
Abstract
This study reviews available data on stroke epidemiology in Italy. Data were identified through Medline/PubMed, Embase, and from reference lists, related articles, and citation lists of each of the retrieved papers. Nineteen papers were considered, referring to selected stroke-registers performed in seven different geographical areas: Acquaviva-Casamassima county, Aeolian Islands, Aosta district, Belluno district, L'Aquila district, Trasimeno area, and Vibo Valentia district. Registers covered a total population of 2 262 940 people, with a hospitalization rate from 82% to 98%. The mean age at stroke onset was 74·6 ± 1·1 years, 72·3 years in men and 76·6 years in women. Among all strokes:
67·3–82·6% were classified ischemic 9·9–19·6% as primary intracerebral hemorrhage 1·6–4·0% as sub-arachnoid hemorrhage, and 1·2–17·7% as undetermined.
Annual incidence rates standardized to the Italian population ranged from 175/1 00 000 to 360/1 00 000 in men and from 130/1 00 000 to 273/1 00 000 in women. Thirty-day case-fatality rates for all strokes ranged from 18·1% to 33·0% while one-year case-fatality rates ranged from 37·9% to 40·2%. Data from selected Italian registers on stroke incidence and case-fatality indicate the great burden of the disease on our national healthcare system. The continuous implementation of preventive strategies, either population-based or addressed to the single patient at a high risk of stroke, is important to reduce the burden of the disease.
Introduction
Stroke is one of the main public health concerns, representing the third leading cause of death and the main cause of disability (1). Epidemiological studies are fundamental for planning adequate health services for stroke, and to assess the need for and effectiveness of preventive therapeutic strategies and resources (2,3).
This study reviews available data on stroke epidemiology in Italy, which is located on the Italian Peninsula in Southern Europe, Sicily and Sardinia, and covers a total area of 3 01 328·45 km2 with a population, in the last 2001 census, of 56 995 744 individuals (4). The age and gender structure of the resident population are reported in Fig. 1.
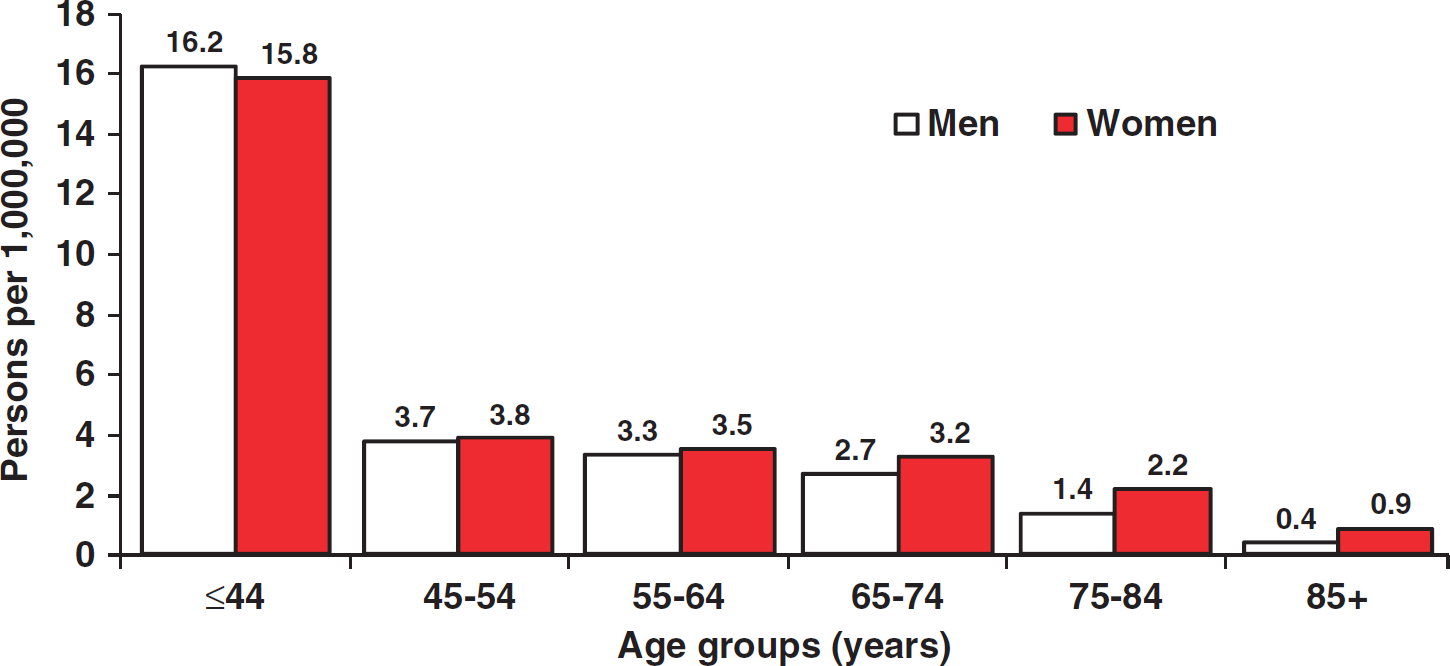
Age and gender structure of the Italian population at the 2001 census.
Methods
Data for this study were obtained through Medline/PubMed and Embase using, in various combinations, the following keywords: population-based, community-based, community, epidemiology, incidence, attack rates, survey, surveillance, mortality, morbidity, fatality, case-fatality, stroke, cerebrovascular disease, isch(a)emic stroke, intracerebral, intraparenchymal, sub-arachnoid, h(a)emorrhage, trends, and Italy. Additional papers were identified from reference lists, related articles, and citation lists of each of the retrieved articles. The search was restricted to the period from January 1970 through to September 2009; papers published in English and in Italian were reviewed. Two authors (S. S. and D. C.) performed the data search, independently graded the articles according to eligibility criteria, and completed data extraction forms. Any disagreement was resolved by a third opinion (A. C.).
Eligibility was agreed upon proposed and updated ideal criteria for a stroke incidence study (2,3,5–7). These criteria required the following issues referring to definition, methods, and data presentation:
compliance with the World Health Organization definition of stroke
at least 80% verification by brain computed tomography (CT) or magnetic resonance imaging (MRI) of the diagnosis of ischemic stroke, intracerebral hemorrhage, and sub-arachnoid hemorrhage
classification of ischemic stroke into sub-types where possible, and
inclusion of first-ever-in-a-lifetime and recurrent strokes (separate and combined).
