
Abstract
Aims and Hypothesis
Giant intracranial aneurysms have a poor prognosis mainly due to their high risk of rupture. Because their incidence is low, clinical trial evidence for adequate treatment is lacking. The Giant Intracranial Aneurysm Registry is designed to document current treatment strategies in giant aneurysm care and to monitor the course of the disease over five-years. It aims to evaluate the hypothesis that all three possible branches of therapy (conservative/endovascular/surgical) lead to equal rupture rates.
Design
The Giant Intracranial Aneurysm Registry is an interdisciplinary multicenter observational study. Each center recruits patients diagnosed with a giant intracranial aneurysm both prospectively and retrospectively. Primary outcome will be the aneurysm rupture rate at five-years of follow-up.
Study Outcome
Patient enrollment has begun at 20 neurovascular centers throughout Germany, with 19 further centers applying for local ethics approval to take part in the study. The first nine months are designed as a pilot phase followed by the integration of study centers throughout the EU and the initiation of separate sub-studies.
Discussion
Giant intracranial aneurysms have often been ignored or marginalized due to their low incidence. The Giant Intracranial Aneurysm Registry aims to lead to a better understanding of these complex lesions and to serve as a basis for the development of future clinical studies.
Keywords
Executive Summary
Aim
Giant intracranial aneurysms remain among the most challenging neurovascular lesions. They have a poor prognosis mainly due to their high risk of rupture. As their incidence is low, clinical trial evidence for adequate treatment strategies is lacking. The Giant Intracranial Aneurysm Registry is designed to document the current treatment strategies in giant aneurysm care and to monitor the course of the disease. It is expected to serve as a basis for the development of future clinical studies.
Design
The Giant Intracranial Aneurysm Registry is an interdisciplinary multicenter observational study. Each center recruits patients diagnosed with a giant intracranial aneurysm both prospectively and retrospectively. Past medical history, events leading to the diagnosis, clinical presentation at admission, radiological findings, therapeutic intervention, complications of therapy and outcomes will be documented using standardized criteria at different time points up to five-years after the initial diagnosis. The primary outcome will be the aneurysm rupture rate at five-years of follow-up.
Study outcomes
Patient enrolment has begun at 20 neurovascular centers throughout Germany, with 19 further centers applying for local ethics approval to take part in the study. The first nine-months are designed as a pilot phase, followed by final modifications of data collection, integration of study centers throughout the EU, and the initiation of separate sub-studies. The preliminary results of the pilot phase are expected to be reported in Spring of 2011.
Introduction and rationale
According to diameter, intracranial aneurysms are categorized to be of small (<10 mm), large (<25 mm) or giant sizes (≥25 mm) (1). In previous case series, only about five per cent belong to the giant group (2). These aneurysms usually occur between ages 50 and 70 and can lead to symptoms including headache, cranial nerve palsies, stroke and subarachnoid hemorrhage.
Clinical trial evidence for adequate treatment of intracranial giant aneurysms is insufficient. Cases are usually described anecdotally so that standard therapy guidelines have not yet been established. Most therapists view direct clipping to be the optimal treatment with best outcomes as endovascular coiling usually results in reperfusion or further growth of the aneurysm (3–6). Yet, only one-third of the cases are amenable to direct clipping and therefore proximal occlusion of the vessel carrying the giant aneurysm might be a promising strategy. However, proximal occlusion can only be applied in combination with a feasible revascularization strategy to ensure adequate distal blood flow (7, 8).
Apart from size, the grim prognosis of giant intracranial aneurysms can be explained by unique pathophysiological traits. In contrast to smaller aneurysms that grow from within the lumen, giant intracranial aneurysms are usually partially thrombosed and grow – and therefore rupture – extraluminally (9). This causes an intramural inflammatory response and the proliferation of the vasa vasorum (10). These processes do not play as much of a role in smaller aneurysms. So far, most data on giant intracranial aneurysms were generated from retrospective trials: conservative therapy is associated with a mortality of 75–100% within two- to five-years compared with morbidity and mortality rates for endovascular therapy of 12–42% and 24–29%, and for surgical therapy of 3–8% and 6–12% (4–6, 11–15). Even though surgical therapy seems to be superior, these data should be handled with caution due to their retrospective nature. The only prospective study of giant intracranial aneurysms was carried out during the ISUIA trial (2). Here, 192 giant aneurysms were assigned to a conservative, a surgical or an endovascular therapy group. Prognosis was equally poor in all groups, with five-year rupture rates between 40% and 50 %. The authors comment that one should discuss with the patient that the risk of death or severe disability during conservative therapy is just as large as with endovascular or surgical treatment. This conclusion reflects the current dilemma of giant aneurysm care.
