
Abstract
The primary aim of these guidelines is to assist individual clinicians, hospital departments, and hospital administrators to produce local protocols for the:
assessment, investigation and immediate management of individuals with a transient ischemic attack or acute stroke (other than sub-arachnoid hemorrhage), and secondary prevention and risk factor management following a transient ischemic attack or acute stroke.
The secondary aim of these guidelines is to suggest methods for implementation and clinical audit. The workgroup preparing these guidelines was formed by the Ministry of Health, Singapore. It comprised healthcare workers from relevant specialties, family medicine, nursing, occupational therapy, and a lay patient advocate. The Scottish Intercollegiate Guidelines Network's Clinical Practice Guidelines on the Management of Patients with Stroke were reviewed, updated, and modified to meet local needs. The final guidelines are made up of evidence-based recommendations covering the following areas – assessment, investigation, immediate management, secondary prevention, rehabilitation, and implications for service delivery. The guidelines were sent to professional organizations for comments and endorsements. The final version was circulated to all medical practitioners in Singapore. It is hoped that the guidelines will improve the care of patients with stroke and transient ischemic attack. Clinical quality improvement measures are proposed.
Introduction
Stroke is a major cause of death, disability, and hospitalization in Singapore (1). Cerebral infarction accounts for 74%, primary intracerebral hemorrhage 24%, and sub-arachnoid hemorrhage 2% (2). Heavily subsided, accessible healthcare is provided by a network of public sector hospitals and polyclinics scattered throughout the island. Private practitioners provide 80% of primary healthcare services, while government polyclinics provide the remaining 20%. However, public hospitals provide 80% of the more expensive hospital-care with the remaining 20% being provided by private hospital care (3).