The standard methods required the presence of:
complete population-based case ascertainment, based on multiple overlapping sources of information: hospitals (including admissions for acute vascular problems and brain imaging studies and/or interventions), outpatient clinics (including regular checking of general practitioners' databases), and death certificates
prospective study design, with hot pursuit of cases
large, well-defined stable resident population
follow-up of patients' vital status for at least one-month, and
reliable method for estimating the denominator (census data not more than five-years old).
The standard data presentation required the presence of:
complete calendar years of data; not more than five-years of data averaged together
data on men and women presented separately
recommended reporting of age-specific estimates within standard mid-decade age bands (e.g., 45–54 years), including the oldest age group (≥85 years) and 95% confidence intervals (CI) around rates.
For this review, because the majority of the Italian studies were performed earlier than the year 2000, the proportion of verification by brain CT or MRI of stroke types was set at 65%. Moreover, we also included studies not reporting the classification of ischemic stroke sub-types. Reviewed data included data collection and study period, population at risk, total strokes, and their distribution according to gender, percentage of neuroimaging and of hospitalization, age at stroke onset, distribution of risk factors, distribution of stroke types, stroke incidence rates and time trends, stroke case-fatality rates, post-stroke disability, and stroke recurrences.
In the case of multiple publications reporting data from the same population over different time periods, the most recent one was used for the analysis of stroke incidence; we referred to the one with the best data completeness. In the analysis of trends, all available studies were considered.
In this review, all strokes classified as ‘undetermined stroke,’‘unknown,’‘stroke of unknown origin,’‘not known,’‘undetermined,’‘ill-defined,’ or ‘stroke of unspecified type’ were reported as ‘undetermined.’
Statistical analysis
The incidence of first-ever-in-a-lifetime stroke was reported per 1 00 000 person-years. Incidence was computed by age, gender, and stroke type where available. For standardization of incidence by age and gender, we used the direct method. The 2001 Italian, 2006 European, and 2005 world populations were used as reference populations, where necessary (4,8,9). We calculated CI by assuming a Poisson distribution of incident strokes over time. A Poisson regression model was fitted to data to calculate the incidence rate ratios (IRR) of stroke for age, gender, geographic area (Northern, Central, and Southern Italy), and study period. Only factors with a P-value<0·10 were included in the final model. To compare stroke incidence rates by type, we resorted to indirect standardization, because the age and gender distribution was not available for all studies. The age-specific incidence rates from L'Aquila were used as a reference to obtain area-specific expected cases. Values were expressed as standardized incidence ratios (SIR). The mean age was calculated by the weighted mean. Case-fatality rates were calculated as the percentage of patients with stroke who died within one-month or one-year after the event. Twenty-eight-day and 30-day case-fatalities were presented combined as 30-day case-fatality rates. Case-fatality rates by stroke types were calculated based on those studies that provided the data. All analyses were performed using
Results
Studies and patients characteristics
Nineteen papers met eligibility criteria and were considered for the present review (10–28). Studies were performed in seven different geographical areas: Acquaviva-Casamassima county, Aeolian Islands, Aosta district, Belluno district, L'Aquila district, Trasimeno area, and Vibo Valentia district (Table 1, Fig. 2). Aosta and Belluno are located in Northern Italy, L'Aquila and the Trasimeno area in Central Italy, and Acquaviva-Casamassina, the Aeolian Islands, and Vibo Valentia in southern Italy. Data were collected from 1986 to 2002 and the duration of the selected studies varied from one- to five-years. The reported studies covered a total population of 2 262 940 people, with 9 08 327 person-years of observation and a hospitalization rate ranging from 82% in the Aeolian Islands study to 98% in the Vibo Valentia study (Table 1) (13,20). The Trasimeno register had 69% of patients evaluated by neuroimaging (21,22). The mean age at stroke onset was 74·6 ± 1·1 years, and was higher in women (76·6 years) than in men (72·3 years). The distribution of risk factors was only available for the Aeolian Islands, Aosta, Belluno, and L'Aquila registers (Table 2). In the Aosta and Belluno registers, the distribution of risk factors referred to patients with ischemic stroke while in the remaining registers it referred to the overall stroke population.
Main characteristics of the population-based registers included in the analysis of stroke incidence and case-fatality
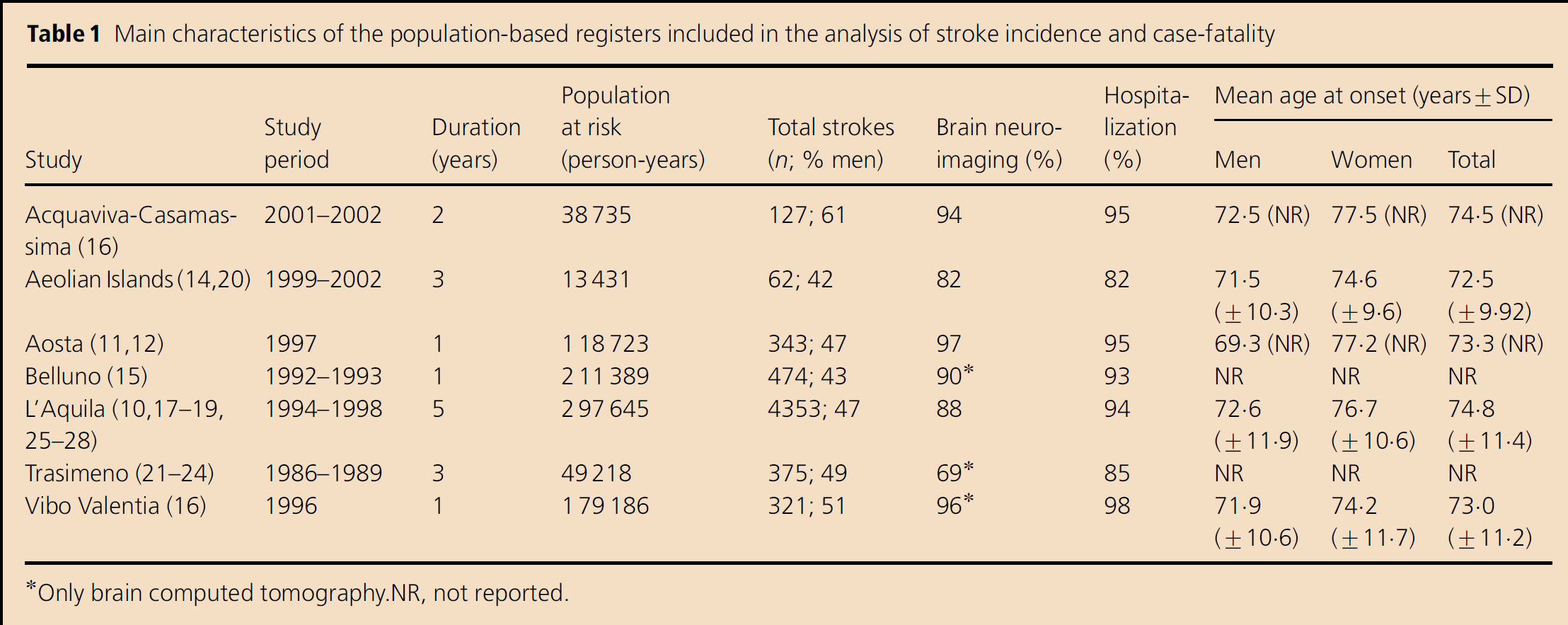
Only brain computed tomography. NR, not reported.