The Giant Intracranial Aneurysm Registry aims to systematically monitor how often giant aneurysms occur, investigate whether they present ruptured or not, document which therapies are being conducted and assess patient outcome of different treatment strategies. The registry is expected to lead to a better understanding of this complex pathology and to inform future intervention studies about the potential endpoints and anticipated efficacy of intervention.
Methods
Constitution of the Giant Intracranial Aneurysm Study Group
The idea of initiating an international multicenter observational registry was developed by investigators from the Department of Neurosurgery at the Charité Berlin and was presented at the national conference of the German Society of Neurosurgery/Vascular Section 2008. The Charité Berlin is the coordinating center of the registry and received the approval of the ethics committee of the Charité Berlin in December 2008. All neurosurgical clinics throughout Germany received an invitation letter to join the registry. So far, 39 have expressed their interest to take part. Each center has to apply for the local ethics committee's approval and will become a member of the ‘Giant Aneurysm Study Group’ once approval is granted.
Definition of the aims, patient eligibility and data flow
In August 2009, a steering committee was appointed and its first meeting took place in Berlin. Here, the aims of the registry were defined as:
to generate a detailed insight into which therapies are being conducted
to document the natural history of patients and follow it over years after diagnosis
to follow imaging data of giant aneurysms over years after diagnosis, whether treated conservatively or not, and
to expand the register both interdisciplinarily (by inviting neuroradiologic and neurologic centers to join) and internationally.
Inclusion criteria are:
the diagnosis of a giant intracranial aneurysm by CT, MRI or regular angiography
patient age of 18-years and older, and
informed consent.
There are no exclusion criteria. If a patient is not able to give informed consent due to his or her clinical situation, the legal representative of the patient (e.g., a family member) will be informed and asked to sign the consent form on the patient's behalf.
Patients will be recruited consecutively to the responsibility of each center. In addition to the prospective part of the study, there is a retrospective part in which patients are included who were admitted after January 2006. Data are gathered at admission, discharge, and one-, three- and five-years after discharge. Patient data will be stored in a pseudonymized fashion. Starting from February 2010, a nine-month pilot phase is being conducted in order to identify and correct possible problems of data acquisition.
Development of a study protocol
Relevant variables were discussed on the basis of the existing literature on giant intracranial aneurysms (2, 7, 16, 17). All variables were chosen so that they can be determined in a routine clinical context even in small centers with minimal technical equipment. It was decided that data collection was to be carried out using a modular structure, consisting of a basic module and additional modules for specific research questions. This set-up proved efficient in earlier registry studies (18, 19).
