
Abstract
Abstract
Constraint-induced movement therapy is a commonly used intervention to improve upper limb function after stroke. However, the effectiveness of constraint-induced movement therapy and its optimal dosage during acute or sub-acute stroke is still under debate. To examine the literature on the effects of constraint-induced movement therapy in acute or sub-acute stroke. A literature search was performed to identify randomized, controlled trials; studies with the same outcome measure were pooled by calculating the mean difference. Separate quantitative analyses for high-intensity and low-intensity constraint-induced movement therapy were applied when possible. Five randomized, controlled trials were included, comprising 106 participants. The meta-analysis demonstrated significant mean differences in favor of constraint-induced movement therapy for the Fugl–Meyer arm, the Action Research Arm Test, the Motor Activity Log, Quality of Movement and the Grooved Pegboard Test. Nonsignificant mean difference in favor of constraint-induced movement therapy were found for the Motor Activity Log, Amount of Use. Separate analyses for high-intensity and low-intensity constraint-induced movement therapy resulted in significant favorable mean differences for low-intensity constraint-induced movement therapy for all outcome measures, in contrast to high-intensity constraint-induced movement therapy. This meta-analysis demonstrates a trend toward positive effects of high-intensity and low-intensity constraint-induced movement therapy in acute or sub-acute stroke, but also suggests that low-intensity constraint-induced movement therapy may be more beneficial during this period than high-intensity constraint-induced movement therapy. However, these results were based on a small number of studies. Therefore, more trials are needed applying different doses of therapy early after stroke and a better understanding is needed about the different time windows in which underlying mechanisms of recovery operate.
Introduction
Stroke is one of the main causes of disability in the western world (1). Although most patients show significant gains in motor function early after stroke onset (2), a large proportion still show significant long-term impairments of upper limb function, limitations of activities and restrictions in social participation after stroke (2,–4).
Constraint-induced movement therapy (CIMT) is a neurorehabilitation approach developed to improve the use of the more affected upper limb after stroke. The original therapy involves inducing the use of the more affected limb by constraining the less affected limb for up to 90% of waking hours over a two-week period, including two weekends. During this period, repetitive training of the more affected limb using shaping principles is applied for six-hours on each weekday (5).
On the basis of a systematic review involving 19 randomized controlled trials (RCTs) (N = 619), Sirtori et al. (6) concluded that CIMT is an effective therapy for improving upper limb function and ADLs outcomes. However, the application of CIMT is heterogeneous and several modified forms of CIMT ((m)CIMT) have been advocated in the literature. These modified forms are generally characterized by less time dedicated to shaping procedures as well as less constraining time of the less affected limb.
One aspect that is particularly debated in the literature is the optimal dosage of (m)CIMT that is started in the first days and weeks poststroke (7,–10). For example, several animal studies (7, 9, 10) have shown that early exclusive use of the impaired forelimb within the first seven- to 15 days postischemic stroke may increase the lesion volume (9, 10), may have detrimental effects on sensorimotor function (7) and may result in chronic behavioral deficits (7, 9, 10). In line with this finding, the VECTORS study (8) found a negative dose–response relationship for early (m)CIMT therapy in stroke patients starting 10 days poststroke. Their results showed that a CIMT application involving three-hours of shaping on every workday in combination with constraining the less affected limb for 90% of the waking hours for every day, including weekends for a period of two-weeks led to significantly less upper extremity motor improvement at 90 days than two-hours of shaping therapy and six-hours of restraining per day. On the other hand, some studies also suggest that there may be a critical time window of heightened reactive neuroplasticity by up-regulation of growth promoting factors during the process of spontaneous neurological recovery in the first few weeks poststroke (11, 12).
The purpose of the present review was to systematically review the literature on the effects of (m)CIMT on the upper limb motor function in patients with acute or sub-acute stroke. Sensitivity analysis was used to investigate the impact of the (m)CIMT dosage in acute or sub-acute stroke. Although we hypothesized that the use of (m)CIMT would have a positive effect on upper limb function, we also expected that a lower dose of (m) CIMT would be more beneficial than the traditional form of CIMT during the acute or sub-acute phase after stroke.
Methods and materials
Definitions
Stroke has been defined by the World Health Organization as ‘a clinical syndrome typified by rapidly developing signs of focal or global disturbance of cerebral functions, lasting more than 24 h or leading to death, with no apparent causes other than of vascular origin’ (13).
In the present review, the acute or sub-acute phase was defined as the time window in which time-dependent spontaneous neurological recovery still occurs, which is typically within the first 10 weeks after stroke onset (12).
