a key predictor for the treatment's efficacy. Results of a pooled analysis of trial data suggest a steady decrease of efficacy for intravenous thrombolysis (IVT) from an ‘odds ratio’ to benefit of 2·8 within the first 90 min over 1·55 for 90–180 min to 1·4 for treatment within 4·5 h (2). The latter was recently reproduced by the ECASS-3 results (3). This shows that even within the approved three-hour time window treatment needs to be initiated as early as possible. Time to treatment, on the other hand, consists of two separate parts: first, time from onset to hospital admission (‘onset-to-door’ (OTD)) and second, time from admission to initiation of thrombolysis, the ‘door-to-needle’ (DTN) time. While the first is often dependent on the specific situation of the patient and the circumstances in which the stroke occurs and thus is only partially influenceable with public educational efforts and training of emergency services (4), the second is a direct responsibility of physicians treating patients with acute stroke in the hospital. Often, time is lost within the hospital for avoidable reasons and even the generous benchmark of a door-to-needle time of 60 min given by the recommendations of the National Institute of Neurological Disorders and Stroke (NINDS) is not met (5).
In addition, a ‘three-hour effect’– the phenomenon that patients admitted in ultra-early time windows display longer DTN times than patients admitted just before the three-hour time line – has now been demonstrated in more than 10 000 thrombolysis patients from various cohorts (6–9). With a possible expansion of the label to the 4·5 h time window of ECASS-3, the danger of time loss gets even more pronounced (3).
Hypothesis: we hypothesized that a standardized and constantly monitored thrombolysis procedure within a neurological emergency room (NER) staffed by a specialized stroke team can minimize in-hospital delays and eliminate the ‘three-hour effect’.
Methods
Emergency procedures and thrombolysis protocol
The Department of Neurology is located in a specialized University hospital containing all clinical neuroscience departments (Neurology, Neurosurgery, Interventional Neuroradiology and Psychiatry). The Erlangen Stroke Service was established in 2006. At that time, a specialized ‘stroke and emergency’-team consisting of one attending physician (specialized stroke neurologist) and 10 neurological residents was introduced. The team staffs (i) the NER, which is located separately from the surgical and general medical ERs within our hospital, as well as (ii) a 14 bed stroke unit applying a 24/7 shift system. The NER receives all kinds of neurological emergencies (e.g. seizures, strokes) and has a catchment population of about 500 000 people. Emergency services are instructed to bring potential stroke patients directly to the NER and whenever possible to inform the NER about symptoms, time of onset and stroke circumstances in advance. A standardized thrombolysis protocol is especially designed to avoid treatment delays (see Fig. 1). Upon arrival, the point of care testing for International normalized ratio (INR; CoaguCheck, Roche, Mannheim, Germany) as well as glucose, hemoglobin and an electrolyte panel is performed with the results being available immediately (<1 min). Other basic laboratory parameters (e.g. CBC, complete coagulation panel, liver function tests) are drawn and the results are available during thrombolysis. No additional diagnostic tests are performed unless specific indications arise. Medical history focusing on potential contraindications for treatment as well as a short standardized neurological exam including an NIHSS score evaluation is performed. All physicians of the stroke service are certified for performing the NIHSS score (certificate of the American Heart Association; http://learn.heart.org). The neuroimaging facility with 24/7 availability of one CT and two MRI scanners staffed by a neuroradiologist is directly located next to the NER and – upon admission of a possible thrombolysis patient – is informed to stand-by and guarantee an available CT-scanner. Within the three-hour time window (4·5 h after publication of the ECASS-3 results (3)), patients are treated based on noncontrast CT and thrombolysis is started directly within the CT scanner after exclusion of clinical and neuroradiological contraindications based on the resident's and/or attending decision. Door-to-needle times are diligently documented, closely monitored by the whole team and regularly discussed during rounds.