The steering committee decided on the content of a mandatory basic data collection for all centers. This basic module was designed to keep the amount of variables at a minimum so that data collection can be conducted as safely and quickly as possible by multidisciplinary physicians (Fig. 1). It focuses on the clinical course between initial presentation and discharge but also includes data on patient history, such as risk factors and possible prior aneurysm therapy. A neurological examination of cranial nerve functions, motor capability and speech is conducted initially, at discharge and during three mandatory follow-up examinations. At each examination, the patients' physical condition is recorded using internationally accepted and reliable grading systems. The investigator is asked to not only record a clinical diagnosis, such as epileptic seizure or incidental finding, but also to use imaging data to produce a radiological diagnosis and characterise the aneurysm regarding its location, size, shape and structure. The mode of therapy is documented choosing between conservative, surgical and endovascular options and combinations thereof. Possible complications are recorded as well as the radiologic results of intervention.
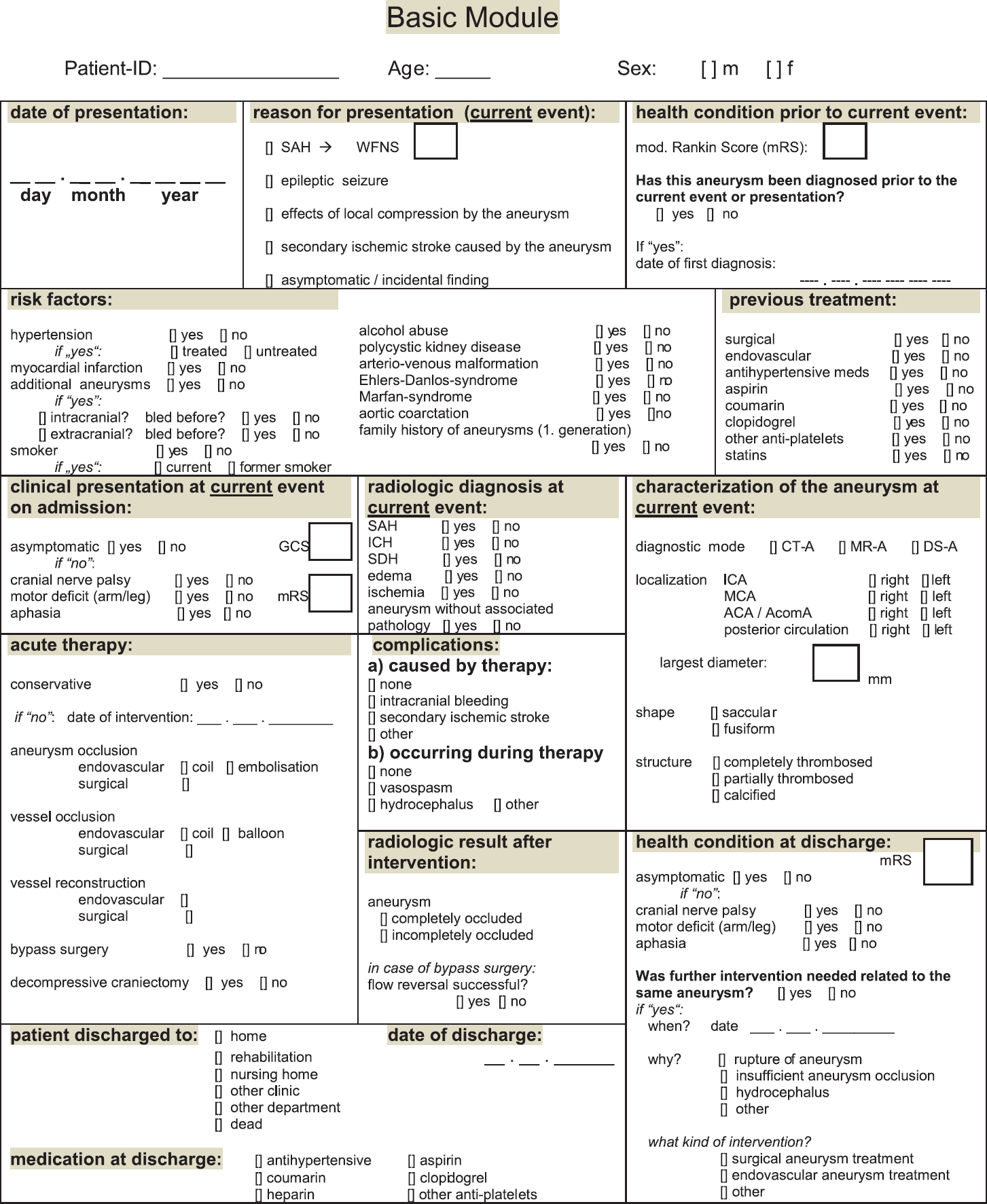
Basic Module. Each center is required to complete the Basic Module data sheet. SAH, subarachnoid hemorrhage; WFNS, World Federation of Neurosurgery – Score; ICH, intracerebral hematoma; SDH, subdural hematoma; CT-A, computed tomography angiogram; MR-A, magnetic resonance angiogram; DS-A, digital subtraction angiogram; ICA, internal carotid artery; MCA, middle cerebral artery; ACA, anterior cerebral artery; AcomA, anterior communicating artery.
Once the pilot phase is completed, each center will be given the option to take part in additional extra modules, which serve as a basis for spin-off projects resulting from the discussion within the study group. This comprises, for example, an imaging module to lead to a better understanding of how giant intracranial aneurysms develop over time. It will monitor changes in the aneurysm configuration and flow dynamics using 3D-imaging data. A cost module will integrate data on treatment expenses, making it possible to compare the costs of each mode of therapy.
An external review of the study protocol was conducted to ensure high methodological quality and wide acceptance of the results. For this purpose, a preliminary working report was forwarded to five independent experts in the field of neurovascular research. The reviewers were asked to comment on the appropriateness of the methods, the practicability of our variables and the coverage of relevant aspects of giant intracranial aneurysm care. The comments of the external reviewers were gathered and discussed within the steering committee. Based on the recommendations of the external reviewers, a final revision of the study protocol took place.
Primary hypothesis, study outcome and statistical analyses
The primary hypothesis of the study is that conservative, endovascular and surgical therapy result in equal aneurysm rupture rates. Therefore, the primary outcome will be the aneurysm rupture rate at five-years of follow-up.
The sample size calculation is based on the estimated five-year cumulative rupture rates for patients with unruptured giant aneurysm given by Wiebers et al. (2). According to their results, we assume a five-year rupture rate of 0·30 irrespective of which specific treatment is applied. Because of a lack of data on special rupture rates regarding patients treated with the three considered methods, sample size calculation was carried out for one proportion based on precision analysis. Consequently, a two-sided 95% confidence interval with a width equal to 0·10 is achieved by a sample size of 320 patients.