Scope of the guidelines
These guidelines address the assessment, investigations, immediate management, and secondary prevention of stroke and transient ischemic attack (TIA). This paper is a summary of the evidence behind the recommendations made in the guidelines; the recommendations are reproduced in full: Tables 1–6.
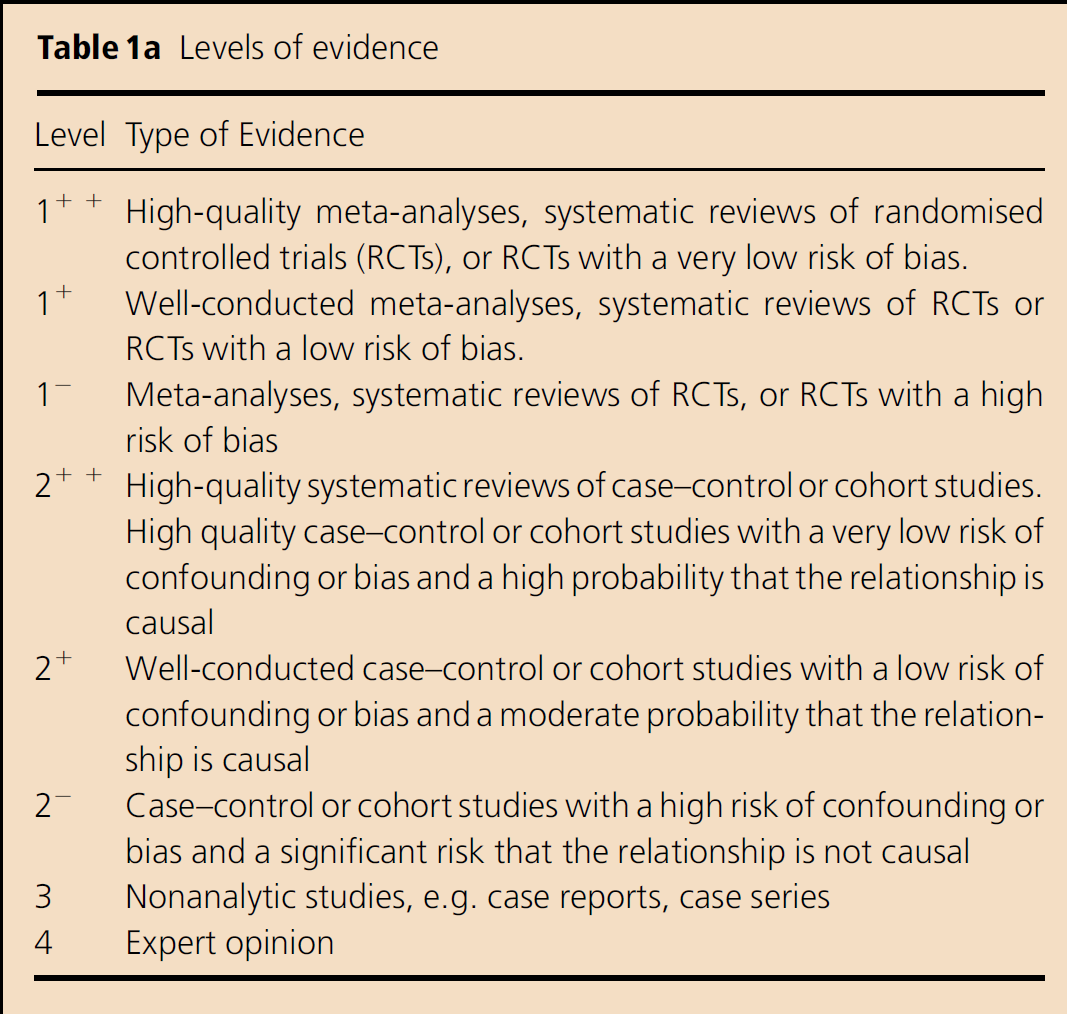
Levels of evidence
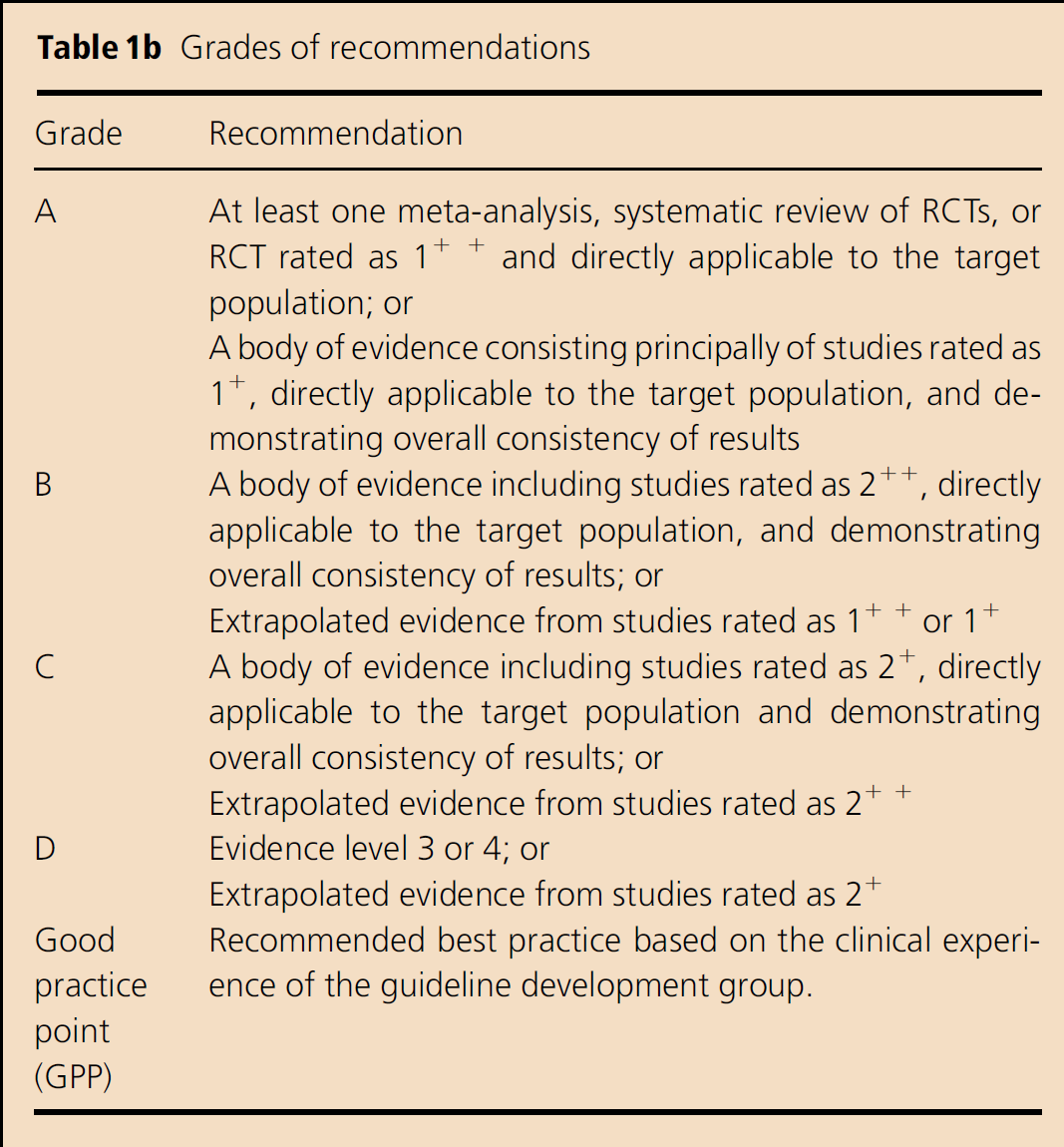
Grades of recommendations
Assessment and investigation of acute stroke and transient ischemic attack
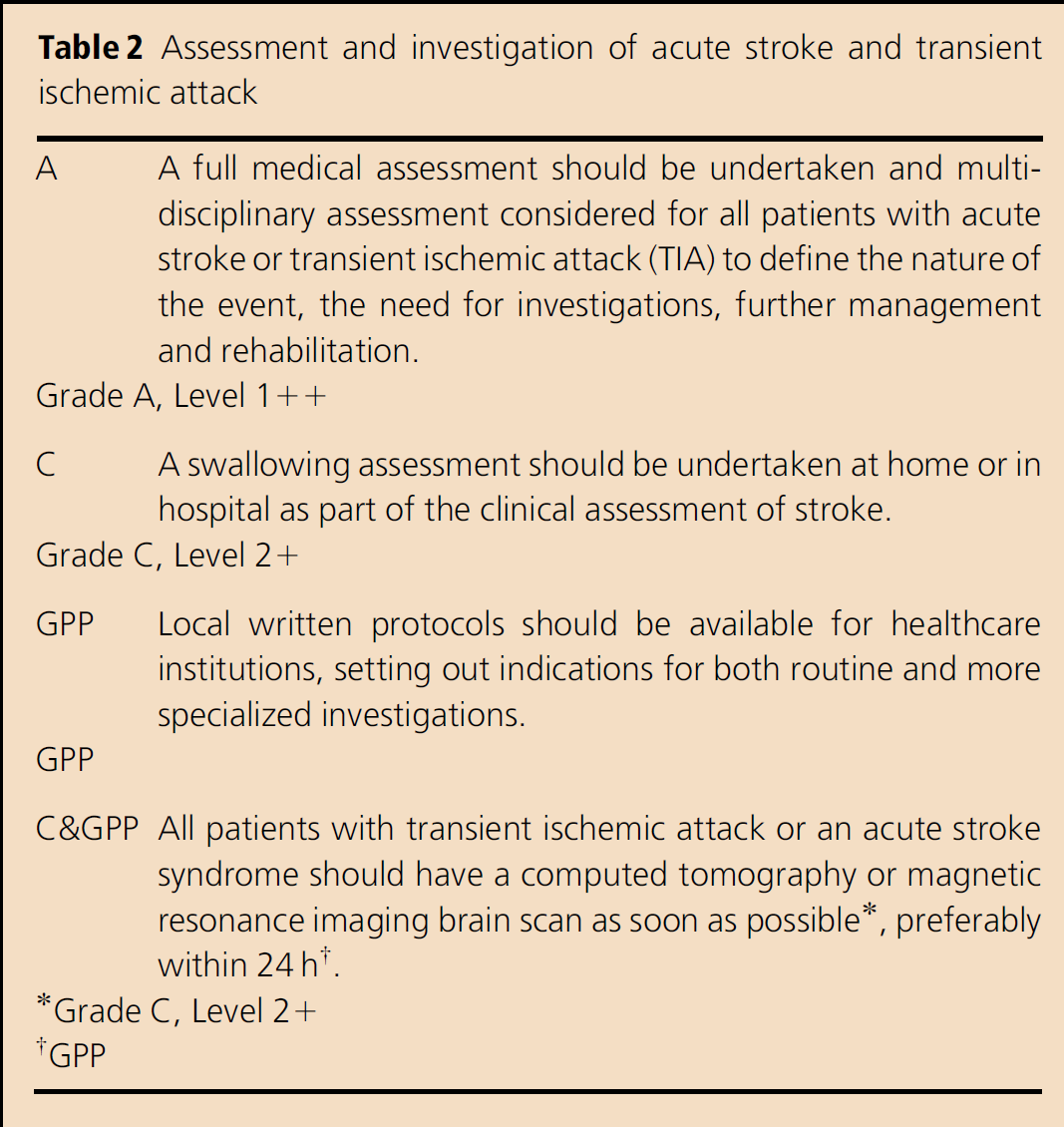
Grade C, Level 2+
GPP
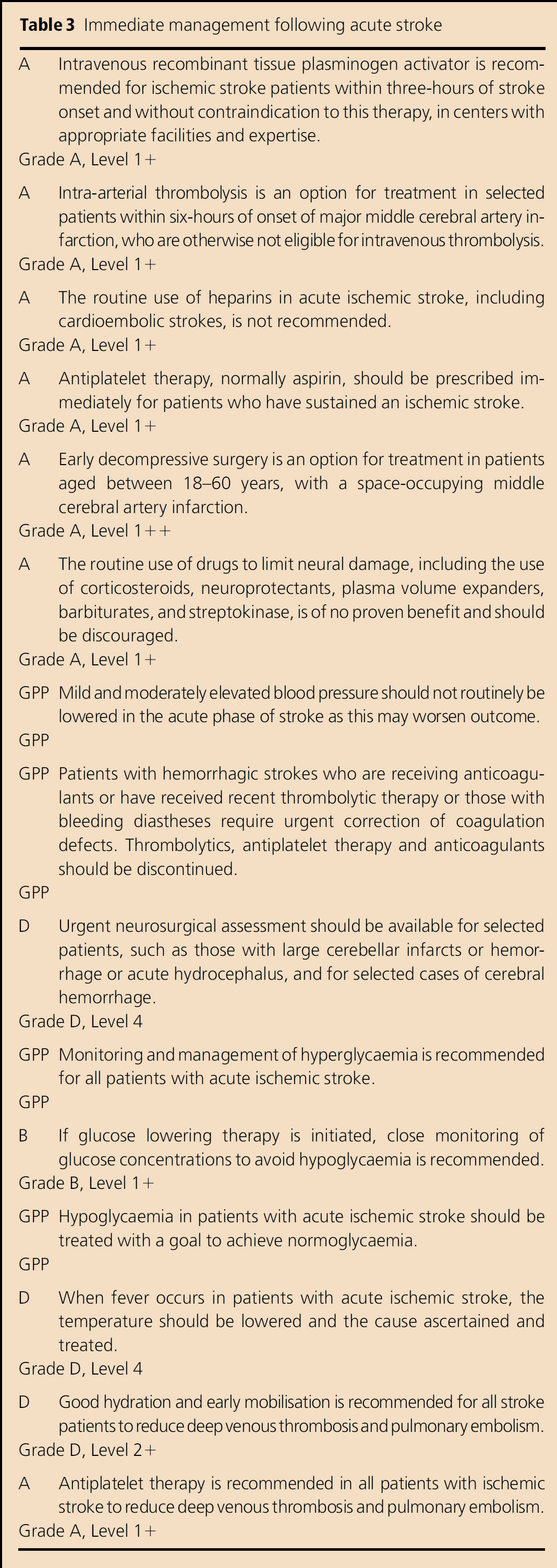
Immediate management following acute stroke
Secondary prevention following acute ischemic stroke and transient ischemic attack
Rehabilitation
Implications for service delivery
The complete version of the guidelines is available at http://www.moh.gov.sg/mohcorp/publications.aspx?id=22920
Objectives of the guidelines
The primary aim of these guidelines is to assist individual clinicians, hospital departments, and hospital administrators in producing local protocols for:
assessment, investigation, and immediate management of individuals with a TIA or acute stroke (other than sub-arachnoid hemorrhage), and
secondary prevention and risk factor management following a TIA or acute stroke
The secondary aim of these guidelines is to suggest methods for implementation and clinical audit.
Development process of the guidelines