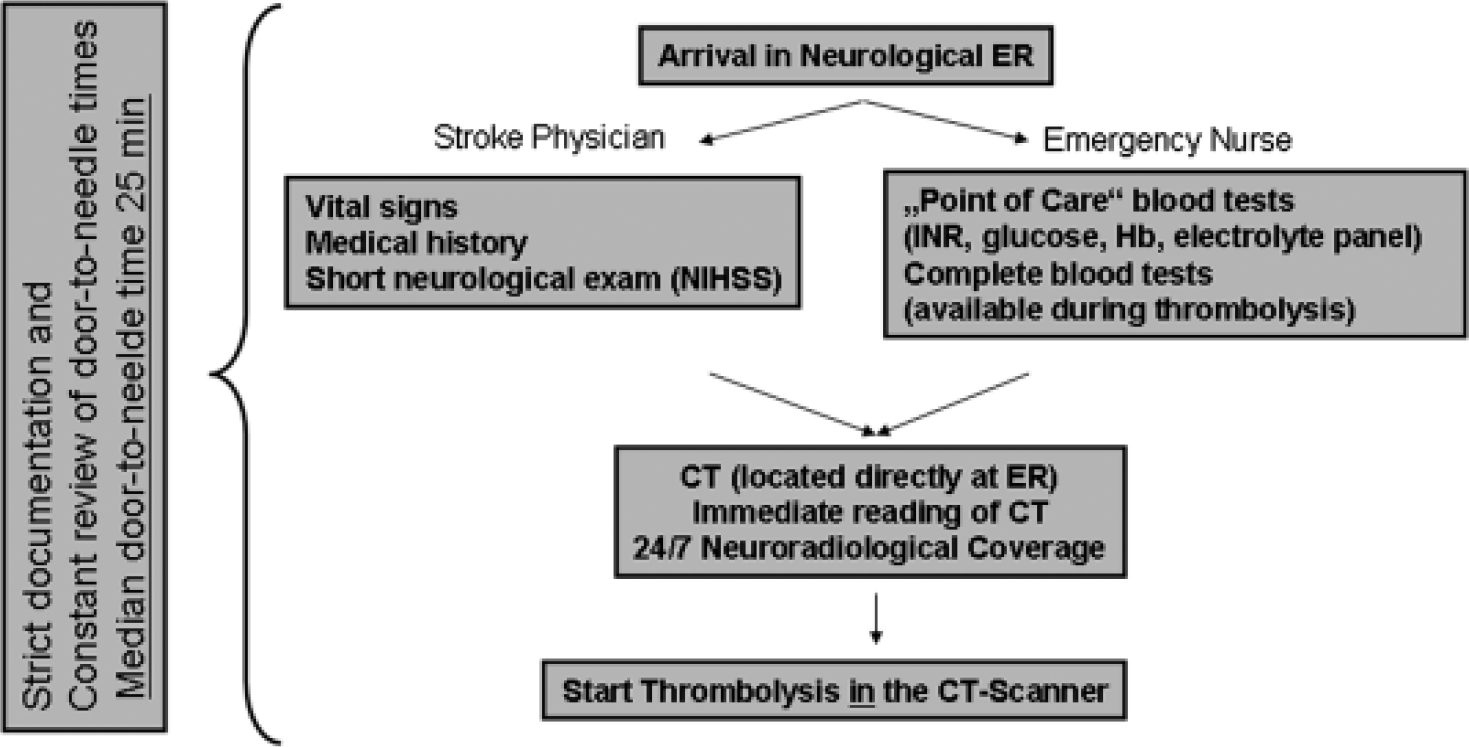
Treatment protocol for thrombolysis patients.
Patient selection and data collection
All stroke patients treated at our center are prospectively entered into the ‘Erlangen Stroke and Thrombolysis’ database, which includes basic demographic parameters as well as clinical and neuroradiological information on the present stroke (10). The OTD and DTN times are included. To allow comparison with other studies on standard IVT, the present analysis consists of all patients receiving IVT based on CT diagnostics within three-hours from symptom onset between 4/2006 and 4/2009. Correlation of DTN and OTD time as well as time of treatment (night- vs. day-time and weekday vs. weekend) was analyzed. Night-time was defined as 22:00–06:00 hours following the regular shift times. Weekend was scored from Saturday 0:00 until Sunday 24:00 hours. Symptomatic intracerebral hemorrhage (sICH) was defined according to the SITS-MOST criteria (11). Outcome was assessed as part of the standard data base evaluation using the modified Rankin Score (mRS) at 90 days and was dichotomized into favorable (mRS 0–2 or return to the prestroke mRS) and unfavorable (mRS>2) outcome according to the SITS-MOST functional endpoint (11).
Statistical analysis
All statistical analyses were performed using the ‘
Results
Baseline characteristics, OTD and DTN times
Two hundred and forty-six patients were included into the present study. Median age was 73·5 years (IQR 63–80) and 60 patients (24%) were over 80 years old. 43% were female and the median NIHSS score on admission was 9 (IQR 5–14). Three patients were diagnosed having a ‘stroke mimic’ during the hospital stay (peripheral facial palsy and general weakness, migraine with aura, partial seizure with subsequent hemiparesis). The median OTD time was 72·5 min (IQR 52–99 min) and 172/246 patients (70%) arrived within 90 min from symptom onset. Median DTN time was 25 min (IQR 18–35 min) (Table 1). Fifty-seven of 246 patients (23%) were treated on a weekend and 37 (15%) during night hours (Table 2).
