
Abstract
Background
Among patients with a patent foramen ovale and cryptogenic ischemic stroke, the long-term prognosis is unclear.
Aims
This study aims to estimate the recurrence rate in young cryptogenic stroke patients with and without patent foramen ovale.
Patients and methods
One hundred eighty-six cryptogenic stroke patients (aged 18–45 years) were prospectively followed for up to five-years. They were divided into two groups according to the echocardiographic presence of patent foramen ovale. All patients received aspirin (100mg/day) for secondary prevention.
Results
Mean age was 32·3 (standard deviation 7·9) years. During the mean follow-up of 66 months five patients with patent foramen ovale had recurrent strokes compared with 11 patients without patent foramen ovale. The average annual rate of recurrent cerebral ischemia was 1·1% and 1·6% for patients with and without patent foramen ovale, respectively. The recurrence rate did not increase with the presence of patent foramen ovale, atrial septal aneurysm or other variables. More than 60% of the reported cases achieved a good functional outcome.
Conclusions
Young patients with cryptogenic ischemic stroke with and without patent foramen ovale have a low recurrence rate in a long-term follow-up and most present a favorable outcome. Patent foramen ovale with or without atrial septal aneurysm did not increase the risk of recurrence.
Introduction
Patent foramen ovale (PFO) has been associated with stroke, especially with cryptogenic stroke, or stroke of undefined cause, which accounts for up to 40% of all ischemic stroke (IS) (1).
Among patients with a PFO and prior cryptogenic ischemic stroke (CIS) or transient ischemic attack, the absolute rate of recurrent events is variable (2,–5). Recently, a systematic review and meta-analysis (6) showed that the available evidence does not support an increased relative risk of recurrent ischemic events in those with a PFO vs. those without a PFO. Evaluating the risk of long-term recurrence is paramount in constructing therapeutic plans for these patients. Our aim was to estimate the long-term risk of stroke recurrence in patients younger than 45 with CIS, with or without a PFO, and determine which associated risk factors might increase the risk of recurrence.
Patients and methods
We analyzed data from 186 patients younger than 45 who were diagnosed with CIS. The data were prospectively collected in the stroke clinic database at the National Institute of Neurology in Mexico City, over a period of time beginning in January 1990. The database captures a standardized protocol of 186 variables, including demographics, vascular risk factors, clinical findings, laboratory, and imaging results as well as complications and functional outcomes posthospital discharge. To date, this registry includes 4400 cases with a median age of 52·3 ±18·6 years; among these, 67·9% are IS, and 36% (n = 1616) were younger than 45.
We defined CIS (1) as
acute neurological deficits lasting longer than 24 h
imaging studies with either magnetic resonance imaging (MRI) or computerized tomography (CT) scans corroborating the presence of ischemic events, and
absence of vascular pathology (intra- and extracranial) as well as other cardiac sources of emboli and prothrombotic states that could have been responsible for the IS; diagnosis of CIS was made by the treating physician.
The following disorders were considered to be definite causes of IS and led to exclusion (7): large artery atherosclerosis (defined by stenosis at least 50% or occlusion of the corresponding vessel); lacunar stroke (defined by a small, deep infarct <15 mm in diameter in a patient with hypertension); cardioembolic causes such as atrial fibrillation, rheumatic mitral stenosis, mitral, or aortic vegetations or prostheses; and other definite causes of stroke such as nonatherosclerotic arteriopathies (e.g. dissection), coagulopathies, hematologic or systemic disorders (e.g. antiphospholipid antibody syndrome).
For each patient the clinical, laboratory, and imaging data were reviewed by at least two neurologists.