Distribution of risk factors in the selected population-based registers
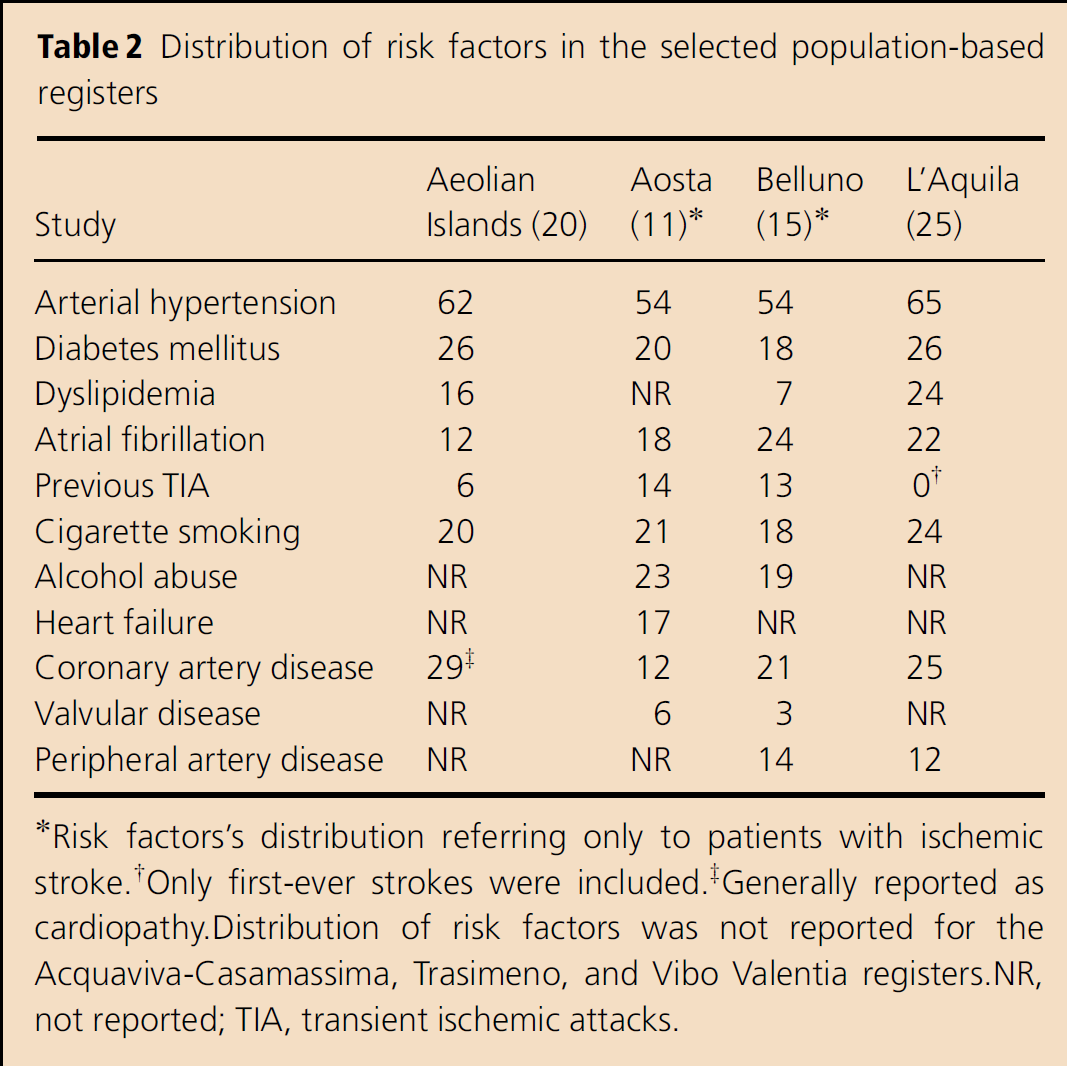
Risk factors's distribution referring only to patients with ischemic stroke.
Only first-ever strokes were included.
Generally reported as cardiopathy. Distribution of risk factors was not reported for the Acquaviva-Casamassima, Trasimeno, and Vibo Valentia registers. NR, not reported; TIA, transient ischaemic attacks.

Geographical distribution of the Italian stroke incidence registers.
Stroke types
Data on stroke type were available from all the seven registers. In five registers (12,13,15,16,20), stroke type classification was reported only for patients who had brain neuroimaging or autopsy studies, while in the L'Aquila and Trasimeno registers (25,27,28,21,22), cases without neuroimaging studies were classified and included according to predefined clinical criteria. The classification of stroke types was performed by brain CT, MRI, or autopsy in a mean proportion of 88% of the cases (from 69% to 97%); in six of the seven registers, the proportion was over 80% (Table 1). The proportions of stroke types are shown in Fig. 3; 67·3–82·6% were classified as ischemic stroke, 9·9–19·6% as primary intracerebral hemorrhage, 1·6–4·0% as sub-arachnoid hemorrhage, and 1·2–17·7% as undetermined.