Demographic parameters, outcome and safety measurements
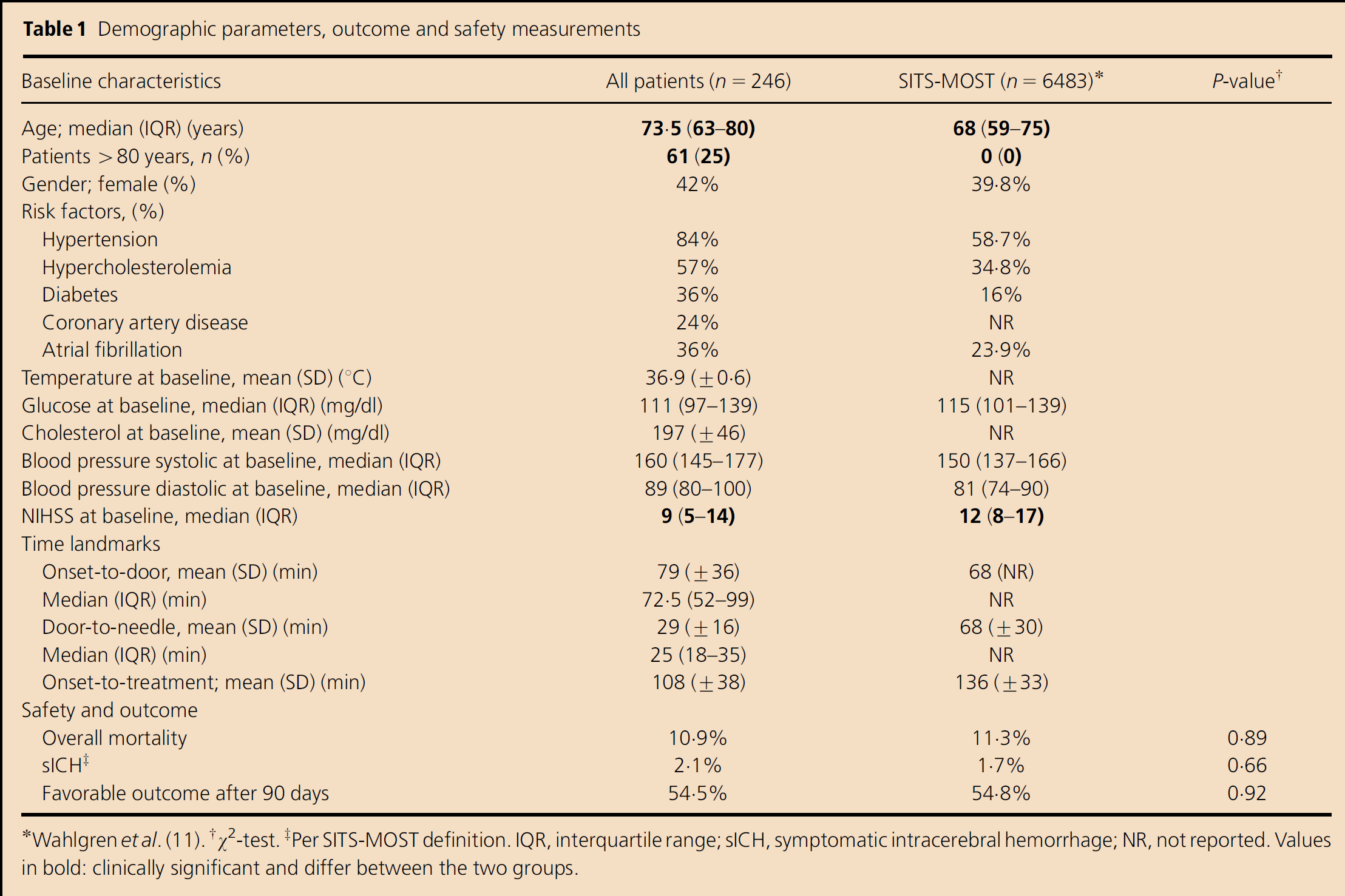
Wahlgren et al. (11).
χ2-test.
Per SITS-MOST definition. IQR, interquartile range; sICH, symptomatic intracerebral hemorrhage; NR, not reported. Values in bold: clinically significant and differ between the two groups.