Data collection
All stroke patients admitted to our hospital since January 1990 were registered and included in our database. We systematically collected information regarding vascular risk factors; history of previous vascular events or previous neurological problems and the results of MRI or CTscans. Prothrombotic profiles querying the levels of protein S, protein C, antithrombin III, antiphospholipid antibodies, and anti-B2 glycoprotein were routinely requested for this age group and added to the registry. In the first week after stroke, a 12-lead EKG, 24 h telemetry, and at least one of the following procedures were performed: a conventional cerebral angiogram, a transcranial Doppler, or a magnetic resonance angiogram (MRA) of extracranial arteries along with carotid ultrasound. The decision to perform additional tests to rule out deep venous thrombosis (DVT) was considered on a patient-by-patient basis.
Echocardiogram
A 2D transthoracic echocardiogram (TTE) with a bubble test was performed in all patients to rule out a cardiogenic cause of emboli, and the presence or absence of PFO and atrial septal aneurysm (ASA) was established. All tests were performed between the first and fourth weeks after stroke by two echocardiogram-trained cardiologists a routine protocol. This protocol initially includes a routine TTE, and once the possibility of structural pathology related to cardiac embolism are ruled out, a saline-bubble test is performed by injecting agitated saline solutions through a peripheral vein. The test was performed twice at rest and twice again during a Valsalva maneuver. A positive right to left shunt is observed when microbubbles are detected in the left chambers during the first five beats after saline administration (8). In the case of optimal acoustic window, and a complete opacification of the right chambers during Valsalva maneuver, TTE was considered conclusive (8). In the case of negative test results (absence of bubbles in left chambers), or a poor thoracic window, a transesophageal echocardiogram (TEE) with a bubble test was performed. In contrast, TTE is a very specific technique, whose major advantage is the ability to detect right-to-left shunt, particularly if associated with an ASA (9).
The diagnosis of ASA was determined as bulging of the oval fossa membrane of both atrium chambers measuring more than 10 mm with a base of 14 mm (8,9).
Other tests
Prothrombotic screens were performed three-months after each event and repeated six-months later. In all cases, either a carotid Doppler or CT/MR angiogram of extra- and intracranial vessels was also performed.
Treatment and follow-up
Owing to weak evidence-based data supporting anticoagulation in our Institution, all our patients with PFO were managed with aspirin for secondary stroke prevention.
Follow-up was done in person, by telephone interviews or by medical chart review; follow-up periods varied from six-months to a year. Specific questions concerning therapy, compliance, disability, and any recurrent IS or vascular event were evaluated.
The primary end-point of the study was recurrent IS; defined as a recurrent neurological deficit lasting more than 24 h in a different territory or location compared with the baseline stroke, worsening of an already known deficit corroborated by CT or MRI, extension of previous lesions or the presence of new ischemic events.
Disability six-months and at the end of the follow-up was assessed by using the modified Rankin scale (mRS); a score of 0–2 in this scale was considered good.
Statistical analysis
Data analysis was performed with the statistical package SPSS 17. Clinical, demographic, and imaging data were compared between patients with and without a PFO (with and without ASA). Group comparisons were performed with an χ2-test (the Yates correction for continuity was used when necessary), Fisher's exact test, or Student's t-test. The time/risk contribution of each subject was taken into consideration using the population time (the sum of the duration of the follow-up for all N recurrent stroke-free subjects). Multivariate logistic regression analysis was used to determine factors associated with a PFO and outcome. Kaplan–Meier survival curves were used to evaluate the absolute risk of recurrent events. Average annual event rates were calculated according to the formula 1-(1-P)1/n, where P equals the cumulative event rate at n years of follow up (10). The predictive value of each variable on the outcome was analyzed with the proportional risk Cox model.
Results
Until July 2008, 4400 consecutive new patients entered into our database, 254 cases were diagnosed as CIS. We excluded 25 patients due to questionable prothrombotic screening results; 23 due to lack of study completion, 19 died during the acute phase, and one because the PFO was surgically repaired.
A total of 186 patients with a median age of 32·3±7·9 (16–45 years) were followed (98 women, 88 men). Eighty-five of these (45·7%) had PFO, and 101 (54·3%) did not have any echocardiographic lesion. In 24 (13%) cases with a PFO, ASA was also associated. Patient baseline characteristics are shown in Table 1.