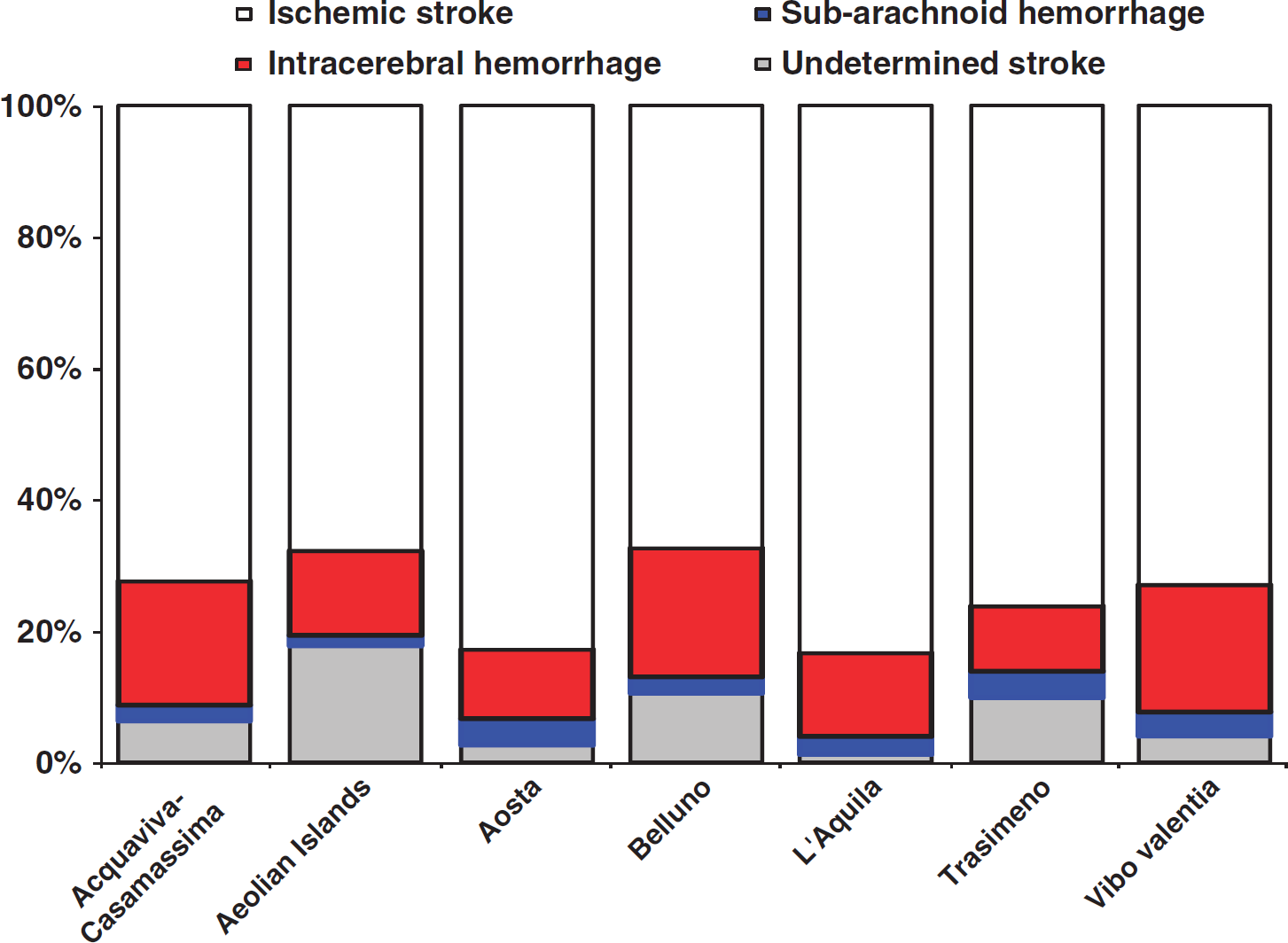
Distribution of stroke types in the selected studies.
Stroke incidence and time trends
The crude and standardized annual stroke incidence rates are reported in Table 3. Crude rates were higher in the L'Aquila register than in the other registers. Rates standardized to the Italian population ranged from 175/1 00 000 in the Aeolian Islands register to 360/1 00 000 in the Aosta register among men, and from 130/1 00 000 in the Acquaviva-Casamassima register to 273/1 00 000 in the Aosta register among women. The crude annual incidence rates per 1 00 000 for all strokes by age groups are reported in Fig. 4. The incidence rates increased linearly with age, peaking in subjects aged ≥85 years in all the registers; the rates were within 17/1 00 000 per year in subjects aged<45 years in four registers (data were not provided by the Acquaviva-Casamassima, Belluno, and Trasimeno registers), from 60 to 141 in subjects aged 45–54 years (data were not provided by the Trasimeno register), from 73 to 280 in subjects aged 55–64 years, from 350 to 816 in subjects aged 65–74 years, from 965 to 1780 in subjects aged 75–84 years, and from 1218 to 3413 in subjects aged ≥85 years. In the Poisson regression model (Table 4), age group, gender, and geographic area were significant predictors of stroke incidence; in detail: living in southern Italy with respect to Northern Italy, and being of female gender, with respect to male gender, were associated with a lower IRR while increasing age group was associated with a higher IRR. Stroke incidence increased slightly by time period but the term was not significant (P=0·10) and was not included in the computation of SIR. The crude annual incidence rates and SIRs according to different stroke types are reported in Table 5.
Crude and standardized annual stroke incidence rates per 1 00 000 population in the included registers
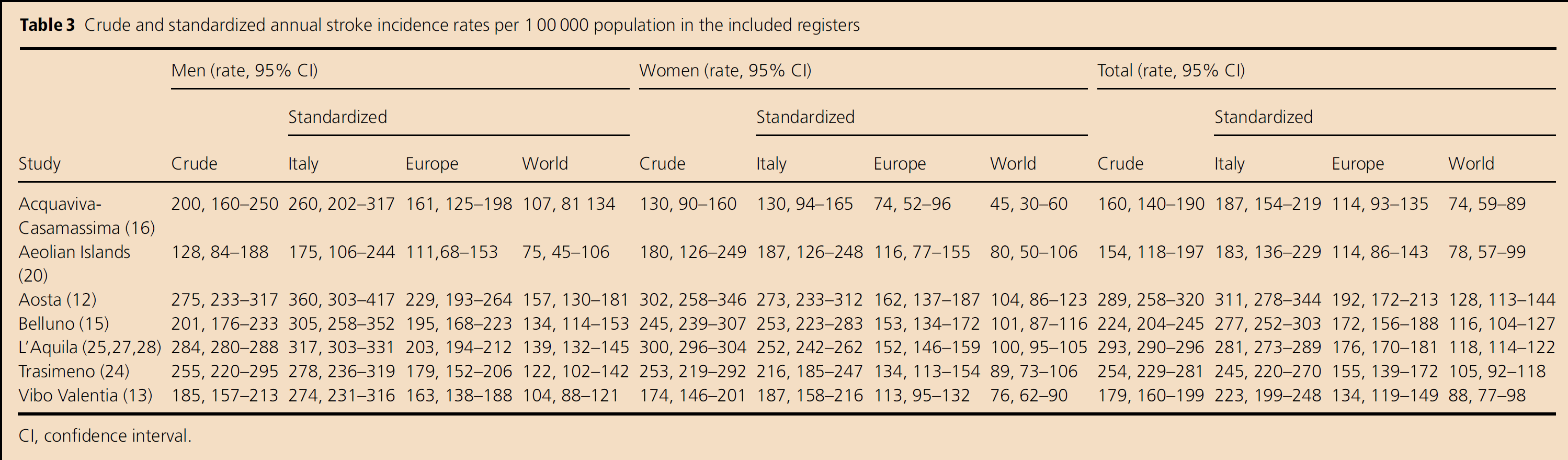
CI, confidence interval.