Door-to-needle times depending on time of treatment (Mann–Whitney U-test)

OTD, onset-to-door time; IQR, interquartile range.
Outcome and safety
Overall mortality within 90 days was 10·9%. Five patients experienced sICH (2·1%; sICH as per SITS-MOST definition) (11) and 54·4% reached a favorable outcome (mRS 0–2). Neither of these outcomes and safety parameters were statistically different compared with the results obtained in the SITS-MOST trial (Table 1) (11).
Correlation of DTN times with OTD and time of treatment
There was no significant correlation between OTD and DTN times (Pearson's correlation coefficient r=−0·097; P=0·13; Fig. 2). In addition, DTN times did not differ between patients presenting to the hospital within or beyond 90 min from symptom onset. The median DTN time for patients <90 min was 25 min compared with 25·5 min for patients in the 90–180 min time window (P=0·33).
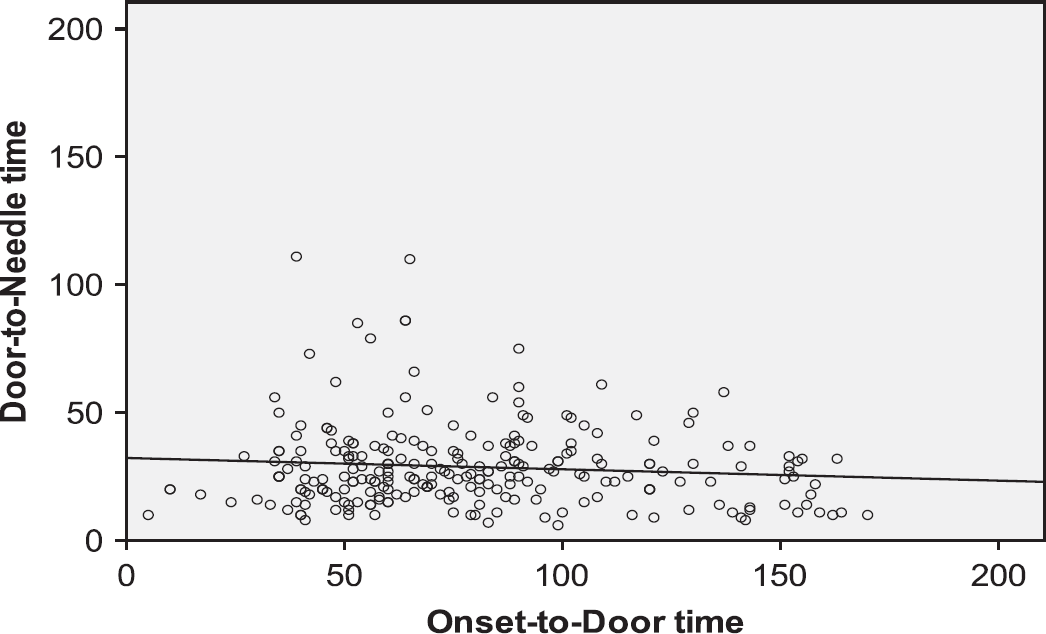
Correlation of onset-to-door and door-to-needle times: there was no significant correlation between onset-to-door and door-to-needle times. (Pearson's correlation coefficient r=−0·097; P=0·13).
Neither treatment on weekends nor during night hours played a significant role for DTN time. On weekends, median DTN time was 28 min compared with 25 min on weekdays (P=0·08) and during night hours 29·5 min again compared with 25 min during daytime (P=0·17; Table 1).
Discussion
The efficacy of IVT is highly dependent on the time window in which treatment is initiated. This was shown for the approved three-hour time window and is especially pronounced in ultra early time windows, although there are little data on treatment within the first hour after symptom onset (2). Time to treatment consists of two time periods: first, the time it takes until the patient is admitted to the hospital (OTD time) and second, the time from admission to initiation of therapy. While public awareness and educational programs have improved OTD times (4), often valuable time is lost because of avoidable organizational problems within the hospital.