To investigate the impact of the (m)CIMT dosage during acute or sub-acute stroke, the interventions that were included in this review were categorized as ‘high–intensity CIMT’ (HI CIMT) or ‘low–intensity CIMT’ (LO CIMT). In line with the VECTORS study (8), HI CIMT was defined as three-hours or more of shaping therapy per day in combination with restraining of the less affected limb for 90% of waking hours, whereas LO CIMT was defined as less than three-hours of shaping therapy per day and constraining of the less affected limb for less than 90% of waking hours.
Study identification
Potentially relevant literature was identified through computerized and manual searches. The following electronic databases were systematically searched through December 2010: PubMed, EMBASE, Cochrane Central Register of Controlled Trials, CINAHL, Physiotherapy Evidence Database (PEDro), WHO ICTRP trial register and EBSCO/SportDiscusTM. The following MeSH headings and key words were used: stroke, cerebrovascular accident, constraint induced therapy, forced use and RCT. Additional relevant studies were identified by examining bibliographies of review articles as well as references from retrieved articles. Studies published up to December 2010 were included if they met the following inclusion criteria:
the study was a RCT
CIMT was applied focusing on the upper limb
participants were patients with stroke who were at least 18 years of age
participants were recruited and observed within the acute or sub-acute phase after stroke onset, and
the study was published in English, German or Dutch.
Two authors (J. B. and R. N.) independently reviewed the titles of the identified references, selected the relevant studies on the basis of title and abstract and subsequently checked independently if the selected studies satisfied the inclusion criteria. If a study that did not provide conclusive information in the abstract, the full text was retrieved and reviewed. Disagreements were resolved by consensus, and a third review author (G. K.) was consulted when disagreements persisted.
Methodological quality
Two independent reviewers (J. B., R. N.) assessed the methodological quality of each RCT using the PEDro scale (14). PEDro is a reliable and valid scale consisting of 11 items, in which the first item relates to external validity and the other 10 items assess the internal validity of a clinical trial. One point was given for each criterion that was satisfied (except for the first item, which was allocated a YES or NO), yielding a maximum score of 10. The higher the score, the better the quality of the study. PEDro scores ≥ 4 points were classified as ‘high quality,’ whereas studies with ≤ 3 points were classified as ‘low quality’ (15). Low-quality studies were excluded from the current review. Reviewers were not blinded to authors, journals or outcomes. Agreement regarding each item was evaluated by calculating a κ statistic. In case of disagreement, consensus was sought, but when disagreement persisted, a third independent reviewer (G. K.) made the final decision.
Quantitative analysis
Two reviewers independently checked the extracted data (i.e. the numbers of patients in the experimental and control groups and the mean and standard deviation (SD) of postintervention scores for each intervention group). For each outcome variable, the results were pooled by calculating the mean difference (MD) and 95% confidence intervals (Cis) when outcomes were reported on the same scale. When outcomes were reported on different scales the standardized mean difference (SMD) was calculated. Mean differences or SMDs and the corresponding SDs were calculated using the difference in postintervention means between the experimental and the control groups. The χ2-test was used to test for homogeneity, set at a significance level of 10%. Because the χ2-test tends to underestimate heterogeneity in meta-analyses, I2 was calculated as well to provide an estimate of the percentage of variability due to heterogeneity rather than chance alone (16). If significant heterogeneity was found (I2 values ≥ 50%) a random effects model was applied (16). In case of statistical heterogeneity, a sensitivity analysis was considered for methodological quality with respect to randomization, allocation concealment, blinding of final outcome assessment, and use of intention-to-treat analysis. For all outcome variables, the critical value for rejecting H0 was two-tailed and set at a level of 0·05. The review manager 5 software package was used to calculate the MDs or SMDs and to visualize the results by using forest plots.
Sub-group analysis
Because the optimal dose of (m)CIMT when started in the first weeks poststroke is still under debate, separate quantitative analyses for HI CIMT and LO CIMT were applied if possible. MDs or SMDs could not be defined on outcome measures when only one study had applied HI or LO CIMT. However, to explore the differential effects of HI and LO CIMT, the data of such a single study are also presented in forest plots, while the difference between the experimental and the control groups within the study of interest is reported only as ‘difference.’