Poisson's regression analysis of stroke incidence by age class, gender, and geographic area
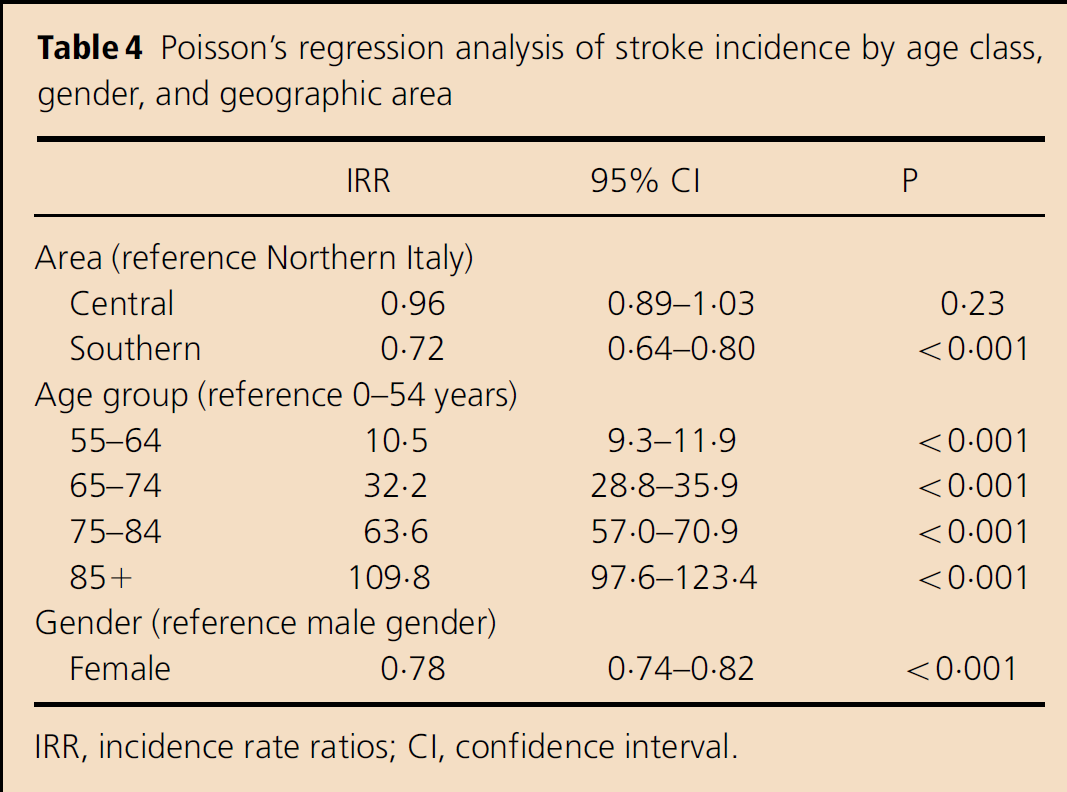
IRR, incidence rate ratios; CI, confidence interval.
Crude annual incidence rates per 100 000 population by stroke types in the included registers and standardized incidence ratio (SIR)
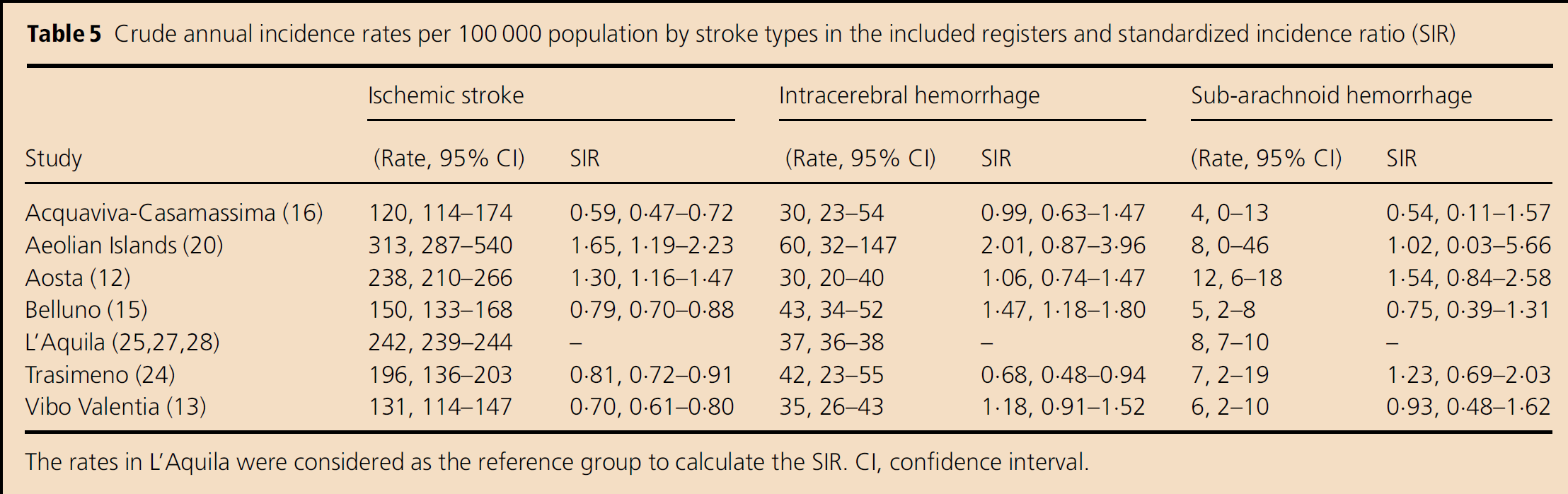
The rates in L'Aquila were considered as the reference group to calculate the SIR.