Patients' characteristics and demographics among groups
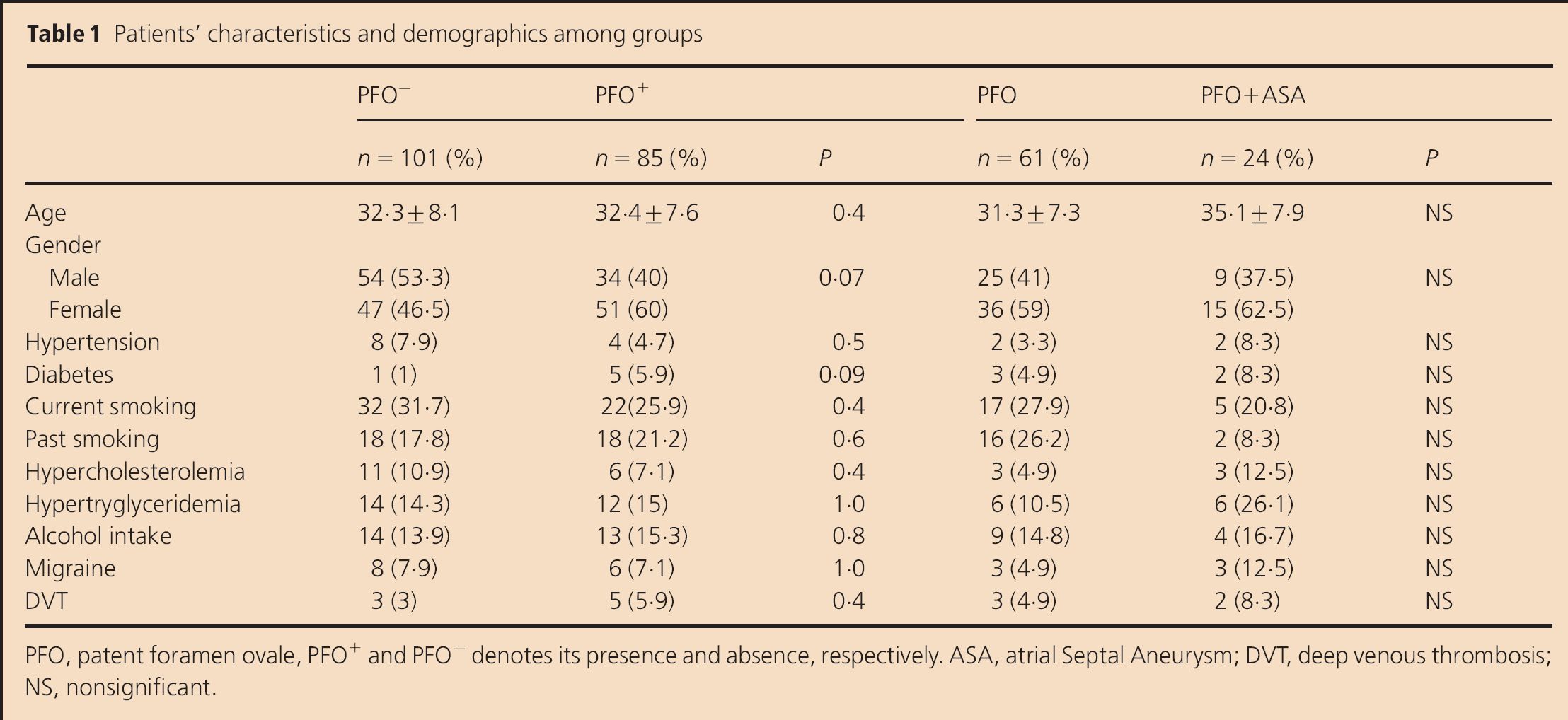
PFO, patent foramen ovale, PFO+ and PFO- denotes its presence and absence, respectively. ASA, atrial Septal Aneurysm; DVT, deep venous thrombosis; NS, nonsignificant.