Results
Study identification
The search strategy yielded 1033 citations. The results of the electronic search strategy in different databases are available by the corresponding author. After selection based on title and abstract, 805 studies were excluded. Figure 1 shows the flow chart of identified studies that were considered for inclusion. Reasons for exclusion were that the interventions did not fit in with the definitions given above, or that studies had been conducted in a different patient population. Of the remaining 228 full-text articles, 160 were excluded because of inappropriate intervention or study design. Sixty-two studies were excluded because of recruitment outside the acute or sub-acute phase, and finally one study was excluded because of lack of quality (17). Screening of references did not yield any further studies. A total of five studies were included in this systematic review (8, 18–21), comprising 106 participants. In two studies, HI CIMT was compared with usual care (18, 21), two studies compared LO CIMT with usual care (19, 20) and one study compared HI CIMT with LO CIMT and usual care (8). The timing to start the intervention varied between studies from a mean of 4·4 days in the study by Page et al. (20), to a median of 11 days in the study by Boake et al. (18). The main characteristics of the included studies are shown in Table 1.
Characteristics of the studies included in this review
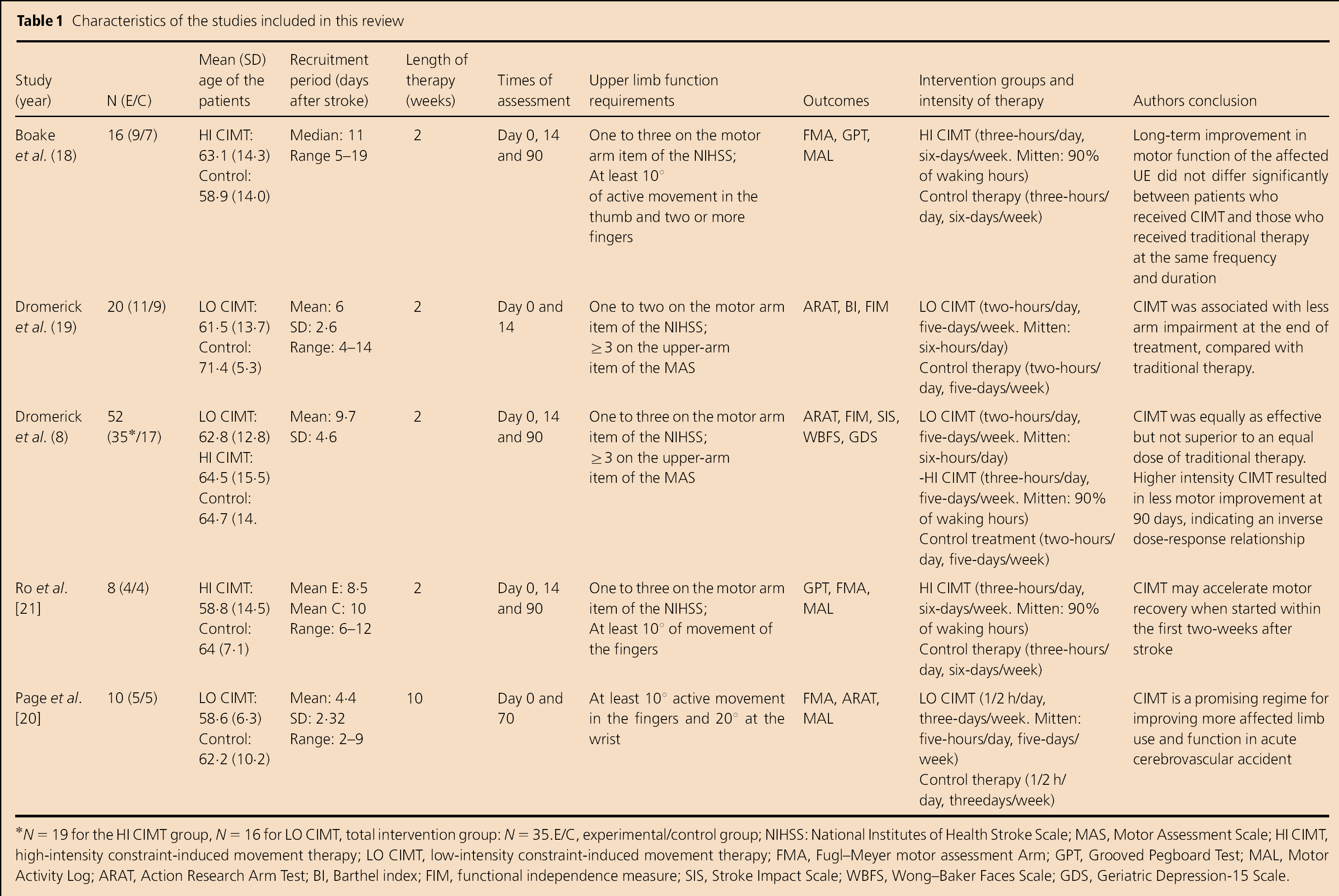
N = 19 for the HI CIMT group, N = 16 for LO CIMT, total intervention group: N = 35.E/C, experimental/control group; NIHSS: National Institutes of Health Stroke Scale; MAS, Motor Assessment Scale; HI CIMT, high-intensity constraint-induced movement therapy; LO CIMT, low-intensity constraint-induced movement therapy; FMA, Fugl–Meyer motor assessment Arm; GPT, Grooved Pegboard Test; MAL, Motor Activity Log; ARAT, Action Research Arm Test; Bl, Barthel index; FIM, functional independence measure; SIS, Stroke Impact Scale; WBFS, Wong–Baker Faces Scale; GDS, Geriatric Depression-15 Scale.