The workgroup, formed by the Ministry of Health, Singapore, comprised specialists from neurology, neurosurgery, neuroradiology, rehabilitation, family medicine, nursing, occupational therapy, and a lay patient advocate. The Scottish Intercollegiate Guidelines Network's Clinical Practice Guidelines on the Management of Patients with Stroke (4) were reviewed, updated and modified to meet local needs. The system of levels of evidence and grades of recommendation used to grade recommendations are shown in Table 1. The draft guidelines were then sent to various professional organizations for comments and endorsements. The final version was sent to all medical practitioners in Singapore, and also made available on the website of the Ministry of Health. The guidelines will form the basis of the ministry's audit of clinical practice by healthcare organizations.
Summary of evidence
Assessment and investigation of acute stroke and TIA is given in Table 2.
Multidisciplinary assessment, as part of the organized stroke unit care, involving nursing and other medical professionals, should begin as soon as possible in the management of a patient with a stroke (5). Assessment of swallowing should be undertaken before permitting oral intake. Nurses may be trained to perform an initial dysphagia screen. Patients with swallowing defects should be referred to a speech therapist.
Neuroimaging by computed tomography (CT) or magnetic resonance imaging (MRI) is essential for accurate diagnosis (6). Both allow a definitive diagnosis, differentiation of ischemic from hemorrhagic stroke, exclusion of mimics, and assessment of arterial and venous flow and brain perfusion (7, 8).
Other imaging modalities include carotid ultrasound, transcranial Doppler ultrasound and digital subtraction angiography.
Immediate management following acute stroke is shown in Table 3.
Cerebral infarct