CI, confidence interval.
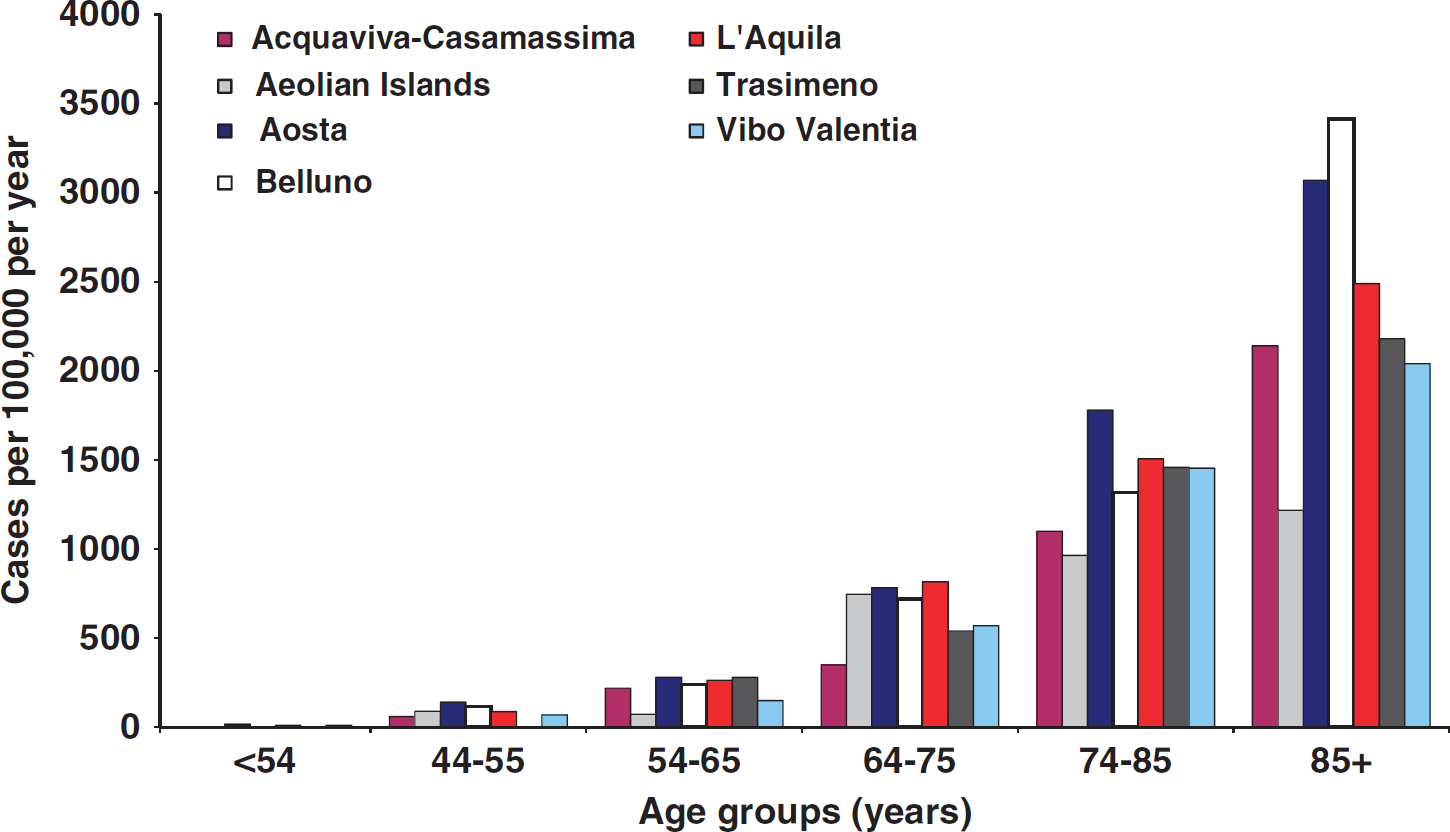
Age specific incidence rates for all strokes. Three registers did not report data for patients aged <45 years (Acquaviva-Casamassima, Belluno, Trasimeno) and one register did not report data for patients aged 45–54 years (Trasimeno).
Three registers were available for the evaluation of the stroke incidence trend (12,24,25). Data from the Aosta register showed an increase of the rate from 223 per 1 00 000 in 1989 to 289 per 1 00 000 in 1997; the increase was observed in all age groups but was statistically significant only in men ≥85 years (P<0·05). However, after standardization for age and gender by the direct method to the Italian population, no significant changes in the incidence rates were found on comparing the two study periods (12). Data from the Trasimeno register showed, after standardization to the Italian population, a decreasing trend not statistically significant from 232 per 1 00 000 in 1986–1989 to 201 per 1 00 000 in 1999, with a lower stroke incidence in the older population (24). In the L'Aquila register, the annual stroke incidence rates increased slightly from 275 per 1 00 000 in 1994 to 283 in 1995, 287 in 1996, 298 in 1997, up to 319 in 1998, with a mean increase of 1·76% per year (slope=1·0176; P=0·1035) at the Poisson regression analysis (25). For ischemic stroke, the mean annual increase was 4·28% and was mainly due to the increased stroke incidence in women (slope=1·0512; P=0·0023) and particularly in women aged ≥85 years, in whom the mean annual increase was 8·52% (slope=1·0852; P=0·0213) (25).
Stroke case-fatality rates
Thirty-day case-fatality rates were reported in all registers, while one-year case fatality rates were reported only in three (13,14,20,25,27,28) out of seven.
Actually, two registers reported case-fatality rates at 28 days (13,16) (Table 6). Case-fatality rates for all strokes ranged from 18·1% in the Acquaviva-Casamassima register to 33·0% in the Belluno register. Case-fatality rates for ischemic stroke ranged from 9·8% in the Trasimeno register to 26·4% in the Belluno register; the rates for intracerebral hemorrhage ranged from 20·8% in the Acquaviva-Casamassima register to 48·1% in the L'Aquila register; the rates for sub-arachnoid hemorrhage ranged from no mortality in the Acquaviva-Casamassima register to 66·7% in the Trasimeno register; and the rates for undetermined stroke ranged from 61·5% in the Vibo Valentia register to 100% in the Aosta and Acquaviva-Casamassima registers. Data were not available for the Aeolian Islands.