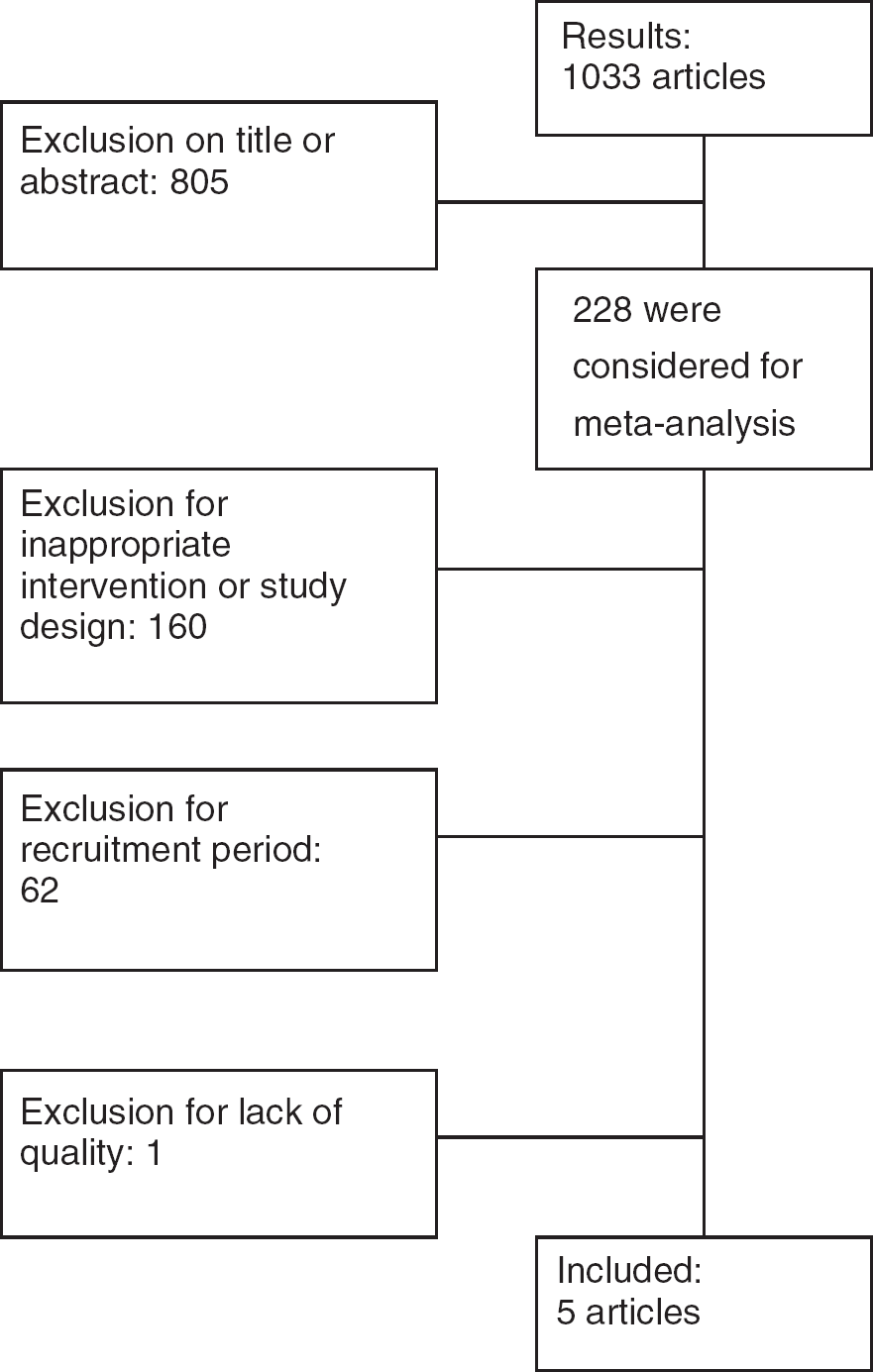
Flowchart of study identification.