Intravenous recombinant tissue plasminogen activator (rtPA) significantly improves functional outcome at three-months and one-year in patients treated within three-hours of ischemic stroke onset (9, 10). Although it carries the risk of symptomatic brain hemorrhage with high mortality, it is safe and effective in routine clinical practice (11).
Intravenous rtPA therapy commenced between 3–4·5 h after stroke onset is also associated with significantly increased favorable outcomes (12), but the benefit is less than rtPA initiated within three-hours. Thus intravenous rtPA should be initiated as soon as possible in suitable patients within three-hours of stroke onset, with possible extension of the treatment time window to 4·5 h.
Intra-arterial prourokinase in patients with stroke in the middle cerebral artery (MCA) territory of less than six-hours duration gives better clinical outcomes vs. placebo despite a slightly higher rate of hemorrhage (13).
Thrombolysis requires the patient to be at an experienced stroke center with immediate access to cerebral angiography and qualified interventionalists.
Mechanical devices (MERCI, Concentric Medical Inc, Mountain View, California, USA) may be effective in clot retrieval, while ultrasound-enhanced thrombolysis may improve recanalization, but improved clinical outcome has not yet been demonstrated (14–16).
Heparins (unfractionated heparin (UFH), low-molecular-weight heparin (LMWH), or heparinoids) do not reduce mortality. Any reduction in recurrent stroke is offset by the increase in symptomatic intracranial hemorrhage (17).
Commencement of aspirin within 48 h of ischemic stroke onset reduces early recurrence (18, 19).
Decompressive surgery improves functional outcome and reduces mortality when undertaken within 48 h of stroke onset in patients aged between 18 and 60 years, with a space-occupying MCA-territory infarction (20).