A CTscan of the brain was done in all cases; brain MRI was also performed in 174 patients to corroborate ischemic lesions. The carotid arteries were evaluated with an MRA in 90 patients (48·4%), a conventional digital-subtraction angiogram in 92 (49·5%) and carotid Doppler in 69 (37·1%). All patients underwent a TTE for the diagnosis of PFO, and in 65 (76·5%) cases, a TEE was required to diagnose PFO. In 30 patients without shunt evidence, the contrast TTE was considered conclusive as has been described previously. The characteristics of this group were an optimal acoustic window, use of harmonic frequencies and a complete opacification of the right chambers during Valsalva maneuver.
The carotid territory was the most heavily affected area in 56 patients (66%) with PFO and 73 (73%) without PFO. Cortical, sub-cortical, and cortico-sub-cortical regions were equally affected in both groups.
In some patients, a history of DVT was recorded, though no significant differences were seen between groups and DVT was not detected in any of the patients.
The follow-up time ranged from 12 to 160 months, with an average of 66 months.
During the follow-up, five recurrent IS were seen in patients with PFO (399 person/year) and 11 recurrent IS were observed in patients without PFO (356 persons/year). The average annual rate of recurrent cerebral ischemia was 1·1% and 1·6% for patients with and without PFO, respectively (Fig. 1).
The Cox analysis did not reveal any predictive variable related to recurrence, nor was the presence of ASA associated with the presence of PFO.
The functional outcome at discharge was good in both groups: 55 patients (54·5%) without PFO and 49 (57·6%) with PFO had a mRS of 0–2 (P = 0·76). These numbers increased in the final assessment to 66 (65·3%) and 62 (72·9%), respectively (P = 0·34). None of the patients died.
Discussion
Even though the association of a PFO and ASA has been established as a cause of IS in young patients, there exists little data to support its relevance with respect to recurrence rate (11,–13). The present study has a prospective design, and was performed in one institution with strict inclusion and exclusion criteria protocol with long-term follow-ups. Also, our series only included patients younger than 45 years in an effort to minimize the presence of other risk factors associated with other mechanisms of IS. Our results confirm previous studies (2,4,12,13) that found low recurrence rates in patients with and without a PFO. Prospective studies, such as ours have shown that the risk of recurrence is low regardless of medical management (5,12–14).
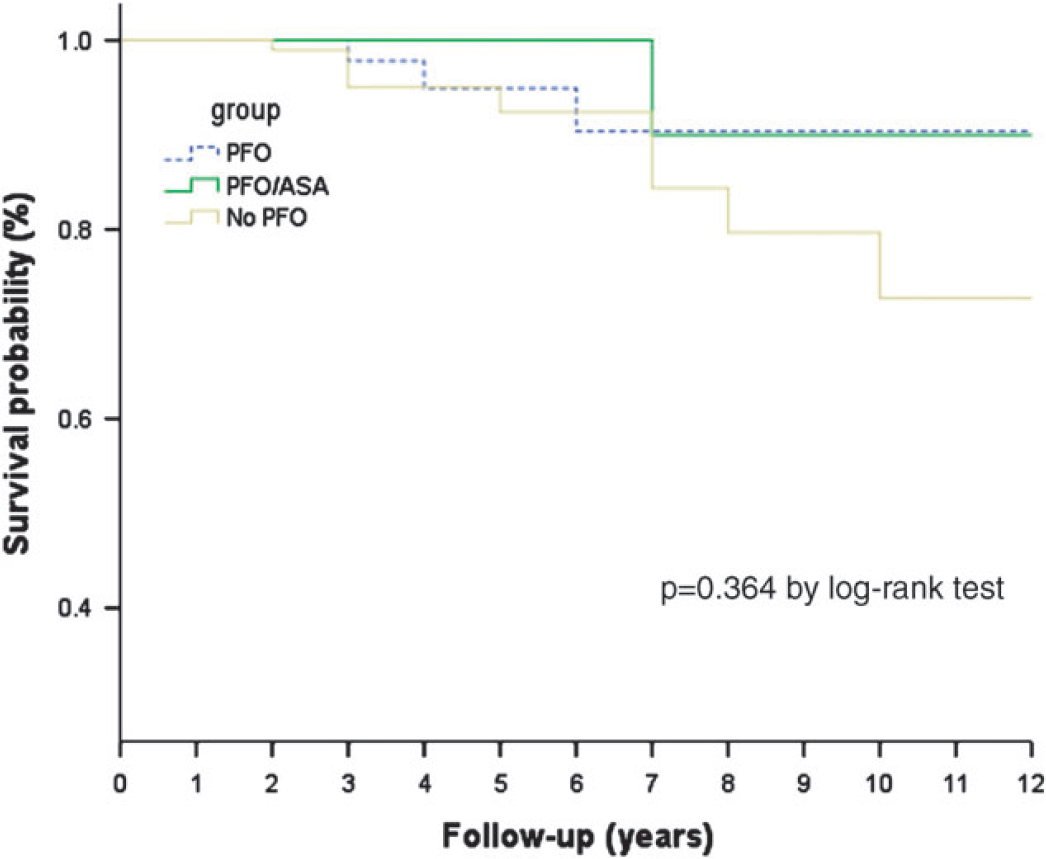
Kaplan–Meier event-free survival curves for recurrence over follow-up. ASA, atrial septal aneurysm; PFO, patent foramen ovale.