Methodological quality
Table 2 shows the methodological quality scores of the included studies, according to the PEDro scale. The PEDro scores ranged from one to eight points, with a median score of 6·5 points. The assessment of the methodological quality using the 10-item PEDro scale resulted in a Cohen's κ of 0·75 between the two independent review authors. All studies, except that by Grotta et al. (17) scored at least six points on the PEDro scale. The study by Grotta et al. (17) was excluded from further analysis.
Methodological quality of the included trials, assessed with the 10-item PEDro scale
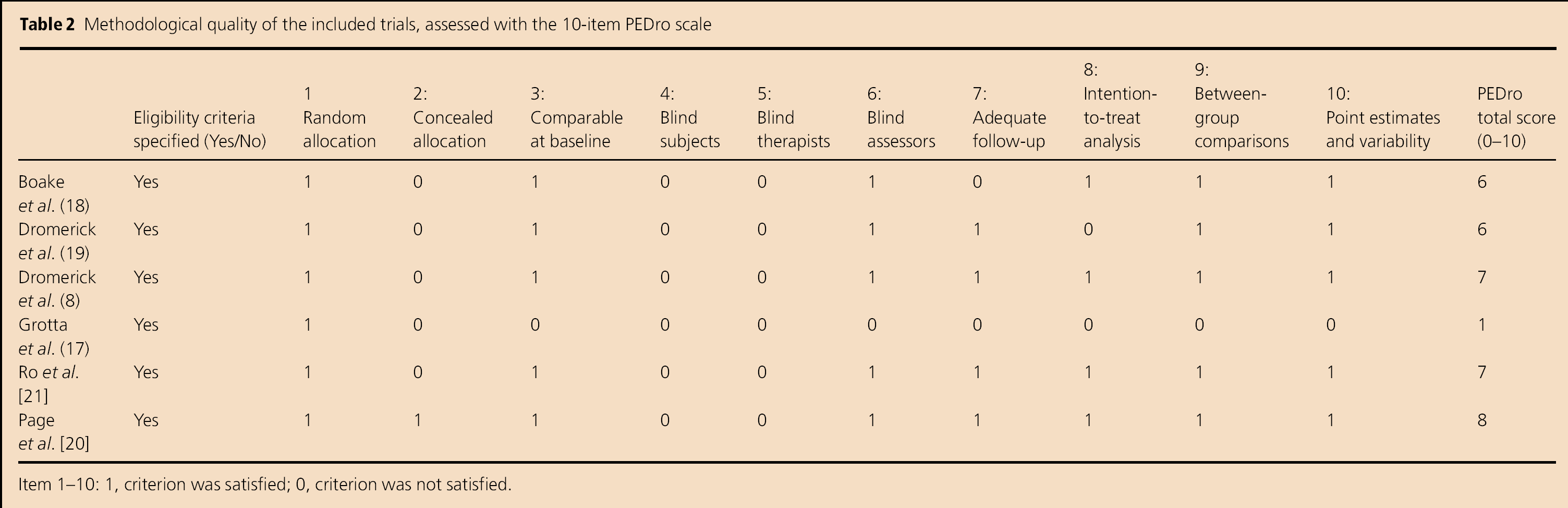
Item 1–10: 1, criterion was satisfied; 0, criterion was not satisfied.
Quantitative analysis
As results for all outcome variables were reported on the same scale, MDs were calculated. Pooling of outcomes was possible for
upper limb impairment, measured with the Fugl–Meyer motor assessment of the arm (FMA)
upper limb function, measured with the Action Research Arm Test (ARAT)
dexterity, measured with the Grooved Pegboard Test (GPT), and
perceived upper limb function, measured with the Motor Activity Log (MAL) for Amount of Use (AOU) and Quality of Movement (QOM).
FMA
Figure 2a shows a significant heterogeneous MD for the three studies that assessed the FMA (18, 20, 21) (MD (random): 11·00; 95% CI: 2·50–19·49; Z = 2·54; P = 0·01; I2 = 51%).