Thirty-day and one-year case fatality rates in included registers
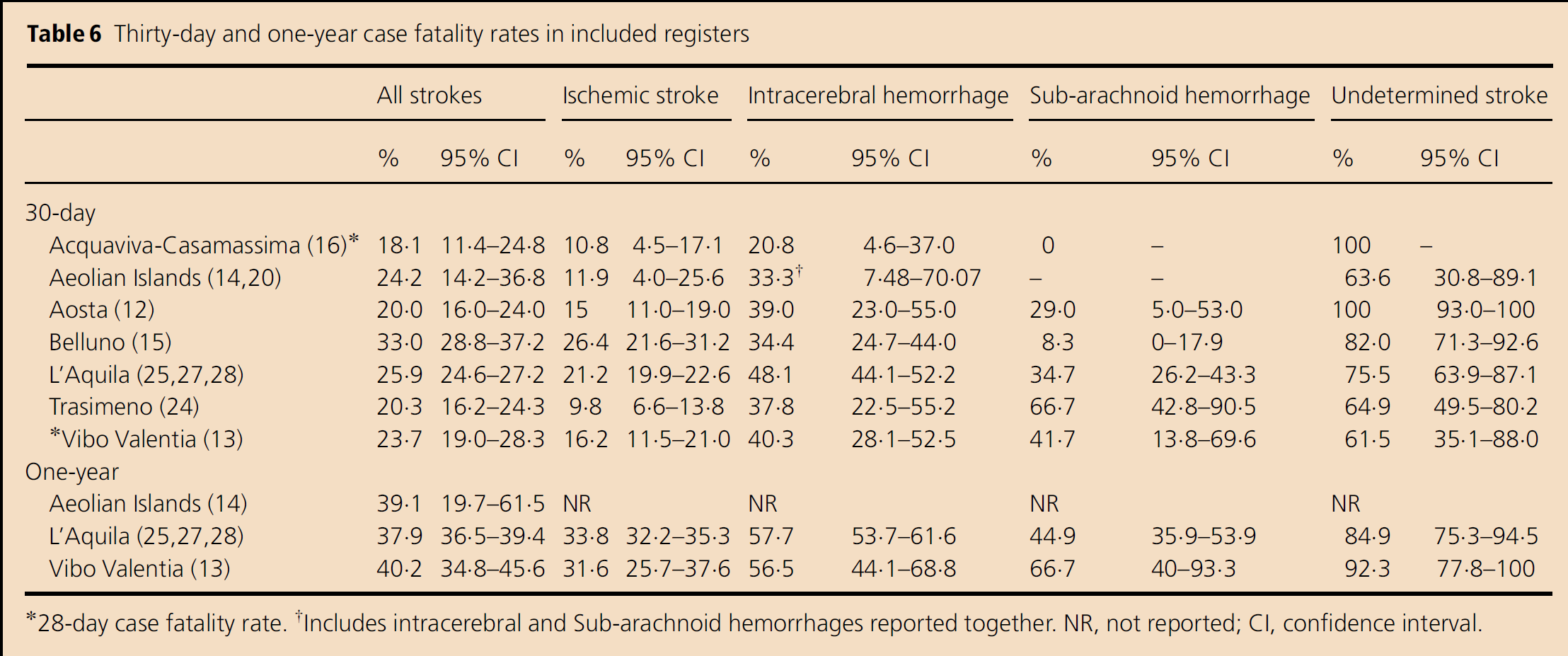
28-day case fatality rate.
Includes intracerebral and Subarachnoid haemorrhages reported together. NR, not reported; CI, confidence interval.
Case-fatality rates at one-year were reported in three areas (Table 6) (13,14,25,27,28). The rates for all strokes ranged from 37·9% in the L'Aquila register to 40·2% in the Vibo Valentia register. Only two registers reported rates for the different stroke types: the rates for ischemic stroke ranged from 31·6% in the Vibo Valentia register to 33·8% in the L'Aquila register; the rates for intracerebral hemorrhage ranged from 56·5% in the Vibo Valentia register to 57·5% in the L'Aquila register; the rates for sub-arachnoid hemorrhage ranged from 44·9% in the L'Aquila register to 66·7% in the Vibo Valentia register; and the rates for undetermined stroke ranged from 84·9% in the L'Aquila register to 92·3% in the Vibo Valentia register.
Data on the long-term mortality were available only for the Aeolian Islands and the L'Aquila register (14,25,27,28). The long-term mortality ranged from 51% in the Aeolian Islands register (95% CI, 35·8–66·3; mean follow-up 33·6 months, range one-day to 6·7 years) to 65% in the L'Aquila register (95% CI, 63·6–66·5; mean follow-up 47·4 months, range from 0 to 11·2 years).
Post-stroke disability
Data referring to post-stroke disability were available for the Aeolian Islands, Aosta, Belluno, Trasimeno, and Vibo Valentia registers. In the Aeolian Islands register, 62% of patients had a modified Rankin scale (mRS) score ≥3 at 30 days, 47% at one-year, and 56% at four-years; moreover, 34% of the patients had a Barthel index (BI)<51 at 30 days, 28% at one-year, and 40% at four-years (14). In the Aosta register, 38% of patients were fully independent at 30 days, 34% were partially dependent, and 29% totally dependent according to the BI score (11). In the Belluno register, 46% of patients were independent in activities of daily living (mRS score≤2) at 30 days (15). In the Trasimeno register, at 30 days, 54% of stroke patients were disabled (mRS score≥3), whereas 25% had recovered completely or almost completely; at six–months, 44% of patients were still disabled (21). In the Vibo Valentia register, 54% of patients were independent in activities of daily living (BI≥85), 12% were mildly dependent (BI 75–84), and 34% were moderately or severely dependent (BI<75) (13).
Stroke recurrence
Data referring to stroke recurrences were available for the Aeolian Islands, Aosta, Belluno, L'Aquila, and Trasimeno registers. In the Aeolian Islands register, 32% of the patients had a recurrent stroke within 30 days (14). In the Aosta and in the Belluno registers, the recurrence rate at 30 days was 2% (11,15). In the L'Aquila register, the five-year recurrence rate was 12% for patients with intracerebral hemorrhage, 11% in patients with ischemic stroke, and 8% in patients with sub-arachnoid hemorrhage (25). In the Trasimeno register, 3% of the patients had a recurrence within six-months (21).