Corticosteroids, hemodilution, and neuroprotectants confer no benefit (20–24).
Blood pressure
A reduction of blood pressure occurring as a side effect of treatment is associated with a worsening of outcome (25).
The current recommendation is to carefully treat hypertension if SBP>220 mmHg or DBP>120 mmHg. Exceptions include patients who have been thrombolysed, have hypertensive encephalopathy, aortic dissection, acute renal failure, acute myocardial infarction, or acute pulmonary edema (26). Conversely, persistent hypotension should be corrected speedily (26).
Neurosurgical intervention
Early surgical evacuation of spontaneous, supratentorial, intraparenchymal hematomas is not better than conservative treatment (27). Surgical evacuation of intraparenchymal hematomas could be considered if the hematoma is thought to be causing clinical deterioration.
Ventricular shunting and decompression surgery should be considered in patients with cerebellar stroke and acute hydrocephalus due to compression of the aqueduct of Sylvius (28).
Medical management
Hyperglycemia
There is no benefit of maintaining normoglycemia by glucose–potassium–insulin infusion (29); if glucose lowering therapy is initiated during acute stroke, close monitoring of glucose concentrations to avoid hypoglycemia is needed.
Hypoglycemia
Hypoglycemia should be treated. The goal is to achieve normoglycaemia. Marked elevation of blood glucose levels should be avoided.
Fever
Paracetamol is modestly effective in lowering temperature in acute stroke (30).
Venous thromboembolism
Thigh-length, graduated compression stockings result in a non-significant, absolute reduction in deep vein thrombiosis (DVT) but lead to significantly more skin breaks, ulcers, blisters, and skin necrosis (31). Mechanical compression devices are effective in aneurysm patients (32).
In acute ischemic stroke, aspirin reduces DVT and pulmonary embolism (PE) (33, 34).
Heparin reduces the risk of asymptomatic DVT (35, 36). However, the small non-significant reduction in PE is more than offset by an increase in intracranial and extracranial hemorrhage (34). LMWH may be safer than sub-cutaneous UFH. Other measures that may prevent DVT include early mobilization, and good hydration (36).
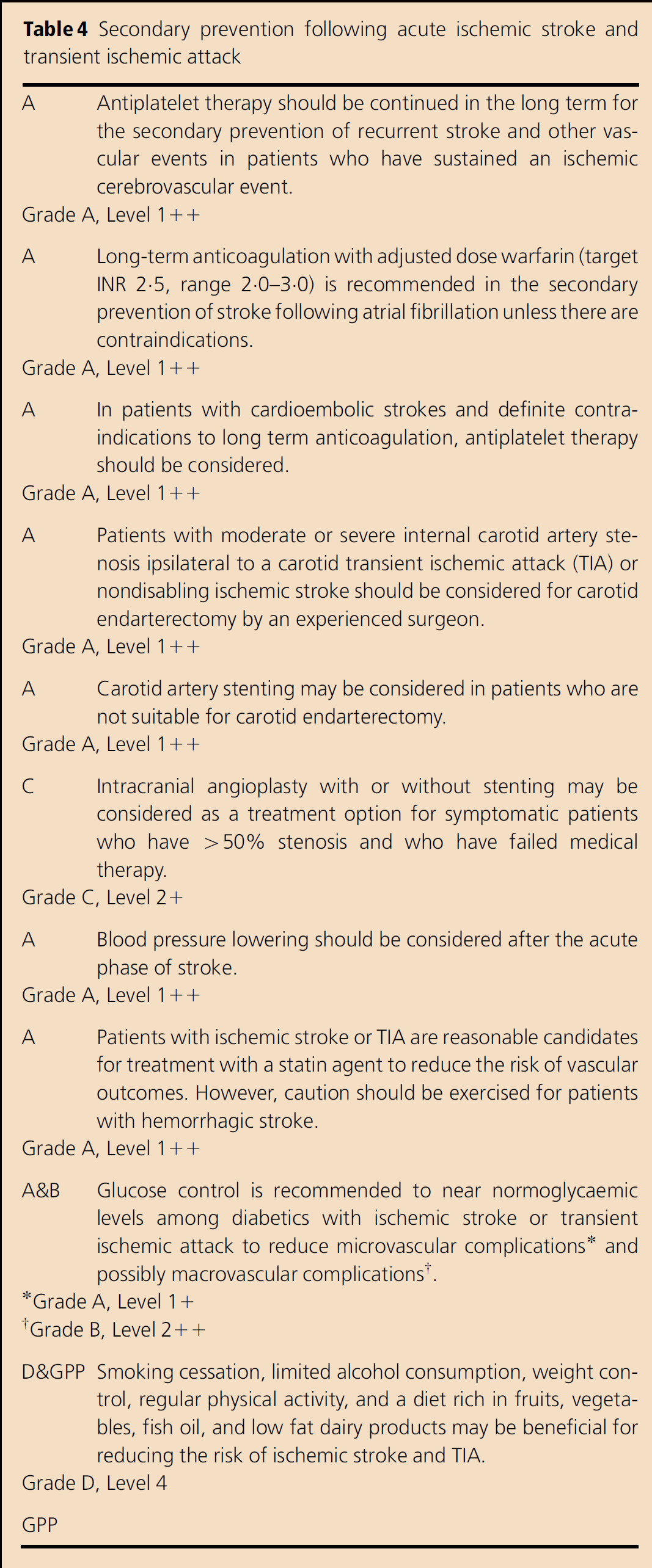
Secondary prevention (Table 4)
Antiplatelet therapy
Long-term antiplatelet therapy reduces the risk of serious vascular events (recurrent stroke, myocardial infarction, or vascular death) following an ischemic stroke or TIA (37).