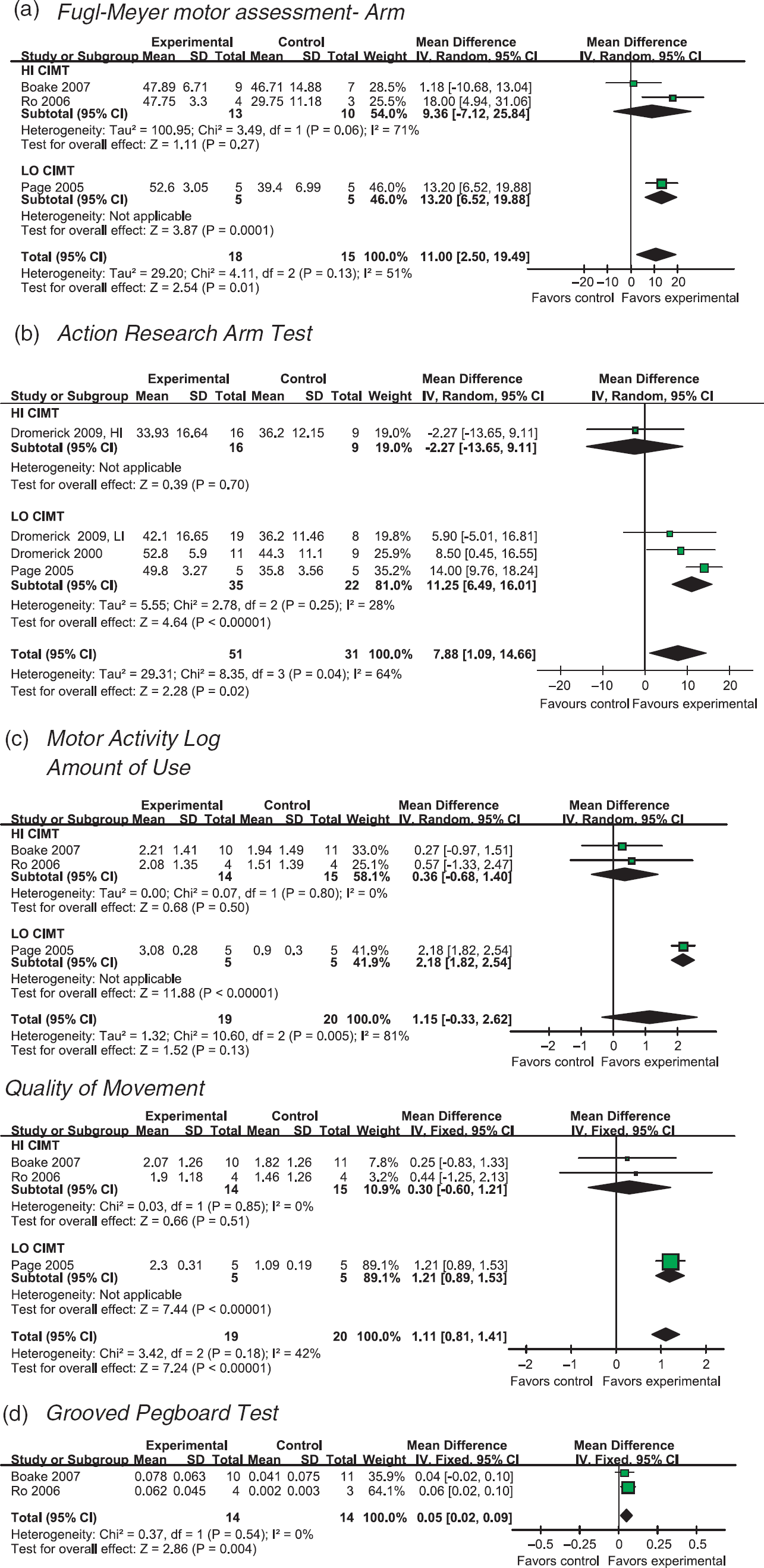
Meta-analysis of CIMT in the acute phase after stroke. (a) Fugl–Meyer motor assessment Arm. (b) Action Research Arm Test. (c) Motor Activity Log. (d) Grooved Pegboard Test.
The two studies that used HI CIMT yielded a nonsignificant MD (MD: 9·36; 95% CI: −7·12 to 25·84). The study that used LO CIMT yielded a significant difference in favor of the experimental group (difference: 13·20; 95% CI: 6·52–19·88).
ARAT
Three studies evaluated the effect of CIMT on the ARAT (8, 19, 20). The VECTORS study (8) included two separate trials, one in which HI CIMT was compared with a lower dose of traditional upper extremity (UE) therapy and one in which LO CIMT was compared with dose-matched traditional UE therapy.
Figure 2b shows a significant heterogeneous total MD on the ARAT (MD (random), 7·88; 95% CI: 1·09–14·66; Z = 2·28; P = 0·02; I2 = 64%;).
The study that used HI CIMT yielded a nonsignificant difference in favor of the control group (difference: −2·27; 95% CI: – 13·65 to 9·11). The three studies that used LO CIMT yielded a significant MD in favor of the experimental group (MD: 11·25; 95% CI: 6·49–16·01).
AOU and QOM of the MAL
Figure 2c shows that pooling the results of the three studies that assessed the MAL (18, 20, 21) yielded a nonsignificant heterogeneous MD for the AOU (MD (random): 1·15; 95% CI: −0·33 to 2·62; Z = 1·52; P = 0·13; I2 = 81%).