Discussion
Several well-designed registers assessed the epidemiological characteristics of stroke in Italy. They included a total population of 2 262 940 subjects covering Northern, Central, and Southern Italy and can be considered, by their distribution, representative of the global Italian population. The largest available register (n=4353) was performed in the L'Aquila district and included patients over a five-year inclusion period; other studies included less patients within shorter time periods. The design of the studies included fulfilled established criteria of the ideal stroke incidence study, thus contributing to the reliability of the reviewed data.
Global data on stroke incidence were similar to those of other high-income countries (3,29). However, across Italy, several differences were found. Crude rates were higher in the Aosta, Belluno, L'Aquila, and Trasimeno registers with respect to those of Acquaviva-Casamassima, Aeolian Islands, and Vibo Valentia. Lower incidence rates were found in Southern Italy. In those registers, a lower IRR was also found at the Poisson analysis. Differences among incidence rates were only partially mitigated by standardization, indicating that heterogeneity according to age and gender, in the different resident populations, may only partially account for the observed variations. In Italy, there was a quite homogenous Caucasian population with a rather low rate of immigration and emigration in the 1980s and 1990s when the registers were performed and consequently differences cannot be ascribed to heterogeneity in the susceptibility of the disease of interest. Variations in stroke incidence rates may at least in part be attributable to differences in the distribution of risk factors across the populations; however, rigorous comparisons are hindered by differences in the same definition of risk factors. Regions in Southern Italy are also characterized by a low standard of healthcare, which may imply a poor management of risk factors and a low application of primary preventive strategies but also a low hospitalization rate after the acute event that may have led to a bias in case ascertainment. A further explanation may rely on differences in life-style among regions with a higher intake of fruit, vegetables, and fish, which may be protective against stroke, in persons living in Southern Italy (30,31). In fact, the lowest annual incidence rates were found in the Aeolian Islands and can probably be attributed to the high fish intake of the islanders. Information on several other parameters including the distribution of stroke etiology, differences in social and economic structure of the considered study populations, and differences in healthcare organization and stroke care management would be relevant to better understand the results but unfortunately these data were not adequately reported in the considered registers to allow any comparison. In all geographical areas, the incidence of stroke increased with age and was higher in men than in women. When considering the annual incidence rates for the different stroke types, ischemic stroke had a higher incidence rate in the Aeolian Islands, Aosta, and L'Aquila registers with respect to other registers, intracerebral hemorrhage had the highest incidence rate in Belluno and the lowest in the Trasimeno register, while rates of sub-arachnoid hemorrhage were similar across the different registers. The different incidence rates observed might have depended on the number of included patients as on the proportions of diagnoses that were confirmed by brain neuroimaging studies and by the time interval from stroke onset and brain neuroimaging studies in the corresponding registers. As reported in Fig. 3, the proportion of undetermined strokes varied across the studies depending on several factors such as differences in the proportion of included patients who died before reaching the hospital, those who had brain neuroimaging, or those who, in the absence of neuroimaging, were classified according to predefined clinical features in some studies but not in others.
Data on the stroke incidence trend were reported in only three registers (12,24,25). No significant variations were found, except in women aged ≥85 years with ischemic stroke in the L'Aquila register. This result was at variance with more recent data (32). Overall, the crude number of strokes increased, due to increased life-expectancy (33). Because of improvements in primary and secondary stroke prevention, we cannot exclude a possible unrecognized recent decrease in stroke incidence.
Thirty-day and one-year case-fatality rates were comparable with those found in other Western countries (2,29). Case-fatality rates at 30 days were lower in the registers performed in Acquaviva-Casamassima, Aosta, and Trasimeno and higher in the register performed in Belluno. As hypothesized, the results from the Trasimeno register could be explained by the inclusion of very mild cases treated just for a few days, while the results from the Acquaviva-Casamassima and Aosta registers could be explained by a better healthy state of the resident populations or to improved standard of stroke care (34,35). The same considerations could also explain the differences in the 30-day case-fatality rate for ischemic stroke. Intracerebral hemorrhage is characterized by higher case-fatality rates. The highest case-fatality rate for intracerebral hemorrhage was reported in the L'Aquila register as a predictable consequence of a higher mean age of the patients and inclusion of patients who died early, before performing neuroimaging studies (27,36–38), while the lowest value, but with a wide CI, was reported in the Acquaviva-Casamassima register. Differences in the availability of neurosurgical or endovascular treatments in different study periods could explain the data reported on the case-fatality rate of sub-arachnoid hemorrhage. Differences in the case-fatality of sub-arachnoid hemorrhage could not be appreciated in the present review due to the low number of cases included and the consequent overlapping of CI. Available data on long-term mortality in the L'Aquila and the Aeolian Islands registers showed a 14% difference between the two studies, mainly due to the different mean ages at stroke onset of the included patients and the different mean durations of the follow-up, which was shorter in the Aeolian Islands register. Data on post-stroke disability cannot be compared across registers due to differences in the methods of assessment and in time from stroke onset to evaluation while data on stroke recurrence were higher in the Aeolian Islands with respect to the other registers.
This paper identified and reviewed all comparables population-based stroke incidence studies that were performed in Italy. At variance with well-known criteria for the ideal stroke incidence study, the proportion of diagnoses verified by brain CT or MRI had to be set at 65% instead of 80% because one register, performed between 1986 and 1989, included patients with a lower proportion of brain neuroimaging studies. Although the available population-based studies were performed in different years, largely as much as a decade or two ago, due to accurate methodology and stability of the resident population, reviewed data represent a proper estimate of stroke epidemiology in Italy. The reviewed studies did not report proportions of patients of different race-ethnicities. As we already reported, at the time in which the different studies were performed, in those areas and in Italy as a whole, the rate of immigration was low. However, due to the increase of immigration in this last decade and particularly in some areas of the country, race-ethnicity should be included in future studies on stroke epidemiology in Italy.
Conclusions
Data from selected Italian registers on stroke incidence and mortality indicate the great burden of the disease on the national healthcare system. The correlation between stroke incidence and age plays an important role in our country, where the proportion of elderly people is growing, as shown by census data referring to the last three decades (4). However, the continuous implementation of preventive strategies, either population-based or patient-oriented, will contribute to reduce the burden of the disease. Stroke prevention programs, such as control of blood pressure and smoking cessation, implementation and promotion of adherence to guidelines, and increased availability of stroke units and of thrombolytic treatment throughout the nation, will contribute to reduce stroke-related mortality and morbidity.