Aspirin was the most widely studied antiplatelet drug, with doses of 75–150 mg/day being at least as effective as higher daily doses. The effects of doses lower than 75 mg/day were less certain (37).
Other beneficial antiplatelet agents include ticlopidine, clopidogrel, and dipyridamole (alone or in combination with aspirin) (37). Clopidogrel or the combination of aspirin and dipyridamole may be superior to aspirin alone (37, 38).
The combination of aspirin and clopidogrel is not superior to aspirin or clopidogrel alone (39, 40).
Anticoagulation therapy
Long-term anticoagulation with adjusted dose warfarin (target INR 2.5, range 2·0–3·0) is indicated for secondary prevention if atrial fibrillation is present, unless there are contraindications (41). A lower target INR of 2·0 (range 1·6–2·5) may be preferred in frail elderly (>75 years old) patients or who have an increased risk of hemorrhagic complications (41). In patients with definite contraindications to long-term anticoagulation, antiplatelet therapy should be considered (41, 42).
Carotid endarterectomy (CEA)
When combined with aspirin, CEA reduces recurrence risk, compared to taking aspirin alone, in patients with 70–99% North American Symptomatic Carotid Endarterectomy Trial (NASCET)-measured internal carotid stenosis ipsilateral to a carotid territory TIA or nondisabling ischemic stroke (43). CEA may also benefit selected high-risk patients with symptomatic 50–69% (NASCET-measured) stenosis. The benefit is generalizable only to surgically-fit patients operated on by surgeons with acceptable complication rates.
Carotid artery stenting (CAS)
There is still controversy as to whether CAS is as effective as CEA for secondary prevention in patients with severe carotid artery stenosis (44–47). CAS is reasonable when performed with operative morbidity and mortality rates of 4–6%, similar to that observed in trials of CEA.
Intracranial angioplasty and stenting
Patients presenting with severe intracranial stenosis experience an ipsilateral stroke despite treatment with either warfarin or aspirin (48).
Intracranial stents are deployable successfully, with an acceptable procedural death and ipsilateral stroke rates (49–51).
Blood pressure lowering
While aggressive lowering of mild to moderate elevated blood pressure is not recommended during the acute phase, subsequent blood pressure reduction results in a further reduction of vascular events (52, 53). The benefit is seen in both ischemic and hemorrhagic stroke, in both hypertensive and nonhypertensive subjects (53).
Lipids
Statins reduce vascular events among patients with stroke or TIA (54, 55).
Diabetes
There are no dedicated secondary prevention trials focusing on antidiabetic therapy; hypoglycaemic agents (in particular, metformin in over-weight subjects) are helpful in prevention (56). Hence, glucose control is recommended to near normoglycaemic levels among diabetics with ischemic stroke or TIA to reduce microvascular complications and possibly macrovascular complications (57).
Lifestyle modification
Diet rich in fruits, vegetables, fish oil, and low fat dairy products may be beneficial for reducing ischemic stroke or TIA risk (58, 59).
Elevated stroke risk due to smoking declines after quitting and is eliminated after five-years (60). Smoking cessation is recommended for patients with stroke or TIA.
Drinking one to two drinks per day appears to reduce risk of ischemic stroke, while heavy drinking increases the risk (61). Patients with stroke or TIA who are heavy drinkers should eliminate or reduce alcohol consumption.
Obesity is associated with stroke susceptibility (62). Patients who are overweight with ischemic stroke and TIA should attempt weight reduction.
Increased physical activity is protective against stroke (63). Patients who are capable of exercise after stroke or TIA should maintain moderate intensity physical exercise most days of the week for at least 30 min.