The two studies that used HI CIMTyielded a nonsignificant MD (MD: 0·36; 95% CI: −0·68 to 1·40). The study that used LO CIMT yielded a significant difference in favor of the experimental group (difference: 2·18; 95% CI: 1·82–2·54)
Figure 2c shows a significant homogeneous MD for the QOM (MD (fixed): 1·11; 95% CI 0·81–1·41; Z = 7·24; P < 0·001; I2 = 42%).
Pooling the two studies assessing QOM with a HI CIMT application resulted in a nonsignificant MD (MD: 0·30; 95% CI: −0·60 to 1·21). The study that used LO CIMT yielded a significant difference in favor of the experimental group (difference: 1·21; 95% CI: 0·89–1·53).
GPT
Figure 2d shows a significant homogeneous MD for the two studies (18, 21) that evaluated the GPT for dexterity (MD (fixed): 0·05; 95% CI: 0·02–0·09; Z = 2·86; P = 0·004; I2 = 0%). Both studies used HI CIMT.
Discussion
This systematic review, including five RCTs with a total of 106 participants, suggests an overall trend toward positive effects of LO and HI CIMT during the acute or sub-acute phase after stroke. Although MDs were not significant for all outcome measures, all total MDs (HI and LO CIMT combined) were in favor of the experimental group. Sub-group analyses for HI CIMT and LO CIMT resulted in positive and significant MDs for LO CIMT for all outcome measures, in contrast to HI CIMT. In line with the VECTORS study (8), in which the patients in the HI CIMT group showed even lower gains compared to those in the control group and to the LO CIMT group, the current meta-analysis suggests that LO CIMT may be more beneficial during the acute or sub-acute phase than HI CIMT. However, the sizes and number of included studies that evaluated the effects of CIMT during the acute or sub-acute phase were rather small. As a consequence, our drawn conclusions should be interpreted with caution, as the summarized findings can easily be overturned by one small neutral or negative study. In addition, the relatively small number of patients recruited for the included trials illustrates the difficulty of performing studies of this nature (22). For the VECTORS study (8), for instance more than 35 patients had to be screened for each enrolee (3%), whereas in the study by Ro et al. (21), eight (4%) out of the 187 screened patients enrolled in the trial, which also emphasizes the difficulty of generalizing the results (22). However, all participants enrolled in one of the studies completed the entire intervention period and most studies (18,–20) emphasized that implementation of the applied form of CIMT, which varied between 1·5 h and three-hours of therapy each day, is feasible in acute stroke rehabilitation.
Positive effects of CIMT were found at the activity level (ARAT, MAL, GPT) as well as at the impairment level (FM-arm) of the International Classification of Functioning, Disability and Health. However, scores at the activity level may also improve as a result of increased use of compensation strategies (23). Future studies should therefore investigate what exactly patients learn when they improve. On the other hand, although improvement on the FM arm purportedly reflects improvement at the impairment level, the FM-arm includes four sub-sections: shoulder-arm, wrist, hand and coordination (24), so it remains unclear what exactly changes when FM scores improve. For instance, evidence for favorable effects of (m)CIMT on hand function is still weak, so more differentiated research is required.
Between the included studies heterogeneity was found. One of the reasons for heterogeneity is the variation in the inclusion criteria concerning upper limb function, which differed between studies. Most studies required some proximal and distal voluntary activity (18, 20, 21), whereas both of the studies by Dromerick only required proximal activity (8, 19). As the presence of finger extension may reflect the intactness of some fibers of the corticospinal tract system in the affected hemisphere, finger extension is an important prognostic determinant for the outcome of upper limb function (25). Therefore, such differences in inclusion criteria might also have a substantial influence on the overall intervention effects. As the functional outcome of the upper limb is mainly determined by the skills of the hand and not by the transport function of the arm itself (26, 27), the presence of some distal hand function in terms of visible control of some finger (and/or thumb) extension at onset maybe conditional for a positive effect of CIMT. Another reason for heterogeneity might be the variation in the duration of therapy and constraining. For instance, the study by Page et al. (20) differed substantially from the others in terms of the length of therapy (i.e. 10 versus two-weeks). Additionally, the original CIMT protocol consist of three main elements:
repetitive, task oriented training
constraining use of the more affected upper limb and
a transfer package of adherence-enhancing behavioral methods to transfer gains made in the laboratory or clinical setting to the patient's real-world environment (28).