For the outcomes death or rupture, the corresponding survival functions with 95% confidence intervals will be estimated using the Kaplan–Meier method. The null hypotheses of equal survival curves for two treatment groups will be tested using the Log-Rank test. With documented dates of rupture events, the sample size of 320, calculated above, is sufficient to detect even moderate effects of possible predictors for rupture by Cox's proportional hazards regression within a secondary analysis. The statistical method of choice for detecting significant predictors for aneurysm rupture after five-years and quantifying their effects is multivariate logistic regression. The link function for this model is the logit function, which means the natural logarithm of the odds for the outcome. Therapy (conservative, surgical or endovascular) will be the main factor of interest in all multivariable analyses.
Patient recruitment
Since January 2010, patient recruitment has begun at 20 centers throughout Germany, and 19 further centers are currently applying for local ethics approval. After the completion of the pilot phase, an expansion into other EU countries is planned.
Summary and conclusions
Size and poor prognosis are only two aspects of the problematic nature of giant intracranial aneurysms. It is also their absolute rareness that has caused them to be either marginalized or ignored in previous studies. Patients with a giant intracranial aneurysm are usually referred to a multitude of health-care professionals of different disciplines and therapy is often guided by individual preference rather than based on evidence.
As there is a need for a better understanding of intracranial giant aneurysms, the Giant Intracranial Aneurysm Registry was initiated as the first multicenter prospective study exclusively dedicated to these complex neurovascular lesions. A comprehensive study protocol was developed focusing on relevant aspects of routine giant aneurysm care. Data acquisition focuses on how intracranial giant aneurysms are currently treated, how they develop over time and how the natural history compares with surgery and endovascular treatment. The main goal of the registry is to produce information on the treatment results and possible end points, which can be applied in the design of future prospective randomized clinical trials.
The registry certainly has its limitations. Because of its observational nature, patients are not randomized into groups and the rationale behind each treatment at each center cannot possibly be adequately captured by a registry. However, as there are no generally agreed-upon therapy guidelines, these limitations are just as much present in current clinical practice as they are in the registry.
Over the past two-years, the Giant Intracranial Aneurysm Study Group took shape as a network of 39 interdisciplinary neurovascular centers throughout Germany, of which 20 are already collecting data at present. The registry has already sparked a lively discussion among representatives of all disciplines involved in giant intracranial aneurysm care and will continue to do so as the study group grows. In September 2010, the pilot phase will be completed and data collection will be expanded to neurovascular centers in other EU countries.
Footnotes
Acknowledgements
We would like to thank Juha Hernesniemi and Riku Kivisaari at the Department of Neurosurgery, Helsinki University Hospital; James Byrne at the Department of Neuroradiology, John Radcliffe Hospital, University of Oxford; and Karl Schaller and Philippe Bijlenga at the Department for Neurosurgery, Geneva University Hospital, for conducting the external review of the study protocol and giving valuable advice in the early stages of the registry. We also thank the Center for Stroke Research Berlin (CSB), Charité Berlin, which is an integrated research and treatment center sponsored by the German Ministry of Education and Research, for financial and methodological support. The CSB has proven expertise in developing, running and analyzing multicenter stroke registers (![]() ).
).
Giant Intracranial Aneurysm Study Group
Bad Berka– J. Behnke-Mursch, K. Mursch, Bonn– A. Grote, J. Schramm, M. Simon, Berlin– M. Endres, A. Gräwe, P. U. Heuschmann, H. Hosch, A. Joedicke, U. Meier, D. Moskopp, J. Dengler, P. Vajkoczy, Dortmund– A. Al-Amin, I. Fiss, R. Schultheiss, Duesseldorf– S. Eicker, D. Haenggi, H. J. Steiger, B. Turowski, Essen– A. Ardeshiri, U. Sure, I. Wanke, Flensburg– W. Boerm, P. Riis, Freiburg– S. Glaesker, V. Van Velthoven, J. Zentner, Geneva– P. Bijlenga, K. Schaller, Goettingen– V. Rohde, D. Wachter, Greifswald– S. Guhl, H. Schroeder, Halle– C. Hohaus, H. J. Meisel, C. Strauss, Hamburg– J. Regelsberger, N. Schmidt, M. Westphal, Hannover– B. Hong, J. K. Krauss, M. Nakamura, Heidelberg– C. Jung, A. Unterberg, Karlsruhe– U. Spetzger, G. Winkler, Leipzig– K. T. Hoffmann, Magdeburg– W. Braunsdorf, Mannheim– M. Barth, K. Schmieder, Munich– J. Lehmberg, T. Liebig, C. Lumenta, B. Meyer, S. Roetzer, M. Wostrack, Murnau– H. Jaksche, M. Strowitzki, Regensburg– A. Brawanski, K. M. Schebesch, Rostock– J. Piek, F. Stockhammer, Stuttgart– N. Hopf, C. Musahl, Tuebingen– B. Krischek, M. Tatagiba, Ulm– R. Koenig, R. Wirtz, Zurich– D. A. Rufenacht, Zwickau– M. Beckert, J. Warnke.