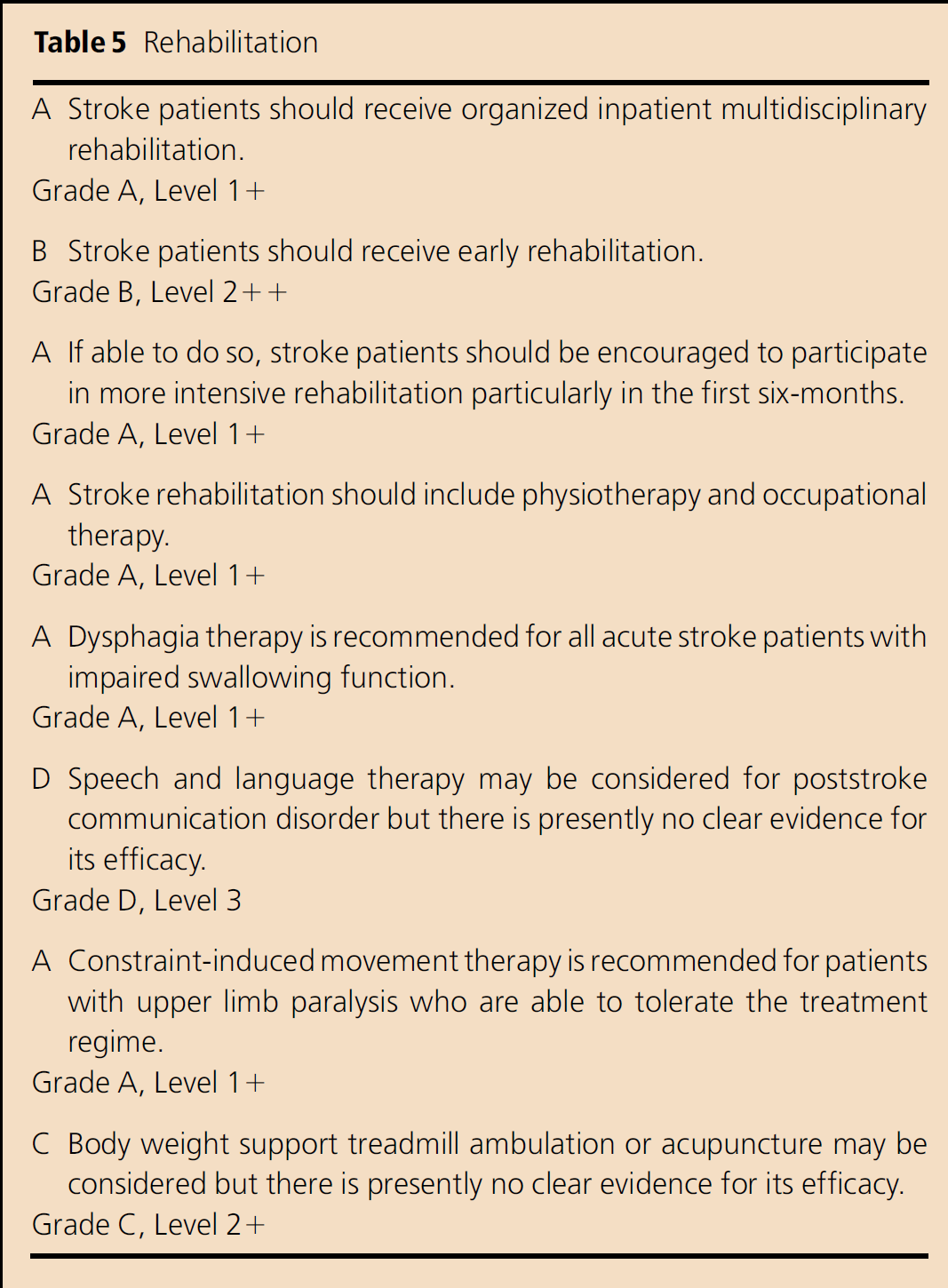
Rehabilitation (Table 5)
Organized inpatient multidisciplinary rehabilitation is associated with reduced odds of death, institutionalization and dependency (64).
Patients with acute stroke benefit from early initiation of stroke rehabilitation, with better functional outcome and shorter length of stay (65–67).
More intensive and longer rehabilitation therapy during the first six-months poststroke has a small but favorable effect on functional outcome (67, 68).
In-hospital care pathways result in no significant differences in death, dependency, or discharge destination. Care pathway patients are less likely to suffer urinary tract infection or be readmitted to hospital, and are more likely to have CT brain or carotid duplex scans. However, patient satisfaction and quality of life may be significantly lower, with no significant difference in length of stay (69).
A mixed physiotherapy approach for promoting postural control and lower limb function is significantly more effective than no treatment at improving functional independence (70).
Occupational therapy interventions reduces odds of a poor outcome, and increases activity of daily living (ADL) scores – patients are less likely to deteriorate and more likely to be independent in ADLs (71).
Dysphagic patients with dietary modification and taught swallowing compensation strategies have increased return to normal diet and recovery of swallowing by six-months, especially with a high-intensity program (72).
The efficacy of formal speech and language therapy on poststroke communication disorders including aphasia, speech apraxia, and dysarthria have not been clearly determined (73–75).
There may be substantial and long-lasting improvement in functional use of the paretic upper limb with constraint-induced movement therapy (76, 77).
There are no statistically significant differences between treadmill training, with or without body weight support, and other interventions for walking speed or dependence. Subjects who could walk independently at the start of treatment tend to have higher walking speeds, and dependent walkers tend to do better with treadmill training using body weight support (78).
A systematic review of randomized unconfounded clinical trials in sub-acute and chronic stroke subjects comparing acupuncture needling with placebo, sham, or no acupuncture found no trials with adequate methodological quality (79).