The first two elements are well described in all articles. But it is unclear how the studies have managed with the transfer package. Finally, although all studies recruited patients within two-weeks after stroke onset, the time because stroke onset varied between studies, from a mean of 4·4 days in the study by Page et al. (20) to a median of 11 days in the study by Boake et al. (18) As recovery mechanisms such as reperfusion, resolution of diaschisis and restitution of non-infarcted penumbral areas may play an important role in spontaneous neurological recovery during the first days post-stroke (29), small differences in the timing of the start of the study may not only have affected the rate of recruitment but also the probability of the sample to regain dexterity after stroke (25). The observed heterogeneity between the studies is probably not due to the methodological quality of the studies, as PEDro scores were more or less comparable. However, because of the heterogeneity and the variety in patient populations, caution is required when comparing studies and combining results.
The suggestion that a lower dose of CIMT may be more beneficial than a potentially harmful higher dose during the acute phase after stroke is largely based on the results of the VECTORS study (8). These finding are, however, supported by several animal studies (9, 10, 30, 31), which have found that intensive practice of the affected limb in rats is detrimental if it occurs too soon after the infarction, when cells in the penumbral tissue are presumably still vulnerable (32). For example, Kozlowski et al. (10) found a disrupted recovery of function after immobilization of the nonimpaired forelimb during the first 15 days (22). Additionally, Schallert et al. (31) showed that when rats with unilateral lesions of the forelimb area in the motor cortex were forced to use the affected limb for the first seven-days postinjury, the injury size increased in terms of a significantly greater loss of brain tissue compared with rats that were forced to use the affected limb from days eight to 15. These results suggest that the region surrounding an infarct is vulnerable ‘to behavioral pressure’ in the early days to weeks poststroke. In addition, Bland et al. (33) suggested that the effects of forced use of the affected arm during the first 10 days may differ depending on cortical or sub-cortical involvement. They found that overuse of the affected limb in rats with a distal middle cerebral artery occlusion, resulting in an exclusively cortical infarction, worsened the outcome. In contrast, in rats with a proximal middle cerebral artery occlusion, damaging striatal neurons, not overuse but disuse of the affected limb during the first 10 days worsened the outcome, whereas overuse of the affected limb had no effect. These results suggest that neurons in the cortex may respond differently to early demands than neurons in the striatum (33). It remains speculative which mechanisms are responsible for these differences (33). On the other hand, Murphy and Corbett (11) emphasized in their review that several animal studies indicate that a critical period of heightened neuroplasticity may exist after stroke. Many of the genes and proteins those are important for neuronal growth, synaptogenesis and the proliferation of dendritic spines are expressed at their highest levels during first days to weeks after stroke (11). A better understanding of the mechanisms responsible for upper limb recovery, as well as the optimal time windows in which these mechanisms function is a prerequisite to improve our knowledge about intervention effects on upper limb recovery and the optimal timing for intervention during the acute or sub-acute phase after stroke (34). Therefore, future RCTs on (m)CIMT should not only investigate clinical effects but should also simultaneously explore the time-dependent macroscopic changes observed by using noninvasive techniques such as transcranial magnetic stimulation and functional magnetic resonance imaging as a reflection of neuroplasticity (35).
The present systematic review was subject to some limitations. First, the number of studies was small, preventing of a thorough sensitivity analysis to investigate the impact of (m)CIMT dosage on functional outcome. For now, we were only able to explore the differential effects by making a distinction between HI CIMT and LO CIMT, using forest plots. Second, we cannot rule out publication bias. In particular, small RCTs with negative, nonsignificant or inconclusive results are less likely to be submitted or accepted for publication in the literature.
In summary, the current review suggests that LO CIMT may be more beneficial during the acute or sub-acute phase than HI CIMT. However, because of the relatively small number of heterogeneous studies caution is required in the interpretation of the results. More research is needed, focusing on the mechanisms responsible for upper limb recovery and the optimal time windows for intervention. Currently, a single-blind randomized clinical trial is being conducted in the Netherlands (34). One of the main aims of this multicenter trial, under the acronym ‘EXPLICIT-stroke’ (Explaining PLastICITy after stroke) is to determine the effectiveness of a form of early applied mCIMT on stroke recovery mechanisms that is neuroplasticity, compensatory movements and upper limb neuromechanics.
Footnotes
Acknowledgements
The authors would like to thank Hans Ket for his cooperation in the literature search. This study was funded by the ‘Wetenschappelijk College Fysiotherapie’ (WCF: number 450239) of the Royal Dutch Society for Physical Therapy (KNGF), the Netherlands and cofinanced by the EXPLICIT-stroke program (![]() ) of ZonMw (grant number 89000001).
) of ZonMw (grant number 89000001).