The length of follow-up of our study was significantly longer than previous studies, and interestingly, the results are quite similar, suggesting that the natural history of young patients with PFO (with or without ASA) is not modified over time. However, PFO by itself is an inadequate predictor for the first occurrence of IS due to its high prevalence in the general population, which has been estimated at 30% (15), and because other risks certainly contribute to its emboligenic potential (16).
Our study also demonstrated a lack of association between ASA and a PFO in stroke risk recurrence and, interestingly, neither of these associations played a role in the functional outcome, which was good in most patients. This result may be explained by the age of our study group, the lack of traditional risk factors, and absence of concomitant brain pathologies. As per Lamy et al. (17), the clinical and imaging characteristics of our patients suggested an embolic mechanism. We excluded potential embolic cardiac causes and prothrombotic states. However, some authors (17,–19) have suggested that the mechanism of an infarct in patients with PFO could be related to the presence of paroxystic arrhythmias, which were not evaluated but definitely warrant future study.
Possibly the major limitation of our study is its poor statistical power due to the limited number of recurrent events. This outcome could have been the result of our strict selection criteria, as we only included patients who had been completely evaluated. However, in our opinion, this is the best way to demonstrate causality due to this vestige of fetal circulation on ischemic recurrence. Other possible weaknesses of our study were the lack of longer time-cardiac recording studies (e.g. 48 h telemetry/Holter monitoring) and not including the presence of aortic arch atherosclerosis in our database. Notwithstanding, within the latest, the authors consider this to be extremely rare in the age group studied. Nevertheless, we consider the identified limitations to be extremely rare in the age group studied.
PFO is an important cause of cryptogenic stroke, especially among young patients. The fact of finding in our study low stroke recurrence rate, suggest that embolism through a PFO is a more complex phenomena than just the presence of a ‘hole.’ Our results are important and will play an important role in the secondary management of young patients with CIS. There is an extensive debate regarding the use of antiplatelets, anticoagulation or defect closure as a secondary prevention treatment. We feel that if recurrence is low in patients with PFO, more aggressive therapy might not be indicated. Therefore, means of identifying strong risk factors is important, so that novel therapies can be considered.
Conclusion
Young patients with CIS with and without a PFO have a low recurrence rate in a long follow-up and present a high favorable outcome. Patent foramen ovale with or without ASA did not increase the risk of recurrence.