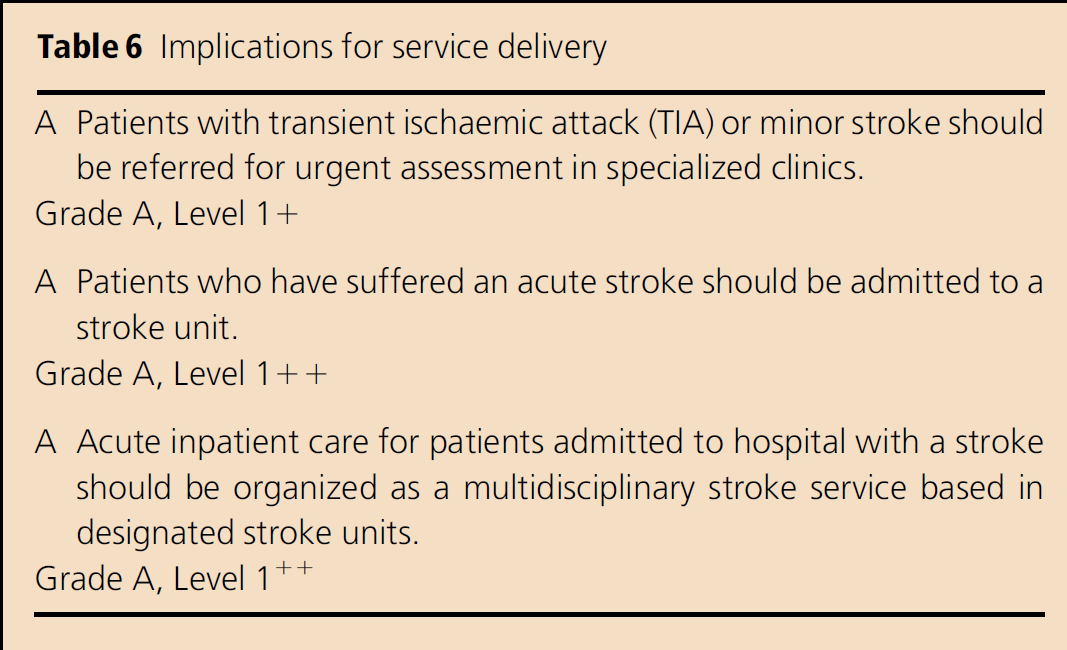
Implications for service delivery (Table 6)
Stroke assessment clinics
Stroke clinics facilitate the outpatient evaluation of suspected stroke/TIA patients, as well as the follow-up of stroke patients. Early initiation of existing treatments is associated with a reduction in the risk of early recurrence (80). Use of TIA clinics with 24 h access and immediate initiation of preventive treatment might reduce length of hospital stay and stroke risk (81).
Admission policies
Compared with general medical units, the management of stroke patients in a stroke unit reduces death, death or disability, and death or institutionalization. More patients are discharged home and remain at home (5). Benefits occur by reducing death from secondary complications and reducing the need for institutional care through a reduction in disability (82).
In the majority of these trials, care was provided in a designated area or ward, as opposed to a roving stroke care team. Members of the multidisciplinary team could include nurses, physiotherapists, occupational therapists, speech therapists, dieticians, medical social workers, case managers, and patient educators.
Organization of care for patients
Systems of care, including primordial and primary prevention, community education, notification and response of emergency medical services, acute treatment, sub-acute treatment and secondary prevention, rehabilitation, and continuous quality improvement activities must be established (83).
Important components of primary stroke centers are acute stroke team, written care protocols, emergency medical services, emergency department, stroke unit, neurosurgical service, commitment and support of medical organization, neuroimaging services, laboratory services, outcome and quality assessment activities, and continuing medical education (84). Comprehensive stroke centers should integrate expert health care personnel, advanced neuroimaging capabilities, surgical and endovascular techniques, and other specific infrastructure and programmatic elements such as an intensive care unit and a stroke registry (85).
Clinical quality improvement
The following clinical quality improvement parameters, based on the recommendations in this guideline, are proposed:
Proportion of stroke patients admitted to the stroke unit Proportion of stroke patients undergoing CT or MRI head within 24 h of admission Proportion of stroke patients undergoing screening for swallowing disorders Proportion of patients with noncardioembolic stroke started on antiplatelet medication at discharge Proportion of stroke patients with atrial fibrillation started on anticoagulation at discharge Proportion of stroke patients with hyperlipidemia started on statin therapy at discharge Proportion of eligible stroke patients receiving intravenous rtPA therapy Proportion of patients screened for need of inpatient multidisciplinary stroke rehabilitation Proportion of patients with TIA or minor stroke presenting to outpatient clinics who are referred for urgent assessment in specialized clinics or emergency departments.
Footnotes
Appendix
Workgroup and guideline development members: CoChairmen: Christopher Chen Li-Hsian, Lee Sze Haur.
Members: Bernard Chan, N. Venketasubramanian Ramani, Lee Kim En, Tang Kok Foo, John Thomas, Ivan Ng, Sitoh Yih Yian, Winston Lim, Lim Su Chi, Matthew Ng, Teo Wee Siong, Peter Lim Ai Chi, Winnie Tang, Ann Yin, Christopher Kuah.
Subsidiary editors: Pwee Keng Ho, Celeste Ong.