Previous studies have shown that re-structuring the emergency service for stroke patients does improve IVT rates as well as time delays until treatment is initiated (7, 12, 13). Three of the central points raised in these studies are implemented into our algorithm. First, neuroradiological facilities are located in the direct neighborhood to the ER with 24/7 emergency availability of CT as well as MRI eliminating transport or waiting times until brain imaging can be performed (12). Second, the treatment decision is made by a specialized mainly resident-based stroke emergency team covering the emergency service at all times (13). Third, we use an expedited algorithm with treatment initiation directly within the CT scanner avoiding delays for additional diagnostics such as stool guaiac (7). In addition, two important aspects are implemented in our protocol: (i) coagulation parameters like the INR are immediately available using the point of care testing, which was shown to reduce treatment delays (14); (ii) diligent documentation of the main time parameters (including DTN time) is carried out by the treating physician and the results are constantly monitored, analyzed and discussed by the stroke service team. The combination of all the abovementioned points resulted in an even shorter DTN time in our cohort compared with the times reported in the above studies (7, 12–14). The median DTN time of 25 min achieved in our cohort is shorter than the one observed in the SITS-MOST registry, which reports a mean DTN time of one-hour and 8-minutes (11) as well as compared with the benchmark of 60 min given by the recommendation of the NINDS (5). Even though patients arrived on average 11 min later than in the SITS-MOST study (mean OTD 79 min in our cohort vs. 68 min in SITS-MOST), they were still treated almost half an hour earlier than in SITS-MOST (onset to treatment times 108 vs. 136 min).
To further test the robustness of the standardized approach, we analyzed whether treatment is delayed during weekend and night hours because both have been discussed to negatively impact stroke care and outcome in previous studies (15, 16). Neither showed a significant impact on DTN times in our study.
It has been reported previously in large cohorts that in IVT for stroke a ‘three-hour effect’ exists (6–9). The earlier a patient is admitted within the three-hour time window, the longer the treating physician takes to initiate thrombolysis. This reverse correlation is mainly attributed to a psychological effect of the treating physician feeling that there is no rush to make the three-hour time window in which IVT is approved (6–8). The phenomenon was first reported for the population in the ‘Standard Treatment with Alteplase to Reverse Stroke’ study (STARS) in which every 30 min delay between stroke onset and ED arrival was associated with a 15 min decrease in the time between arrival and initiation of tPA therapy (regression coefficient, −0·56; P<0·001) (6). The same effect was recently shown in more than 10 000 thrombolysis patients from the ‘Get with the Guidelines-Stroke Database’. The OTD and DTN times were again reversely correlated (r=−0·3) and treatment was significantly delayed in patients arriving within one-hour after symptom onset compared with patients arriving later (9). Being aware of this fact, our study demonstrates that organizational improvements as well as rigid documentation and reviewing of DTN times can eliminate this effect. This is especially important because the time window for IVT is expected to expand to 4·5 h after the results of ECASS-3 (3).
Regarding safety and outcome, there were no statistically significant differences compared with the results of the SITS-MOST study. Of major importance, neither sICH rate nor mortality was increased demonstrating that the faster protocol and the related time gain were not achieved at the expense of higher complication rates. Favorable outcome was observed at a similar rate in both studies. However, a direct comparison of outcome and safety parameters between our study and SITS-MOST must be handled with caution because of different baseline characteristics in the two study populations. On the one hand, the observed median baseline NIHSS score in our population was significantly lower (median NIHSS score 9 vs. 12). Because stroke severity is among the strongest predictors for sICH, this might have lead to lower bleeding complication rates (17). On the other hand, in contrast to SITS-MOST, patients >80 years were included in our analysis and accounted for 25% of our patients. Subsequently, the overall age was significantly higher in our study population (median age 73·5 vs. 68 years). Because age is a comparably strong predictor for safety (17), this may have counterbalanced the effect of a lower stroke severity on bleeding complications. Our study was neither powered to show an improved outcome because of the 30 min earlier treatment compared with SITS-MOST nor to show an improved outcome for early treatment within our cohort. However, as shown in both pooled analyses of the large clinical trials and for pathophysiological considerations, this time gain is likely to translate into improved outcome in larger patient numbers (2).
The main limitation of our study is that our stroke service was newly established in 2006. Thus, no direct internal comparison with previous organizational approaches was possible. In addition, because a completely new protocol was implemented and changes were not made stepwise to an existing protocol, not a single part of the workflow can be identified that helps to expedite the overall procedure. This allows comparison of the final DTN time only with previously reported times in the literature. However, this does not affect the main conclusion of the manuscript that strict organizational structuring helps standardizing DTN, irrespective of the OTD and time of treatment.
Conclusions
Demonstrated in more than 10 000 patients from different cohorts the ‘three-hour effect’ is one of the best-documented procedural flaws in thrombolytic treatment. Especially with the expected expansion of the label of tPA to 4·5 h, it is important to treat patients as early as possible by avoiding in-hospital delays by all means. Thus DTN times and symptomatic hemorrhage rates should be closely monitored, organizational flaws need to be eliminated and treating physicians should never stop aiming for the earliest achievable treatment time.